ABSENCE FROM CLINICAL PRACTICUM Student Name:

ABSENCE FROM CLINICAL PRACTICUM
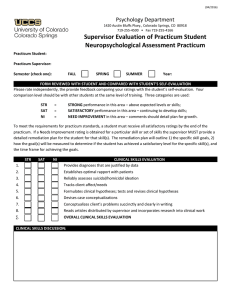
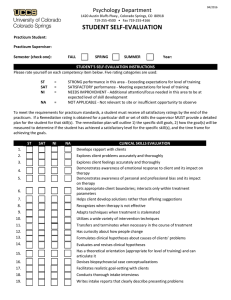
Please complete the information below, describing your absence.
Student Name:
Site:
Date of Absence:
Reason for Absence:
Days Missed at site:
Proposed Make Up Date:
________________________________ _________________
Clinical Supervisor Date
The Clinical Supervisor’s signature above indicates his or her permission to be absent or his or her knowledge of this absence from the site.
ABSENCE FROM CLINICAL PRACTICUM
Please complete the information below, describing your absence.
Student Name:
Site:
Date of Absence:
Reason for Absence:
Days Missed at site:
Proposed Make Up Date:
________________________________ _________________
Clinical Supervisor Date
The Clinical Supervisor’s signature above indicates his or her permission to be absent or his or her knowledge of this absence from the site.
ABSENCE FROM CLINICAL PRACTICUM
Please complete the information below, describing your absence.
Student Name:
Site:
Date of Absence:
Reason for Absence:
Proposed Make Up Date:
Days Missed at site:
________________________________ _________________
Clinical Supervisor Date
The Clinical Supervisor’s signature above indicates his or her permission to be absent or his or her knowledge of this absence from the site.