International comparison

World Health
Organization
INTERNATIONAL COMPARISON OF
SOUTH AFRICAN PRIVATE HOSPITAL
PRICE LEVELS
Francesca Colombo, Head of Health Division, OECD
Luca Lorenzoni, Economist, OECD
Tomas Roubal, Health Economist, WHO South Africa
Sarah L Barber, WHO Representative, South Africa
1
30
25
20
15
10
5
0
45
40
35
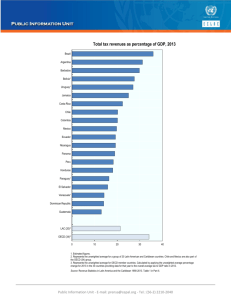
Why are South African private hospital prices a public policy concern?
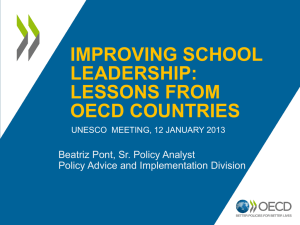
South Africa spends a higher share of its total health expenditures on private voluntary health insurance (41.8%) than any country globally – >6x OECD average (6.3%) – even though it only serves 16% of the population. This is equivalent to 3.7% of South Africa’s GDP.
Source: OECD health data 2015, data for 2013 or latest year available
2
Figure 1. Private health insurance as a share of total current health expenditures (%), 2013
Private voluntary health insurance (PVHI) in OECD countries tends to fill in the gap above public cover- unlike in South Africa where medical schemes mainly finance an alternative to the public sector.
Country
South Africa
USA
Chile
Ireland
France
Canada
Israel
Germany
Australia
New Zealand
Portugal
Spain
UK
Italy
PVHI as % of Total health spending
41.8
34.9
20.0
13.4
13.9
13.2
10.7
9.3
% pop covered by PVHI
16
52.5
18.3
44.6
95
67
82.9
11.0/22.0
8.9
4.9
5.3
4.4
3.4
1.0
54.9/47
29.7
21.1
12.5
10.6
15
Type of coverage
Duplicate, supplementary
Primary
Primary
Duplicate
Complementary
Supplementary
Supplementary
Primary/complementary
Supplementary/duplicate
Duplicate
Duplicate
Duplicate
Duplicate
Complementary
Source: OECD, Health at a Glance 2015; WHO, Global Health Expenditure Database.
Countries with private voluntary health insurance that offer duplicative cover spend much less on PVHI (3.4-13.4% of total health expenditure). 3
OECD countries have measures in place to cap, set or benchmark prices that RSA lacks
• OECD: public sector tends to have some form of price setting for specialist and hospital services, and this provides benchmarks for the private sector. South Africa lacks these price setting measures.
• For OECD countries, prices in the private sector are set using these benchmarks. This has been used as a means to contract/purchase private services to expand access.
• Without these measures in South Africa, negotiations between a handful of medical scheme administrators and private hospitals and specialists determine how a large section of the country’s funds for health are spent (3.7%
GDP).
4
World Health
Organization
Objectives of the study
• Compare private hospital price levels in South
Africa with OECD countries.
• Examine correlations between a country’s income and hospital prices.
• Estimate affordability of hospital services in comparison with general goods and services.
• Using South African data, assess the factors influencing private hospital prices: volume and components of the price (hospitals, specialists, pathology, radiology)
5
World Health
Organization
Methods (1)
• Cross-country price comparison requires standard units, definitions, and ways of measurement that can be applied uniformly across all countries to ensure comparison of “Like with Like.”
• Approach applied and validated in OECD countries: OECD Eurostat
Purchasing Power Parities (PPPs) project. The PPP project identified
28 case types as a sample of hospital services that are the most common services appropriate for international comparison.
– 7 medical services
– 21 surgical services
6
World Health
Organization
Methods (2)
• These are services that are typically covered under the public basket, paid for through government contracting – regardless of whether they are delivered through public or privatelyowned facilities.
• Prices reported represent the total price paid for each case type, including capital
• We also collected information on the number of admissions and average length of stay per case type
• South Africa collected information on the following price components: hospitals, specialists, pathology, radiology.
7
World Health
Organization
Methods (3)
South Africa
• Data from several large medical schemes from 2011-2013 – representing 59.4 % of members and total of 625,940 cases
OECD countries
• Used existing data already collected using same methodology for comparison (Purchasing Power Parities project) for representative sample
• 20 countries: Austria, Czech Republic, Estonia, Finland, France, Germany,
Hungary, Iceland, Ireland, Italy, Luxembourg, Netherlands, Norway, Poland,
Portugal, Slovenia, Spain, Sweden, Switzerland and United Kingdom
• Lower income subset of 7 countries with GDP per capita level closer to
South Africa: Czech Republic, Estonia, Hungary, Poland, Portugal, Spain and
Slovenia
8
World Health
Organization
Methods (4)
South Africa – data from medical schemes
• Insight Actuaries South Africa and other experts from medical scheme administrators worked with OECD to adapt the methodology
• Methodology was tested on the data from Government Employees
Medical Scheme (GEMS)
• Several medical schemes shared their data including GEMS,
Medscheme Holdings (Pty) Ltd, Bonitas Medical Fund
• Preliminary results were presented to and discussed with data providers and some adjustments were made to improve on the accuracy of the findings
• These organizations generously gave their time and expertise to this study, and openly shared their data. We thank them!
9
World Health
Organization
Methods (5)
Prices expressed in Purchasing Power Parities (PPPs)
• Convert different currencies to a common currency and uniform price level
• Equalize purchasing power across countries
• Enables cross-country comparison of prices
10
World Health
Organization
Methods (6)
Results are reported as comparative price levels
• Average for comparison group is calculated as the geometric mean of the comparative price levels across all countries included in the comparison group, and is then set equal to 100.
• Each country’s comparative price level is then expressed in relation to the mean of 100. Results should be interpreted looking at the relative positions of countries rather than looking at absolute levels.
Exchange rates fluctuations are captured in both the CPI and hospital prices.
11
World Health
Organization
Presentation of
Results
South African prices by case type
• Prices in Rand by case type, 2011-13
• Increases in prices over time
Cross country comparison
• Correlations between hospital price levels and income
• Comparison of hospital price levels across countries
• Affordability of hospital prices relative to other goods and services
What is driving South African prices?
• Length of stay and admissions
• Components of the price: hospitals, specialist, pathology
12
Case type
M01 Acute Myocardial Infarction
M02 Angina Pectoris
M03 Cholelitiasis
M04 Heart Failure
M05 Malignant Neoplasm of Bronchus and Lung
M06 Normal Deliveries
M07 Pneumonia
S01 Appendectomy
S02 Caesarean section
S03 Cholecystectomy
S04 Colorectal resection
S05 Coronary artery bypass graft
S06 Discectomy
S07 Endarterectomy
S08 Hip replacement: total and partial
S09 Hysterectomy: abdominal or vaginal
S10 Knee replacement
S11 Mastectomy
S12 Open prostatectomy
S13 Percutaneous transluminal coronary angioplasty
S14 Peripheral vascular bypass
S15 Repair of inguinal hernia
S16 Thyroidectomy
S17 Transurethral resection of prostate
S18 Arthroscopic excision of meniscus of knee
S19 Lens and cataract procedures
S20 Litigation and stripping of varicose veins - lower limb
S21 Tonsillectomy and/or adenoidectomy
S18 Arthroscopic excision of meniscus of knee
S19 Lens and cataract procedures
S20 Litigation and stripping of varicose veins - lower limb
S21 Tonsillectomy and/or adenoidectomy
Average price (in Rand) and average annual rate of change by case type: 7 medical cases studied
Year
2011 2012 2013
56,726 59,038 64,308
25,729 27,562 29,445
11,954 13,788 14,639
25,325 27,168 28,959
24,147 25,651 26,412
16,251 17,056 17,954
17,002 18,359 19,731
23,448 25,725 27,836
27,802 29,915 31,912
34,390 36,753 39,071
95,850 99,863 103,543
220,344 237,497 253,901
80,847 83,851 87,977
69,901 73,993 82,917
111,210 116,976 120,758
29,108 31,616 34,432
105,536 110,801 114,044
31,427 33,944 37,437
68,556 73,683 76,645
88,827 93,466 101,689
95,008 94,889 106,260
20,428 21,704 23,857
29,204 31,907 34,623
29,176 31,500 33,196
21,002 22,974 24,748
19,367 20,464 21,633
21,060 22,122 24,275
10,044 10,853 11,442
17,279 18,152 19,497
18,520 19,299 20,115
12,277 14,518 16,144
7,957 8,341 8,822
Annual rate of change (%)
6.5
13
7.0
10.7
6.9
4.6
5.1
7.7
9.0
7.1
6.6
3.9
7.3
4.3
8.9
4.2
8.8
4.0
9.1
5.7
7.0
5.8
8.1
8.9
6.7
8.6
5.7
7.4
6.7
6.2
4.2
14.7
5.3
Year
Annual rate of
Case type 2011 2012 2013 change (%) Average price (in Rand) and average annual rate of
6.5
M02 Angina Pectoris
M03 Cholelitiasis
25,729
11,954
27,562
13,788
29,445
14,639
7.0
10.7
M04 Heart Failure
M05 Malignant Neoplasm of Bronchus and Lung
M06 Normal Deliveries
M07 Pneumonia
Case type
25,325
24,147 25,651
28,959
26,412
6.9
4.6
Annual rate of change (%) 7.7
S02 Caesarean section
M02 Angina Pectoris
17,002 18,359 19,731
56,726 59,038 64,308
27,802
25,729
29,915
27,562
31,912
29,445
11,954 13,788 14,639
7.1
7.0
S06 Discectomy
M05 Malignant Neoplasm of Bronchus and Lung
S10 Knee replacement
S01 Appendectomy
S14 Peripheral vascular bypass
S04 Colorectal resection
S18 Arthroscopic excision of meniscus of knee
S07 Endarterectomy
S18 Arthroscopic excision of meniscus of knee
S10 Knee replacement
S13 Percutaneous transluminal coronary angioplasty
S14 Peripheral vascular bypass
S15 Repair of inguinal hernia
S16 Thyroidectomy
S17 Transurethral resection of prostate
S18 Arthroscopic excision of meniscus of knee
S19 Lens and cataract procedures
S20 Litigation and stripping of varicose veins - lower limb
S21 Tonsillectomy and/or adenoidectomy
S18 Arthroscopic excision of meniscus of knee
S19 Lens and cataract procedures
S20 Litigation and stripping of varicose veins - lower limb
S21 Tonsillectomy and/or adenoidectomy
25,325 27,168 28,959
80,847
24,147
83,851
25,651
87,977
26,412
16,251 17,056 17,954
17,002 18,359 19,731
105,536 110,801 114,044
23,448 25,725 27,836
27,802 29,915 31,912
34,390 36,753 39,071
95,008
95,850
94,889 106,260
99,863 103,543
220,344 237,497 253,901
80,847 83,851 87,977
21,002
69,901
22,974
73,993
24,748
82,917
111,210 116,976 120,758
29,108 31,616 34,432
17,279
105,536
18,152
110,801
19,497
114,044
31,427 33,944 37,437
68,556 73,683 76,645
88,827 93,466 101,689
95,008 94,889 106,260
20,428 21,704 23,857
29,204 31,907 34,623
29,176 31,500 33,196
21,002 22,974 24,748
19,367 20,464 21,633
21,060 22,122 24,275
10,044 10,853 11,442
17,279 18,152 19,497
18,520 19,299 20,115
12,277 14,518 16,144
7,957 8,341 8,822
14
4.3
4.6
4.0
9.0
5.8
3.9
8.6
8.9
6.2
4.0
7.0
5.8
8.1
8.9
6.7
8.6
5.7
7.4
6.7
6.2
4.2
14.7
5.3
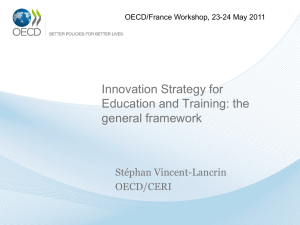
Private hospital prices in South Africa increased over time (6.2-6.8%), which is higher than the price increase for other goods/services (CPI: 5.6% and 5.7%)
CPI index
Private hospitals, average
6,2
6,8
Surgical
6
6,9
2013/2012
2012/2011
Medical
7
7,1
0 1 2 3 4 5 6 7 8
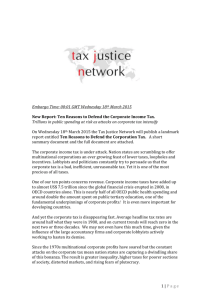
Strong correlation (r=0.82) between country’s income (GDP) and hospital prices – but South Africa is the outlier
Each country’s comparative price level is expressed relative to the mean of 100.
South Africa’s prices are on par with France, UK, Germany
– countries with much higher income levels. 16
South Africa has the lowest GDP per capita and a price level for private hospitals comparable to the average observed across OECD countries
Private hospitals are charging high-prices for their services in an environment where other goods and services are delivered at lower cost.
17
South African economy wide price level represents 53% of OECD average in 2013: but private hospital prices are comparable or higher than OECD averages
Consistent over three years
100 = OECD mean
OECD average
South Africa average
GDP per capita (in US$ PPPs)
40,169
12,144
40,700
12,555
41,224
12,891
18
For lower GDP subset: South African economy wide price level is 74% of the subset average; but private hospital prices approximately double the subset average
100=OECD subset mean
Comparative Price and GDP Levels
South Africa sample
Medical services
Surgical services
Total
2011
174
207
195
2012
168
201
189
2013
161
211
192
Gross Domestic
Product
Subset of 7 lower income OECD countries on average
South Africa average
85 86 74
GDP per capita (in US$ PPPs)
26,404
12,144
26,702
12,555
27,323
12,891
19
South Africa private hospital prices rank as least affordable in comparison with other countries
…because there is the largest difference between hospital price levels and general price levels – i.e., prices of food, clothing and other common goods
20
Within South Africa, private hospital prices are likely to be expensive for 90% of South Africans
- even for people with higher incomes
Hospital comparative price levels and household consumption expenditure pc
(US$PPP), including South Africa’s high income populations (expenditure deciles 7-10)
21
World Health
Organization
What is driving prices?
• Volume
– Length of stay
– Number of Admissions
• Unit price components dedicated to:
– Specialists
– Pathology
– Hospitals
– Radiology
• Other factors
– Organization of care (supply)
– Patient preferences (demand)
22
Average length of stay in private hospitals in South
Africa (3.3 days) is lower than OECD average (4.7 days)
23
5
4
3
2
1
-
7
6
8-41% lower average length of stay across all medical and surgical cases studied
41%
39%
37%
31% 29%
27%
24%
45%
40%
35%
30%
25%
20%
15%
10%
5%
0%
South Africa OECD average difference in %
24
No changes in overall admission rates on average in the South African sample between
2011-13 …
45
40
35
30
Admissions increased in line with the increase in medical scheme membership by 12% between 2011-13.
Rate per
1000
25
Beneficiaries
20
15
10
5
0
42,1
42,4
42,2
38,2
38,0
37,6
2011
2012
2013
25
But the structure of admissions changed – with increases mostly in selected surgical cases (2011-13).
.
Surgical inpatient cases increased by 16%
All but 2 medical case admissions increased by 25%
Large increases in hip and knee replacements (31% and 53%)
6000
5000
4000
3000
2000
1000
0
5,7%
Appendectomy
2011
7,5% 31,9%
53,7%
Repair of inguinal hernia
2013
Hip replacement
2011-2013 increase
Knee replacement increase in membership
26
50%
40%
30%
20%
10%
0%
Relatively high admission rates for some services with standardized age/sex rates in comparison with
OECD countries
Hospital utilisation rates per 100,000, South African sample and OECD countries:
Hysterectomy
27
Hospital component accounts for the largest share of prices for both medical (40-52%) and surgical cases (49-62%)
Angina
Pectoris
Pneumonia
50%
40%
30%
20%
10%
0%
Acute
Myocardial
Infarction
Neoplasm of bronchus
• Pathology: 21 – 35 %
• Specialists: 13 – 19 %
Heart Failure
Cholelitiasis
Specialists
Radiology
Hospital
28
But the share of the price devoted to specialists increased over time, and comprises 14%–29%
Changes in share of price for specialist fees, medical cases, 2011-2013
Acute Myocardial
Infarction
20%
Pneumonia
18%
16%
14%
12%
10%
Angina Pectoris
2011
2012
2013
Malignant Neoplasm of Bronch
Cholelitiasis
29
Heart Failure
World Health
Organization
In summary…
Strengths of the study
• Transparent and reproducible methodology, which was tested and validated on medical scheme data
• Hospital cases comparable, clearly defined and representative of hospital production
• Price estimate based on payment from purchaser
– In OECD countries public purchaser’s price was used as they pay the same to public and private hospitals
– This enabled us to compare private hospitals in South
Africa with public/private hospitals in OECD countries
• All costs included (specialists, nursing, pharma, pathology, investment)
• When comparing prices, PPPs convert currency into common currency and eliminate differences in price levels between countries.
30
World Health
Organization Limitations
• Comparison done with countries for which data are available from the OECD-EUROSTAT project for 2011-2013
• No data on cost components of hospitals and specialists for comparator countries
• Cannot determine what is behind large share of price devoted to hospitals
• No data on individual medical scheme prices
• No information on the market structure/power and its impact on prices
31
World Health
Organization
Conclusion 1:
Prices are high and increasing.
• South Africa’s private hospital prices are expensive relative to what could be predicted given the country’s wealth.
• Prices are increasing over time above the rate of inflation, or at a higher rate than other goods and services in the economy.
32
World Health
Organization
Conclusion 2:
Prices are not affordable for most South Africans.
• South Africa data demonstrate the greatest difference between private hospital price level and general prices level among all countries in the sample.
• Thus South Africa’s private hospital price level is ranked as the least affordable among all countries analysed.
• Prices are also likely to be expensive for 90% of
South Africans.
33
World Health
Organization
Conclusion 3:
Unusually low lengths of stay probably result from cost-control efforts
.
Low ALOS are likely related to the financing and organization of care
--weak/no controls over admissions given that specialists work independently in hospitals.
-- including cost control measures by medical scheme administrators, i.e., pre-authorized length of stay
Impact on quality of care and health outcomes are a concern and should be evaluated in the future.
34
World Health
Organization
Conclusion 4:
Large increases in high volume surgical procedures cannot be fully explained by changes in membership
.
• Planned surgical procedures, i.e., hip and knee replacements increased by 31% and 53% over a very short time (2011-13).
• These changes cannot be fully explained by the 12% increase in medical scheme membership (2011-13)
• They also cannot be fully explained by aging population or other external factors.
• They are likely driven by supplier induced demand.
35
World Health
Organization
Conclusion 5:
Hospital share is the main component of the price, but specialists fees are driving the increase.
• Hospitals are the main component of prices (40-62%) for both medical and surgical cases.
• The increase in the prices observed in this study however, were driven by the increase specialists fees.
• This has implications for the health system as a whole and access to services.
36
World Health
Organization Conclusion 6:
The high prices in private health sector spill over to the health system and economy as a whole.
• Given the magnitude of private voluntary health insurance spending
(3.7% GDP), market interactions between medical schemes and private health care providers spills over to the whole health system.
• Prices set in the private sector set labour market benchmarks that specialists face in choosing between working in public/private facility.
• High private prices restrict the ability of the government to use private services to achieve universal health coverage under National
Health Insurance (NHI).
• Increases in prices are passed on as increases in premiums to members and employers – which can then lead to individuals bearing the burden (i.e., higher co-payments, reduced benefits)
37
World Health
Organization
Conclusion 7:
The current ways in which the private sector controls prices are not effective.
• High and increasing prices suggest that current methods of controlling private hospital prices are not effective in curbing price inflation.
• Other OECD countries have measures to prescribe, cap or benchmark prices that South Africa lacks.
This study suggests that efforts to control prices while ensuring accessibility and quality are needed, which could help individual
South Africans and the country at large get more value from their considerable spending on health care.
38
World Health
Organization
Thank you!
International Comparison of South African Private Hospitals Price Levels; OECD
Working Paper No. 85. DELSA/HEA/WD/HWP(2015)85. Available at http://www.oecd.org/health/workingpapers
Contact: WHO Representative Office in South Africa afwcozawr@who.int
39