Introduction to Biostatistics for Clinical
advertisement

Introduction to Biostatistics
for Clinical and Translational
Researchers
KUMC Departments of Biostatistics & Internal Medicine
University of Kansas Cancer Center
FRONTIERS: The Heartland Institute of Clinical and Translational Research
Course Information
Jo A. Wick, PhD
Office Location: 5028 Robinson
Email: jwick@kumc.edu
Lectures are recorded and posted at
http://biostatistics.kumc.edu under ‘Educational
Opportunities’
Hypothesis Testing
Continued
Inferences on Time-to-Event
Survival Analysis is the class of statistical
methods for studying the occurrence (categorical)
and timing (continuous) of events.
The event could be
development of a disease
response to treatment
relapse
death
Survival analysis methods are most often applied
to the study of deaths.
Inferences on Time-to-Event
Survival Time: the time from a well-defined point in
time (time origin) to the occurrence of a given
event.
Survival data includes:
a time
an event ‘status’
any other relevant subject characteristics
Inferences on Time-to-Event
In most clinical studies the length of study period is
fixed and the patients enter the study at different
times.
Lost-to-follow-up patients’ survival times are measured
from the study entry until last contact (censored
observations).
Patients still alive at the termination date will have
survival times equal to the time from the study entry until
study termination (censored observations).
When there are no censored survival times, the set
is said to be complete.
Functions of Survival Time
Let T = the length of time until a subject
experiences the event.
The distribution of T can be described by several
functions:
Survival Function: the probability that an individual
survives longer than some time, t:
S(t) = P(an individual survives longer than t)
= P(T > t)
Functions of Survival Time
If there are no censored observations, the survival
function is estimated as the proportion of patients
surviving longer than time t:
# of patients surviving longer than t
Sˆ (t ) =
total # of patients
Functions of Survival Time
Density Function: The survival time T has a
probability density function defined as the limit of
the probability that an individual experiences the
event in the short interval (t, t + t) per unit width
t:
P an individual dying in the interval (t, t + t )
f (t ) = lim
t 0
t
Functions of Survival Time
Survival density function:
Functions of Survival Time
If there are no censored observations, f(t) is
estimated as the proportion of patients
experiencing the event in an interval per unit width:
# of patients dying in the interval beginning at time t
fˆ(t )
total # of patients interval width
The density function is also known as the
unconditional failure rate.
Functions of Survival Time
Hazard Function: The hazard function h(t) of
survival time T gives the conditional failure rate.
It is defined as the probability of failure during a
very small time interval, assuming the individual
has survived to the beginning of the interval:
P an individual of age t fails in the time interval (t , t + t )
h(t ) lim
t 0
t
Functions of Survival Time
The hazard is also known as the instantaneous
failure rate, force of mortality, conditional mortality
rate, or age-specific failure rate.
The hazard at any time t corresponds to the risk of
event occurrence at time t:
For example, a patient’s hazard for contracting influenza
is 0.015 with time measured in months.
What does this mean? This patient would expect to
contract influenza 0.015 times over the course of a month
assuming the hazard stays constant.
Functions of Survival Time
If there are no censored observations, the hazard
function is estimated as the proportion of patients
dying in an interval per unit time, given that they
have survived to the beginning of the interval:
# of patients dying in the interval beginning at time t
hˆ(t ) =
# of patients surviving at t interval width
=
# of patients dying per unit time in the interval
# of patients surviving at t
Estimation of S(t)
Product-Limit Estimates (Kaplan-Meier): most
widely used in biological and medical applications
Life Table Analysis (actuarial method): appropriate
for large number of observations or if there are
many unique event times
Methods for Comparing S(t)
If your question looks like: “Is the time-to-event
different in group A than in group B (or C . . . )?”
then you have several options, including:
Log-rank Test: weights effects over the entire observation
equally—best when difference is constant over time
Weighted log-rank tests:
• Wilcoxon Test: gives higher weights to earlier effects—better for
detecting short-term differences in survival
• Tarome-Ware: a compromise between log-rank and Wilcoxon
• Peto-Prentice: gives higher weights to earlier events
• Fleming-Harrington: flexible weighting method
Inferences for Time-to-Event
Example: survival in squamous cell carcinoma
A pilot study was conducted to compare
Accelerated Fractionation Radiation Therapy
versus Standard Fractionation Radiation Therapy
for patients with advanced unresectable squamous
cell carcinoma of the head and neck.
The researchers are interested in exploring any
differences in survival between the patients treated
with Accelerated FRT and the patients treated with
Standard FRT.
Inferences for Time-to-Event
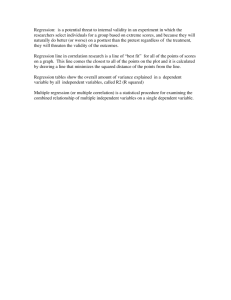
H0: S1(t) = S2(t) for all t
Overall Survival by Treatment
H1: S1(t) ≠ S2(t) for at least one t
1.00
AFRT
SFRT
Survival Probability
0.75
0.50
0.25
0.00
0
12
24
36
48
60
72
Survival Time (months)
84
96
108
120
Squamous Cell Carcinoma
Gender
Male
Female
Age
Median
Range
Primary Site
Larynx
Oral Cavity
Pharynx
Salivary Glands
Stage
III
IV
Tumor Stage
T2
T3
T4
AFRT
SFRT
28 (97%)
1 (3%)
16 (100%)
0
61
30-71
65
43-78
3 (10%)
6 (21%)
20 (69%)
0
4 (25%)
1 (6%)
10 (63%)
1 (6%)
4 (14%)
25 (86%)
8 (50%)
8 (50%)
3 (10%)
8 (28%)
18 (62%)
2 (12%)
7 (44%)
7 (44%)
Squamous Cell Carcinoma
Median Survival Time:
AFRT: 18.38 months (2 censored)
SFRT: 13.19 months (5 censored)
Overall Survival by Treatment
1.00
AFRT
SFRT
Survival Probability
0.75
0.50
0.25
0.00
0
12
24
36
48
60
72
Survival Time (months)
84
96
108
120
Squamous Cell Carcinoma
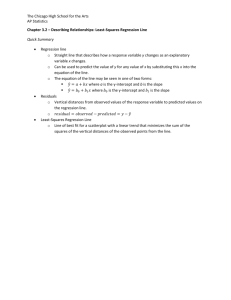
Overall Survival by Treatment
Log-Rank1.00
test p-value= 0.5421
AFRT
SFRT
Survival Probability
0.75
0.50
0.25
0.00
0
12
24
36
48
60
72
Survival Time (months)
84
96
108
120
Squamous Cell Carcinoma
Staging of disease is also prognostic for survival.
Shouldn’t we consider the analysis of the survival
of these patients by stage as well as by treatment?
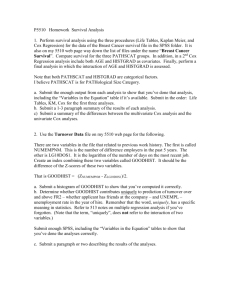
Squamous Cell Carcinoma
Overall Survival by Treatment and Stage
1.00
AFRT/Stage 3
AFRT/Stage 4
SFRT/Stage 3
SFRT/Stage 4
Median Survival Time:
AFRT Stage 3: 77.98 mo.
AFRT Stage 4: 16.21 mo.
SFRT Stage 3: 19.34 mo.
SFRT Stage 4: 8.82 mo.
Survival Probability
0.75
0.50
0.25
0.00
0
12
24
36
48
60
72
Survival Time (Months)
Log-Rank test p-value = 0.0792
84
96
108
120
Inferences on Time-to-Event
Concerns a response that is both categorical
(event?) and continuous (time)
There are several nonparametric methods that can
be used—choice should be based on whether you
anticipate a short-term or long-term benefit.
Log-rank test is optimal when the survival curves
are approximately parallel.
Weight functions should be chosen based on
clinical knowledge and should be pre-specified.
What about adjustments?
There may be other predictors or explanatory
variables that you believe are related to the
response other than the actual factor (treatment) of
interest.
Regression methods will allow you to incorporate
these factors into the test of a treatment effect:
Logistic regression: when y is categorical and nominal
binary
Multinomial logistic regression: when y is categorical
with more than 2 nominal categories
Ordinal logistic regression: when y is categorical and
ordinal
What about adjustments?
There may be other predictors or explanatory
variables that you believe are related to the
response other than the actual factor (treatment) of
interest.
Regression methods will allow you to incorporate
these factors into the test of a treatment effect:
Linear regression: when y is continuous and the factors
are a combination of categorical and continuous (or just
continuous)
Two- and three-way ANOVA: when y is continuous and
the factors are all categorical
What about adjustments?
There may be other predictors or explanatory
variables that you believe are related to the
response other than the actual factor (treatment) of
interest.
Regression methods will allow you to incorporate
these factors into the test of a treatment effect:
Cox regression: when y is a time-to-event outcome
Linear Regression
The relationship between two variables may be
one of functional dependence—that is, the
magnitude of one of the variables (dependent) is
assumed to be determined by the magnitude of the
second (independent), whereas the reverse is not
true.
Blood pressure and age
Dependent does not equate to ‘caused by’
Linear Regression
In it’s most basic form, linear regression is a
probabilistic model that accounts for unexplained
variation in the relationship between two variables:
y = Deterministic Component + Random Error
= mx + b + ε
= β0 + β1x + ε
This model is referred to as simple linear
regression.
10
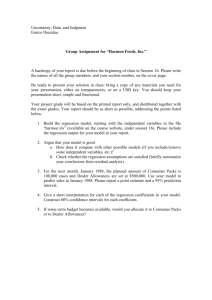
Simple Linear Regression
yy ==0.78
0 +1x+ +
0.89
0 x+ε
8
y = β0 + β1x + ε
4
y
6
y response variable
x explanatory variable
β0 intercept
2
β1 slope
0
ε 'error'
0
2
4
6
x
8
10
Arm Circumference and Height
Data on anthropomorphic measures from a
random sample of 150 Nepali children up to 12
months old
What is the relationship between average arm
circumference and height?
Data:
Arm circumference: x = 12.4cm
Height: x = 61.6cm
s = 1.5cm
R = (7.3cm,15.6cm)
s = 6.3cm
R = (40.9cm,73.3cm)
Arm Circumference and Height
Treat height as continuous when estimating the
relationship
Linear regression is a potential option--it allows us
to associate a continuous outcome with a
continuous predictor via a linear relationship
The line estimates the mean value of the outcome for
each continuous value of height in the sample used
Makes a lot of sense, but only if a line reasonably
describes the relationship
Visualizing the Relationship
Scatterplot
Visualizing the Relationship
Does a line reasonably describe the general shape
of the relationship?
We can estimate a line using a statistical software
package
The line we estimate will be of the form:
ŷ = β0 + β1x
Here,ŷ is the average arm circumference for a
group of children all of the same height, x
Arm Circumference and Height
Arm Circumference and Height
Arm Circumference and Height
How do we interpret the estimated slope?
The average change in arm circumference for a one-unit
(1 cm) increase in height
The mean difference in arm circumference for two groups
of children who differ by one unit (1 cm) in height
These results estimate that the mean difference in
arm circumferences for a one centimeter difference
in height is 0.16 cm, with taller children having
greater average arm circumference
Arm Circumference and Height
What is the estimated mean difference in arm
circumference for children 60 cm versus 50 cm
tall?
Arm Circumference and Height
Our regression results only apply to the range of
observed data
Arm Circumference and Height
How do we interpret the estimated intercept?
The estimated y when x = 0--the estimated mean arm
circumference for children 0 cm tall.
Does this make sense given our sample?
Frequently, the scientific interpretation of the
intercept is meaningless.
It is necessary for fully specifying the equation of a
line.
Arm Circumference and Height
X = 0 isn’t even on the graph
Inferences using Linear
Regression
H0: β1 = 0 versus
H1: β1 > 0 (strong positive linear relationship)
or H1: β1 < 0 (strong negative linear relationship)
or H1: β1 ≠ 0 (strong linear relationship)
Test statistic: t (df = n – 2)
ˆ 1
t
sˆ
1
x x y y
i
i
s
xi x
xi x
2
2
Notes
Linear regression performed with a single predictor
(one x) is called simple linear regression.
Correlation is a measure of the strength of the linear
relationship between two continuous outcomes.
Linear regression with more than one predictor is
called multiple linear regression.
y = β0 + β1x1 + β1x1 +
+ βk xk + ε
Multiple Linear Regression
For the ith x:
H0: βi = 0
H1: βi ≠ 0
Test statistic: t (df = 1)
For all x:
H0: βi = 0 for all i
H1: βi ≠ 0 for at least one i
Test statistic: F (df1 = k, df2 = n – (k + 1))
Multiple Linear Regression
How do we interpret the estimate of βi?
βi is called a partial regression coefficient and can be
thought of as conditional slope—it is the rate of change of
y for every unit change in xi if all other x’s are held
constant.
It is sometimes said that βi is a measure of the
relationship between y and xi after ‘controlling for’ the
remaining x’s—that is, it is a measure of the extent to
which y is related to xi after removing the effects of the
other x’s.
Regression Plane
With one predictor, the relationship is described by
a line.
With two predictors, the relationship is estimated
by a plane in 3D.
Linear Correlation
Linear regression assumes the linear dependence
of one variable y (dependent) on a second variable
x (independent).
Linear correlation also considers the linear
relationship between two continuous outcomes but
neither is assumed to be functionally dependent
upon the other.
Interest is primarily in the strength of association, not in
describing the actual relationship.
Scatterplot
48
Correlation
Pearson’s Correlation Coefficient is used to
quantify the strength.
r
x x y y
x x y y
2
2
Note: If sample size is small or data is non-normal,
use non-parametric Spearman’s coefficent.
49
Correlation
r>0
r<0
r=0
Business Statistics, 4e, by Ken Black. © 2003 John Wiley & Sons.
3-56
Inferences on Correlation
H0: ρ = 0 (no linear association) versus
H1: ρ > 0 (strong positive linear relationship)
or H1: ρ < 0 (strong negative linear relationship)
or H1: ρ ≠ 0 (strong linear relationship)
Test statistic: t (df = 2)
Correlation
52
Correlation
* Excluding France
53
Logistic Regression
When you are interested in describing the relationship
between a dichotomous (categorical, nominal)
outcome and a predictor x, logistic regression is
appropriate.
ln
= β0 + β1x + ε
1
Pr y = 1
Conceptually, the method is the same as linear
regression MINUS the assumption of y being
continuous.
Logistic Regression
Interpretation of regression coefficients is not
straight-forward since they describe the
relationship between x and the log-odds of y = 1.
We often use odds ratios to determine the
relationship between x and y.
Death
A logistic regression model was used to describe
the relationship between treatment and death:
Y = {died, alive}
X = {intervention, standard of care}
ln
= β0 + β1x + ε
1
Pr y = death
if intervention
1
x=
2 if standard of care
Death
β1 was estimated to be 0.69. What does this
mean?
If you exponentiate the estimate, you get the odds ratio
relating treatment to the probability of death!
exp(0.69) = 0.5—when treatment involves the
intervention, the odds of dying decrease by 50% (relative
to standard of care).
Notice the negative sign—also indicates a decrease in
the chances of death, but difficult to interpret without
transformation.
Death
β1 was estimated to be 0.41. What does this
mean?
If you exponentiate the estimate, you get the odds ratio
relating treatment to the probability of death!
exp(0.41) = 1.5—when treatment involves the
intervention, the odds of dying increase by 50% (relative
to standard of care).
Notice the positive sign—also indicates an increase in the
chances of death, but difficult to interpret without
transformation.
Logistic Regression
What about when x is continuous?
Suppose x is age and y is still representative of
death during the study period.
ln
= β0 + β1x + ε
1
Pr y = death
x = baseline age in years
Death
β1 was estimated to be 0.095. What does this
mean?
If you exponentiate the estimate, you get the odds ratio
relating age to the probability of death!
exp(0.095) = 1.1—for every one-year increase in age, the
odds of dying increase by 10%.
Notice the positive sign—also indicates a decrease in the
chances of death, but difficult to interpret without
transformation.
Multiple Logistic Regression
In the same way that linear regression can
incorporate multiple x’s, logistic regression can
relate a categorical y response to several
independent variables.
Interpretation of partial regression coefficients is
the same.
Cox Regression
Cox regression and logistic regression are very
similar
Both are trying to describe a yes/no outcome
Cox regression also attempts to incorporate the timing of
the outcome in the modeling
Cox vs Logistic Regression
Distinction between rate and proportion:
Incidence (hazard) rate: number of “events” per
population at-risk per unit time (or mortality rate, if
outcome is death)
Cumulative incidence: proportion of “events” that occur
in a given time period
63
Cox vs Logistic Regression
Distinction between hazard ratio and odds ratio:
Hazard ratio: ratio of incidence rates
Odds ratio: ratio of proportions
Logistic regression aims to estimate the odds ratio
Cox regression aims to estimate the hazard ratio
By taking into account the timing of events, more
information is collected than just the binary yes/no.
64
Publication Bias
From: Publication bias: evidence of delayed publication in a cohort study of clinical research projects BMJ 1997;315:640-645 (13 September)
65
Publication Bias
Table 4 Risk factors for time to publication using univariate Cox regression analysis
Characteristic
# not published
# published
Hazard ratio (95% CI)
Null
29
23
1.00
Non-significant
trend
16
4
0.39 (0.13 to 1.12)
Significant
47
99
2.32 (1.47 to 3.66)
From: Publication bias: evidence of delayed publication in a cohort study of clinical research projects BMJ 1997;315:640-645 (13 September)
Interpretation: Significant results have a 2fold higher incidence of publication compared
to null results.
Cox Regression
Cox Regression is what we call semiparametric
Kaplan-Meier is nonparametric
There are also parametric methods which assume the
distribution of survival times follows some type of
probability model (e.g., exponential)
Can accommodate both discrete and continuous
measures of event times.
Can accommodate multiple x’s.
Easy to incorporate time-dependent covariates—
covariates that may change in value over the
course of the observation period
Clinical Trials &
Design of Experiments
Random Samples
The Fundamental Rule of Using Data for
Inference requires the use of random sampling or
random assignment.
Random sampling or random assignment ensures
control over “nuisance” variables.
We can randomly select individuals to ensure that
the population is well-represented.
Equal sampling of males and females
Equal sampling from a range of ages
Equal sampling from a range of BMI, weight, etc.
Random Samples
Randomly assigning subjects to treatment levels to
ensure that the levels differ only by the treatment
administered.
weights
ages
risk factors
Nuisance Variation
Nuisance variation is any undesired sources of
variation that affect the outcome.
Can systematically distort results in a particular
direction—referred to as bias.
Can increase the variability of the outcome being
measured—results in a less powerful test because of too
much ‘noise’ in the data.
Example: Albino Rats
It is hypothesized that exposing albino rats to
microwave radiation will decrease their food
consumption.
Intervention: exposure to radiation
Levels exposure or non-exposure
Levels 0, 20000, 40000, 60000 uW
Measurable outcome: amount of food consumed
Possible nuisance variables: sex, weight,
temperature, previous feeding experiences
Experimental Design
Statistical analysis, no matter how intricate, cannot
rescue a poorly designed study.
No matter how efficient, statistical analysis cannot
be done overnight.
A researcher should plan and state what they are
going to do, do it, and then report those results.
Be transparent!
Experimental Design
Types of data collected in a clinical trial:
Treatment – the patient’s assigned treatment and actual
treatment received
Response – measures of the patient’s response to
treatment including side-effects
Prognostic factors (covariates) – details of the patient’s
initial condition and previous history upon entry into the
trial
Experimental Design
Three basic types of outcome data:
Qualitative – nominal or ordinal, success/failure, CR, PR,
Stable disease, Progression of disease
Quantitative – interval or ratio, raw score, difference,
ratio, %
Time to event – survival or disease-free time, etc.
Experimental Design
Formulate statistical hypotheses that are germane
to the scientific hypothesis.
Determine:
experimental conditions to be used (independent
variable(s))
measurements to be recorded
extraneous conditions to be controlled (nuisance
variables)
Experimental Design
Specify the number of subjects required and the
population from which they will be sampled.
Power, Type I & II errors
Specify the procedure for assigning subjects to the
experimental conditions.
Determine the statistical analysis that will be
performed.
Experimental Design
Considerations:
Does the design permit the calculation of a valid estimate
of treatment effect?
Does the data-collection procedure produce reliable
results?
Does the design possess sufficient power to permit and
adequate test of the hypotheses?
Experimental Design
Considerations:
Does the design provide maximum efficiency within the
constraints imposed by the experimental situation?
Does the experimental procedure conform to accepted
practices and procedures used in the research area?
• Facilitates comparison of findings with the results of other
investigations
Threats to Valid Inference
Statistical Conclusion Validity
• Low statistical power - failing to reject a false hypothesis because
of inadequate sample size, irrelevant sources of variation that are
not controlled, or the use of inefficient test statistics.
• Violated assumptions - test statistics have been derived
conditioned on the truth of certain assumptions. If their tenability is
questionable, incorrect inferences may result.
Many methods are based on approximations to a
normal distribution or another probability
distribution that becomes more accurate as sample
size increases—using these methods for small
sample sizes may produce unreliable results.
Threats to Valid Inference
Statistical Conclusion Validity
Reliability of measures and treatment implementation.
Random variation in the experimental setting and/or
subjects.
• Inflation of variability may result in not rejecting a false hypothesis
(loss of power).
Threats to Valid Inference
Internal Validity
Uncontrolled events - events other than the
administration of treatment that occur between the time
the treatment is assigned and the time the outcome is
measured.
The passing of time - processes not related to treatment
that occur simply as a function of the passage of time that
may affect the outcome.
Threats to Valid Inference
Internal Validity
Instrumentation - changes in the calibration of a
measuring instrument, the use of more than one
instrument, shifts in subjective criteria used by observers,
etc.
• The “John Henry” effect - compensatory rivalry by subjects
receiving less desirable treatments.
• The “placebo” effect - a subject behaves in a manner consistent
with his or her expectations.
Threats to Valid Inference
External Validity—Generalizability
Reactive arrangements - subjects who are aware that
they are being observed may behave differently that
subjects who are not aware.
Interaction of testing and treatment - pretests may
sensitize subjects to a topic and enhance the
effectiveness of a treatment.
Threats to Valid Inference
External Validity—Generalizability
Self-selection - the results may only generalize to
volunteer populations.
Interaction of setting and treatment - results obtained in a
clinical setting may not generalize to the outside world.
Clinical Trials—Purpose
Prevention trials look for more effective/safer
ways to prevent a disease in individuals who have
never had it, or to prevent a disease from recurring
in individuals who have.
Screening trials attempt to identify the best
methods for detecting diseases or health
conditions.
Diagnostic trials are conducted to distinguish
better tests or procedures for diagnosing a
particular disease or condition.
Clinical Trials—Purpose
Treatment trials assess experimental treatments,
new combinations of drugs, or new approaches to
surgery or radiation therapy for efficacy and safety.
Quality of life (supportive care) trials explore
means to improve comfort and quality of life for
individuals with chronic illness.
Classification according to the U.S. National Institutes of Health
Clinical Trials—Phases
Pre-clinical studies involve in vivo and in vitro
testing of promising compounds to obtain
preliminary efficacy, toxicity, and pharmacokinetic
information to assist in making decisions about
future studies in humans.
Clinical Trials—Phases
Phase 0 studies are exploratory, first-in-human
trials, that are designed to establish very early on
whether the drug behaves in human subjects as
was anticipated from preclinical studies.
Typically utilizes N = 10 to 15 subjects to assess
pharmacokinetics and pharmacodynamics.
Allows the go/no-go decision usually made from animal
studies to be based on preliminary human data.
Clinical Trials—Phases
Phase I studies assess the safety, tolerability,
pharmacokinetics, and pharmacodynamics of a
drug in healthy volunteers (industry standard) or
patients (academic/research standard).
Involves dose-escalation studies which attempt to identify
an appropriate therapeutic dose.
Utilizes small samples, typically N = 20 to 80 subjects.
Clinical Trials—Phases
Phase II studies assess the efficacy of the drug
and continue the safety assessments from phase I.
Larger groups are usually used, N = 20 to 300.
Their purpose is to confirm efficacy (i.e., estimation of
effect), not necessarily to compare experimental drug to
placebo or active comparator.
Clinical Trials—Phases
Phase III studies are the definitive assessment of
a drug’s effectiveness and safety in comparison
with the current gold standard treatment.
Much larger sample sizes are utilized, N = 300 to 3,000,
and multiple sites can be used to recruit patients.
Because they are quite an investment, they are usually
randomized, controlled studies.
Clinical Trials—Phases
Phase IV studies are also known as post-
marketing surveillance trials and involve the
ongoing or long-term assessment of safety in
drugs that have been approved for human use.
Detect any rare or long-term adverse effects in a much
broader patient population
The Size of a Clinical Trial
Lasagna’s Law
Once a clinical trial has started, the number of suitable
patients dwindles to a tenth of what was calculated before
the trial began.
The Size of a Clinical Trial
“How many patients do we need?”
Statistical methods can be used to determine the
required number of patients to meet the trial’s
principal scientific objectives.
Other considerations that must be accounted for
include availability of patients and resources and
the ethical need to prevent any patient from
receiving inferior treatment.
We want the minimum number of patients required to
achieve our principal scientific objective.
The Size of a Clinical Trial
Estimation trials involve the use of point and
interval estimates to describe an outcome of
interest.
Hypothesis testing is typically used to detect a
difference between competing treatments.
The Size of a Clinical Trial
Type I error rate (α): the risk of concluding a
significant difference exists between treatments
when the treatments are actually equally effective.
Type II error rate (β): the risk of concluding no
significant difference exists between treatments
when the treatments are actually different.
The Size of a Clinical Trial
Power (1 – β): the probability of correctly detecting
a difference between treatments—more commonly
referred to as the power of the test.
Truth
Conclusion
H1
H0
H1
H0
1–β
β
α
1–α
The Size of a Clinical Trial
Setting three determines the fourth:
For the chosen level of significance (α), a clinically
meaningful difference (δ) can be detected with a
minimally acceptable power (1 – β) with n subjects.
Depending on the nature of the outcome, the same
applies: For the chosen level of significance (α), an
outcome can be estimated within a specified margin of
error (ME) with n subjects.
Example: Detecting a Difference
The Anturane Reinfarction Trial Research Group
(1978) describe the design of a randomized
double-blind trial comparing anturan and placebo
in patients after a myocardial infarction.
What is the main purpose of the trial?
What is the principal measure of patient outcome?
How will the data be analyzed to detect a treatment
difference?
What type of results does one anticipate with standard
treatment?
How small a treatment difference is it important to detect
and with what degree of uncertainty?
Example: Detecting a Difference
Primary objective: To see if anturan is of value in
preventing mortality after a myocardial infarction.
Primary outcome: Treatment failure is indicated by
death within one year of first treatment (0/1).
Data analysis: Comparison of percentages of
patients dying within first year on anturan (π1)
versus placebo (π2) using a χ2 test at the α = 0.05
level of significance.
Example: Detecting a Difference
Expected results under placebo: One would
expect about 10% of patients to die within a year
(i.e., π2 = .1).
Difference to detect (δ): It is clinically interesting
to be able to determine if anturan can halve the
mortality—i.e., 5% of patients die within a year—
and we would like to be 90% sure that we detect
this difference as statistically significant.
Example: Detecting a Difference
We have:
H0: π1 = π2 versus H1: π1 π2 (two-sided test)
α = 0.05
1 – β = 0.90
δ = π2 – π1 = 0.05
The estimate of power for this test is a function of
sample size:
1 P z
z 2 SE
P z
p1q1 n1 p2 q2 n2
z 2 SE
p1q1 n1 p2 q2 n2
Example: Detecting a Difference
1β
β
1α
α/2
zα/2
Reject H0
Conclude difference
α/2
zα/2
Fail to reject H0
Conclude no
difference
Reject H0
Conclude difference
Example: Detecting a Difference
Assuming equal sample sizes, we can solve for n:
where
z 2 2 pq z p1q1 p2 q2
n
2
p1 p2
p
2
q 1 p
Example: Detecting a Difference
z 2 2 pq z p1q1 p2 q2
n
2
2
1.96 2 0.925 0.075 1.282 0.95 0.05 0.90 0.1
0.0025
1.96 0.373 1.282 0.371
0.0025
582.5
2
n = 583 patients per group is required
2
Power and Sample Size
n is roughly inversely proportional to δ2; for fixed α and
β, halving the difference in rates requiring detection
results in a fourfold increase in sample size.
n depends on the choice of β such that an increase in
power from 0.5 to 0.95 requires around 3 times the
number of patients.
Reducing α from 0.05 to 0.01 results in an increase in
sample size of around 40% when β is around 10%.
Using a one-sided test reduces the required sample
size.
Example: Detecting a Difference
Primary objective: To see if treatment A increases
outcome W.
Primary outcome: The primary outcome, W, is
continuous.
Data analysis: Comparison of mean response of
patients on treatment A (μ1) versus placebo (μ2)
using a two-sided t-test at the α = 0.05 level of
significance.
Example: Detecting a Difference
Expected results under placebo: One would
expect a mean response of 10 (i.e., μ2 = 10).
Difference to detect (δ): It is clinically interesting to
be able to determine if treatment A can increase
response by 10%—i.e., we would like to see a
mean response of 11 (10 + 1) in patients getting
treatment A and we would like to be 80% sure that
we detect this difference as statistically significant.
Example: Detecting a Difference
We have:
H0: μ1 = μ2 versus H1: μ1 μ2 (two-sided test)
α = 0.05
1 – β = 0.80
δ=1
For continuous outcomes we need to determine
what difference would be clinically meaningful, but
specified in the form of an effect size which takes
into account the variability of the data.
Example: Detecting a Difference
Effect size is the difference in the means divided
by the standard deviation, usually of the control or
comparison group, or the pooled standard
deviation of the two groups
d
where
1 2
12 22
n1 n2
Example: Detecting a Difference
1β
β
1α
α/2
zα/2
Reject H0
Conclude difference
α/2
zα/2
Fail to reject H0
Conclude no
difference
Reject H0
Conclude difference
Example: Detecting a Difference
Power Calculations an interesting interactive
web-based tool to show the relationship between
power and the sample size, variability, and
difference to detect.
A decrease in the variability of the data results in
an increase in power for a given sample size.
An increase in the effect size results in a decrease
in the required sample size to achieve a given
power.
Increasing α results in an increase in the required
sample size to achieve a given power.
Additional Slides
Common Inferential Designs
Comparing 2 independent percentages
χ2 test, Fisher’s Exact test, logistic regression
Comparing 2 independent means
2-sample t-test, multiple regression, analysis of
covariance
Comparing two independent distributions
Wilcoxon Rank-Sum test, Kolmogorov-Smirnov test
Comparing two independent time-to-event variables
Logrank test, Wilcoxon test, Cox proportional-hazards
regression
Estimation of Effect
For a dichotomous (yes/no) outcome
Estimate margin of error within a certain bound
Two or Multiple stage designs (Gehan, Simon, and
others)
Bayesian designs (Simon, Thall and others)
Exact binomial probabilities
Estimation of Effect
For a continuous outcome
Estimate margin of error within a certain bound
Is the magnitude of change above or below a
certain threshold with a given confidence
Detecting a Difference
Two-Arm studies: dichotomous or polytomous
outcome
2 × c Chi-square test (Fisher’s Exact test)
Mantel-Haenzsel
Logistic Regression
Generalized linear model
GEE or GLIMM if longitudinal
Detecting a Difference
Two-Arm studies: continuous outcome
Two-sample t-test (Wilcoxon rank sum)
Linear regression
General linear model
Mixed linear models for longitudinal data
Detecting a Difference
Time to event outcome
Log-rank test
Generalized Wilcoxon test
Likelihood ratio test
Cox proportional hazards regression
Detecting a Difference
Multiple-Arm studies: dichotomous or polytomous
outcome
r × c Chi-square test (Fisher’s Exact test)
Mantel-Haenzsel
Logistic Regression
Generalized linear model
GEE or GLIMM if longitudinal
Detecting a Difference
Multiple-Arm studies: continuous outcome
ANOVA (Kruskal-Wallis test)
Linear Regression – Analysis of Covariance
Multi-factorial designs
Mixed linear models for longitudinal data
Prognostic Factors
It is reasonable and sometimes essential to collect
information of personal characteristics and past
history at baseline when enrolling patient’s onto a
clinical trial.
These variables allow us to determine how
generalizable the results are.
Prognostic Factors
Prognostic factors know to be related to the
desired outcome of the clinical trial must be
collected and in some cases randomization should
be stratified upon these variables.
Many baseline characteristics may not be known to
be related to outcome, but may be associated with
outcome for a given trial.
Comparable Treatment Groups
All baseline prognostic and descriptive factors of
interest should be summarized between the
treatment groups to insure that they are
comparable between treatments. It is generally
recommended that these be descriptive
comparisons only, not inferential
Note: Just because a factor is balanced does
not mean it will not affect outcome and vice versa.
Subgroup Analysis
Does response differ for differing types of patients?
This is a natural question to ask.
To answer this question one should test to see if
the factor that determines type of patient interacts
with treatment.
Separate significance tests for different subgroups
do not provide direct evidence of whether a
prognostic factor affects the treatment difference:
a test for interaction is much more valid.
Tests for interactions may also be designed a
priori.
Adjusting for Covariates
Quantitative Response: Multiple Regression
Qualitative Response: Multiple Logistic
Regression
Time-to-event Response: Cox Proportional
Hazards Regression
Multiplicity of Data
Multiple Treatments – the number of possible
treatment comparisons increases rapidly with the
number of treatments. (Newman-Keuls, Tukey’s
HSD or other adjustment should be designed)
Multiple end-points – there may be multiple ways
to evaluate how a patient responds. (Bonferroni
adjustment, Multivariate test, combined score, or
reduce number of primary end-points)
Multiplicity of Data
Repeated Measurements – patient’s progress may
be recorded at several fixed time points after the
start of treatment. One should aim for a single
summary measure for each patient outcome so
that only one significance test is necessary.
Subgroup Analyses – patients may be grouped into
subgroups and each subgroup may be analyzed
separately.
Interim Analyses – repeated interim analyses may
be performed after accumulating data while the
trial is in progress.
Incidence and Prevalence
An incidence rate of a disease is a rate that is
measured over a period of time; e.g., 1/100
person-years.
For a given time period, incidence is defined as:
# of newly - diagnosed cases of disease
# of individuals at risk
Only those free of the disease at time t = 0 can be
included in numerator or denominator.
Incidence and Prevalence
A prevalence ratio is a rate that is taken at a
snapshot in time (cross-sectional).
At any given point, the prevalence is defined as
# with the illness
# of individuals in population
The prevalence of a disease includes both new
incident cases and survivors with the illness.
Incidence and Prevalence
Prevalence is equivalent to incidence multiplied by
the average duration of the disease.
Hence, prevalence is greater than incidence if the
disease is long-lasting.
Measurement Error
To this point, we have assumed that the outcome
of interest, x, can be measured perfectly.
However, mismeasurement of outcomes is
common in the medical field due to fallible tests
and imprecise measurement tools.
Diagnostic Testing
Sensitivity and Specificity
Sensitivity of a diagnostic test is the probability that
the test will be positive among people that have the
disease.
P(T+| D+) = TP/(TP + FN)
Sensitivity provides no information about people that
do not have the disease.
Specificity is the probability that the test will be
negative among people that are free of the disease.
Pr(T|D) = TN/(TN + FP)
Specificity provides no information about people that
have the disease.
Prevalence
SN == 56/70
SP
24/30
= =30/100
= 0.80
0.80 = 0.30
Healthy
Diseased
Non-Diseased
Diseased
Diseased
Non-Diseased
Positive Diagnosis
Negative Diagnosis
Diagnosed positive
A perfect diagnostic test has
SN = SP = 1
Healthy
Diseased
Non-Diseased
Diseased
Positive Diagnosis
Negative Diagnosis
A 100% inaccurate diagnostic
test has SN = SP = 0
Healthy
Diseased
Non-Diseased
Diseased
Positive Diagnosis
Negative Diagnosis
Sensitivity and Specificity
Example: 100 HIV+ patients are given a new
diagnostic test for rapid diagnosis of HIV, and 80 of
these patients are correctly identified as HIV+
What is the sensitivity of this new diagnostic test?
Example: 500 HIV patients are given a new
diagnostic test for rapid diagnosis of HIV, and 50 of
these patients are incorrectly specified as HIV+
What is the specificity of this new diagnostic test?
(Hint: How many of these 500 patients are correctly
specified as HIV?)
Positive and Negative Predictive
Value
Positive predictive value is the probability that a person
with a positive diagnosis actually has the disease.
Pr(D+|T+) = TP/(TP + FP)
This is often what physicians want-patient tests
positive for the disease; does this patient actually have
the disease?
Negative predictive value is the probability that a
person with a negative test does not have the disease.
Pr(D-|T-) = TN/(TN + FN)
This is often what physicians want-patient tests
negative for the disease; is this patient truly disease
free?
NPV
56/62 == 0.63
0.90
PPV == 24/38
Healthy
Diseased
Non-Diseased
Diseased
Diseased
Non-Diseased
Positive Diagnosis
Negative Diagnosis
Diagnosed positive
A perfect diagnostic test has
PPV = NPV = 1
Healthy
Diseased
Non-Diseased
Diseased
Positive Diagnosis
Negative Diagnosis
A 100% inaccurate diagnostic
test has PPV = NPV = 0
Healthy
Diseased
Non-Diseased
Diseased
Positive Diagnosis
Negative Diagnosis
PPV and NPV
Example: 50 patients given a new diagnostic test
for rapid diagnosis of HIV test positive, and 25 of
these patients are actually HIV+.
What is the PPV of this new diagnostic test?
Example: 200 patients given a new diagnostic test
for rapid diagnosis of HIV test negative, but 2 of
these patients are actually HIV+.
What is the NPV of this new diagnostic test? (Hint:
How many of these 200 patients testing negative for
HIV are truly HIV?)