Smallpox Vaccination - Office of Public Health Practice
advertisement

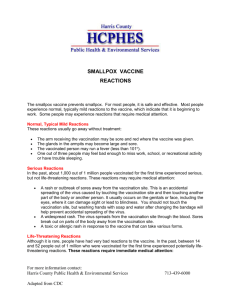
Smallpox Vaccination History of Vaccination in the US Before 1972, smallpox vaccination required for all children at age 1 year Most states required smallpox vaccination before school entry Vaccine DryVax©, a lyophilized, live vaccinia virus Store at -17oC to -20oC (-4 to - 1oF) Re-constituted store 30 days at 2–8oC (36 – 46oF) Contains polymyxin B sulfate dihydrostreptomycin sulfate chlortetracycline hydrochloride neomycin sulfate Aventis vaccine kept for emergencies Supply of Vaccine (12/5/2002) Existing Supply: Dryvax: 15 million doses (2.7 million doses Aventis Pasteur: 85 million doses are approved for distribution as a licensed vaccine) In Production: Acam 1000: 54 million doses Acam 2000: 155 million doses Strains of Vaccinia New York City Board of Health (NYCBOH) used in the DryVax and Aventis vaccine Lister strain used by many Europeans and the Israelis Both were used by the WHO Immune Response Neutralizing and HI antibodies appear about 10 days after vaccination >95% of primary vaccinees have antibody titres ≥ 1:10 Cell mediated response (DTH) can be detected as early as 2 days after vaccination Antibody response is about 4 – 8 days earlier than with natural variola infection, therefore vx after exposure can modify infection Source: Henderson & Moss. In Vaccines Eds Plotkin & Orenstein 3rd Ed 1999 Duration of Immunity Neutralizing antibodies (NA) can be detected > 20 years after Vx Anamnestic (memory) response seen upon re-vaccination, with significant elevation in NA by day 7 Source: Henderson & Moss. In Vaccines Eds Plotkin & Orenstein 3rd Ed 1999 Smallpox vaccination Administered using a bifurcated needle and 15 punctures delivered into the skin Positive “take” can be seen after about 7 days Bifurcated needle with and without the vaccine dose Vaccination site immediately after vaccination Note: small amount of blood which should appear at the site if punctures were sufficiently deep into the skin Vaccination Site Management Blot excess vaccine off the site Cover with non-occlusive bandage – this is to prevent maceration of the site If patient contact use gauze covered by a semi-occlusive bandage – to prevent transmission to others Site should be examined every day Normal Primary Vaccination Vaccinia virus proliferates in the basal cells of the epidermis By day 3….. Papule Day 5-6 Vesicle with surrounding erythema – so called Jennerian pustule Normal Primary Vaccination Day 8 – 9 Well formed pustule This is a major reaction – a POSITIVE TAKE Normal Primary Vaccination ◄ Normal reactions - 5 days Normal reaction 8 days Normal Primary Vaccination Day 12 + Pustules break down and crust over This is a major reaction – a POSITIVE TAKE Normal Primary Vaccination Day 14 Normal Primary Vaccination Day 16 Scabs begin to dry completely and then fall off by day 21 leaving a visible circular scar This is a major reaction – a POSITIVE TAKE Normal Vaccine Reactions Among Primary Vaccinees Low grade fever > 37.7oC 2 – 16% Swelling of regional lymph nodes 25 -50% Myalgia, chills, headache, fatigue 0.3-37% &/or nausea These are normal and should not be considered as adverse events They occur usually about 3-10 days after vaccination Vaccine reactions among re-vaccinees Among those for whom 25 years or more has elapsed since last vaccination, essentially all should experience a "major reaction" Vaccine reactions among re-vaccinees Level of response depends upon level of immunity Persons with some residual CMI can develop an erythema and even a pustule, BUT there may not be sufficient immunity to inhibit viral replication Those with substantial immunity may experience no more than a minor DTH reaction Reactions in re-vaccinees Day 3: Note small vesicles have already formed Accelerated reaction – major reaction. Note the position next to an old smallpox vaccination scar. Source: CDC web page http://www.bt.cdc.gov/training/smallpoxvaccine/reactions/normal_accelerated.html# Vaccine reactions among revaccinees It is impossible to distinguish clinically between an equivocal reaction which is due to residual immunity and one which is due to an allergic reaction Therefore all reactions, other than a major reaction, should be read as a no-take and repeated using a different batch of vaccine ReVaccination Primary Primary Types of reaction at the vaccination site Note: it is impossible to distinguish clinically between a re-vaccination reaction due to residual immunity and one due to a hypersensitivity reaction After Burdon KL. Textbook of Microbiology 1948 Equivocal Reaction Small area of erythema Possibly a small pustule Should be re-vaccinated After 2 unsuccessful re-vaccinations seek consultation Could result from residual immunity or reaction to vaccine components rather than a viral replication – but cannot distinguish between the two Equivocal reaction - Allergic Erythema and a small, evanescent papule are present within several days Symptoms resolve quickly These are “sensitivity” reactions that can be evoked with vaccine virus that is no longer viable. Revaccination is indicated. Equivocal reaction – No Reaction In some individuals, no take is seen after revaccination, even at long intervals after a primary vaccination. Usually this is due to poor technique, low potency vaccine, or inactivation of the virus at the skin site (e.g. if alcohol is used to prepare the site). Revaccination is indicated using vaccine of assured potency. Normal Variant Satellite Lesions The frequency of satellite lesions varies from study to study and ranges from 2.4 to 6.6 %. No treatment other than symptomatic relief Lymphangitis and cellulitis Normal Variant Cellulitis Serious Adverse Reactions Usually occur about 7 days after vaccination These are not the normal reactions to a smallpox vaccination Can be minimised by careful screening of vaccinees for contraindications Serious Adverse Events Potential adverse events should be referred to the designated Hospital Assigned Physician who can evaluate adverse events All adverse events should be reported to both the state health department and to the Vaccine Adverse Events Reporting System (VAERS) Do NOT report normal reactions to smallpox vaccination Smallpox Vaccination: Complications ▲ Eczema vaccinatum ► ◄ Generalized vaccinia Erythema multiforme ► ◄ Accidential transfer from mother to 2-year old Rates of Complications of Smallpox Vaccination Per Million Doses, USA, 1968†, †† Post-Vaccinal Encephalitis Progressive Vaccinia Eczema Vaccinatum Accidental Infection Death † Excludes contact cases All doses Primary doses 1.1 0.8 8.9 13.6 0.6 2.9 0.9 10.4 25.4 1.1 †† Source: From N. Engl J Med, 1969; 281: 1201-1208 Treatment for Serious Adverse Reactions VIG and cidofovir available only from CDC via state health departments Cidofovir (Vistide) may be used under an Investigational New Drug (IND) protocol to treat serious smallpox vaccine Vaccinia Immune Globulin Contains thimerosal Dosage: Usual dosage 0.6ml/kg IM dose may be divided For severe cases 1 – 10 ml/kg 700 doses of IM VIG are available now Approximately 3300 doses of the new IV VIG will be available by the end of December 2002. Indications for Use of Vaccinia Immunoglobulin (VIG) for Treatment of Adverse Reactions Associated With Smallpox Vaccination Inadvertent inoculation of other body sites — Usually not required — Indicated for inoculation of eye or eyelid — BUT contraindicated for vaccinial keratitis because increased scarring can occur Generalized vaccinia—Indicated if patient is toxic or if patient has serious underlying illness Source: Vaccinia (smallpox) vaccine: recommendations of the Advisory Committee on Immunization Practices (ACIP), 2001. MMWR 2001;50(RR10):1-25 Indications for Use of Vaccinia Immunoglobulin (VIG) for Treatment of Adverse Reactions Associated With Smallpox Vaccination - II Eczema vaccinatum—Indicated for severe cases Progressive vaccinia—Indicated for severe cases Postvaccinial encephalitis — Not effective Contraindications to Vaccine in the Absence of Exposure or Potential Exposure to Smallpox Contraindications: Pre-Event Eczema and atopic dermatitis and other chronic skin conditions: 28 million in the US at risk for eczema vaccinatum [Has the patient had an itchy, scaly rash that lasts more than 2 weeks and which comes and goes? – this should be considered as atopic dermatitis] Eye disease of the cornea or conjunctiva, especially if pruritic or inflammatory Contraindications: Pre-Event Immunosuppression (organ transplants, HIV and cancer): 10 million individuals (3.6 percent) may be at increased risk for progressive vaccinia ≥2mgm/kg/ day prednisone or ≥20mgm/day for 14 or more days Pregnancy Any of the previous conditions in a member of the household Contraindications: Pre-Event Breast feeding because of risk of inadvertent inoculation Hypersensitivity to any of the vaccine components Hypersensitivity to thimerosal Contraindications: Post Event None if a person is exposed or at potential exposure Risk of Transmission to Contacts Transmission in virtually all cases from persons who were primary vaccinees 16.8 – 20 cases of contact EV per 106 primary vaccinations 62% of contacts cases in children < 5 years 1.8% of contact cases in persons > 20 years Source: Neff et al. Contact Vaccinia – Transmission of Vaccinia From Smallpox Vaccination. JAMA 288;(15) 1901-1905. Oct 16, 2002 Recent Israeli Experience Lister strain, considered to have fewer side effects Total full reaction among vaccinated – 76 % ( n= 929 ) Side Effects: Fever - 5 % Muscle pain - 18 % Fatigue and weakness - 31 % Other - 13 % . Headaches - 28 % Nausea - 12 % Shivering - 9 % There was one case of suspected encephalitis. The physicians in that case wanted to do a spinal tap, though the patient refused (Israeli Ministry of Health records, 2002) Efficacy of Post-Exposure Vaccination " Vaccination within 3 days of exposure will completely prevent or significantly modify smallpox in the vast majority of persons Overall, when estimates for prevention and disease modification are combined, fewer than 5% of all persons vaccinated within 3 days after exposure would be at risk for disease of normal severity. Vaccination 4 to 7 days post-exposure still offered protection to many people, but significantly less than vaccination before 4 days." Source: Ray Strikas, MD, CDC. Dec 13, 2002 Q & A: Vaccine and Pregnancy Q. What if a woman is vaccinated and then finds out that she is pregnant? A. Vaccination during pregnancy does not appear to increase the risk of miscarriage or stillbirth. Fetal vaccinia is rare. (Plotkin & Orenstein p. 85). VIG may be indicated, contact the HAP. Q & A: VIG and Immunity Q. If VIG is administered for a severe reaction, will this affect my immunity? A. No, the fact that there is a severe reaction indicates that there has been a strong immune response. The VIG will have no impact on the immune system and its memory Q & A: Steroids Q. A person who is on steroids should not receive the vaccine in a pre-event situation because of immunosuppression. What is the dose of steroid that should be the cutoff for deciding immunosuppression or not? A. 20mg/day prednisone for 14 days 2mg/kg/day prednisone These are similar to the levels of steroid that are used for the cutoff for other live virus vaccines such as MMR or varicella Q & A: Re-Vaccination Q. What is the recommended timeframe for revaccination on non-takers? A. If their vaccination site is looked at on Day 7 -12 & found to be a non-take, reimmunize immediately or any time thereafter. (Note the patient receives a new PVN number) Q & A: Swimming Pools Q. Can I swim in the pool before the vaccination scab has dropped off? A. No, even with a dressing, this is probably an inappropriate activity References Henderson & Moss.Vaccines 3rd Ed. Eds Plotkin & Orenstein 3rd Ed 1999 CDC. Vaccinia (Smallpox) Vaccine Recommendations of the Advisory Committee on Immunization Practices. MMWR 50 No. RR-10. June 22, 2001 Neff et al. Contact Vaccinia – Transmission of Vaccinia From Smallpox Vaccination. JAMA 288;(15) 1901-1905. Oct 16, 2002 www.bt.cdc.gov/agent/smallpox/index.asp Supplemental slides Generalized Vesicular or Pustular Rash Illness Protocol Patient with Acute, Generalized Vesicular or Pustular Rash Illness Institute Airborne & Contact Precautions Alert Infection Control on Admission Low Risk for Smallpox (see criteria below) History and Exam Highly Suggestive of Varicella Diagnosis Uncertain Varicella Testing Optional Test for VZV and Other Conditions as Indicated Moderate Risk of Smallpox (see criteria below) ID and/or Derm Consultation VZV +/- Other Lab Testing as indicated Non-Smallpox Diagnosis Cofirmed Report Results to Infx Control High Risk for Smallpox (see criteria below) ID and/or Derm Consultation Alert Infx Control & Local and State Health Depts No Diagnosis Made Ensure Adequacy of Specimen ID or Derm Consultant Re-evaluates Patient Response Team Advises on Management & Specimen Collection Cannot R/O Smallpox Contact Local/State Health Dept Testing at CDC NOT Smallpox Further Testing SMALLPOX CRITERIA FOR DETERMINING RISK OF SMALLPOX High Risk for Smallpox report immediately 1.Febrile prodrome (see below) AND 2.Classic smallpox lesions (see below and photo at right) AND 3.Lesions in same stage of development (see below) Moderate Risk for Smallpox urgent evaluation 1.Febrile prodrome (see below) AND 2.One MAJOR smallpox criterion (see below) OR 1.Febrile prodrome (see below) AND 2. >4 MINOR smallpox criteria (see below) Low Risk for Smallpox manage as clinically indicated 1.No viral prodrome OR 2.Febrile prodrome and <4 MINOR smallpox criteria (no major criteria) (see below) MAJOR SMALLPOX CRITERIA FEBRILE PRODROME: occurring 1-4 days before rash onset: fever >102°F and at least one of the following: prostration, headache, backache, chills, vomiting or severe abdominal pain. All smallpox patients have a febrile prodrome. The fever may drop with rash onset. CLASSIC SMALLPOX LESIONS: deep, firm/hard, round, well-circumscribed; may be umbilicated or confluent LESIONS IN SAME STAGE OF DEVELOPMENT: on any one part of the body (e.g., the face, or arm) all the lesions are in the same stage of development (i.e. all are vesicles, or all are pustules) MINOR SMALLPOXCRITERIA Centrifugal distribution: greatest concentration of lesions on face and distal extremities First lesions on the oral mucosa/palate, face, forearms Patient appears toxic or moribund Slow evolution: lesions evolve from macules to papulespustules over days Lesions on the palms and soles (majority of cases) Condition Clinical Clues Varicella (primary infection with varicella-zoster virus) Most common in children <10 years; children usually do not have a viral prodrome Disseminated herpes zoster Prior history of chickenpox; immunocompromised hosts Impetigo (Streptococcus pyogenes, Staphylococcus aureus) Honey-colored crusted plaques with bullae are classic but may begin as vesicles; regional not disseminated Drug eruptions and contact dermatitis Exposure to medications; contact with possible allergens Erythema multiforme (incl. Stevens Johnson Sd) Major form involves mucous membranes and conjunctivae Enteroviruses incl. Hand, Foot and Mouth disease Summer and fall; fever and mild pharyngitis at same time as rash; distribution of small vesicles on hands, feet and mouth or disseminated Disseminated herpes simplex Lesions indistinguishable from varicella; immunocompromised host Scabies; insect bites (incl. fleas) Pruritis; in scabies, look for burrows (vesicles and nodules also occur); flea bites are pruritic, patient usually unaware of flea exposure Molluscum contagiosum Healthy afebrile children; HIV+ individuals Bullous Pemphigoid Bullous lesions. Positive Nikolski sign. Secondary syphilis Rash can mimic many diseases; rash may involve palms and soles; 95% maculo-papular, may be pustular. Sexually active persons Conditions With Vesicular or Pustular Rashes Laboratory Testing for Varicella: Collect at least 3 good specimens from each patient Direct fluorescent antibody (DFA)—rapid, depends on adequate specimen (see below) Indirect fluorescent antibody (IFA) —rapid, depends on adequate specimen (see below) Polymerase chain reaction (PCR)--available in research labs, some tertiary care centers Serologic testing: an IgG (collected at time of rash) provides evidence of prior varicella, and makes acute varicella infection unlikely but does not rule out herpes zoster in persons at risk of dissemination. IgM is not useful for diagnosis. VZV culture—results delayed, useful only if processed in-house EM (electron microscopy)—can identify herpes viruses How to Collect a Specimen for DFA or IFA Testing 1. 2. 3. 4. 5. 6. Unroof (open) vesicle or pustule with a sterile lancet Swab base of vesicle vigorously with a sterile swab Smear swab onto 3 areas (or wells) of a microscope slide Allow slide to air dry Transport to lab for immediate fixing and staining VZV positive specimens are seen with varicella (chickenpox) and herpes zoster (shingles) The hospital lab performs _________________ test For DFA/IFA , call ________________ (specimen is tested at outside lab) A suspected case of smallpox is a public health and medical emergency. Clinical case definition of smallpox: an illness with acute onset of fever >101°F followed by a rash characterized by vesicles or firm pustules in the same stage of evolution without other apparent cause. Report ALL suspected cases (without waiting for lab results) to: 1. Hospital Infection Control ( ) ___-____ or ( ) ___-____ Pager 2. (Local) health department ( ) ___-____ or ( ) ___-____ Pager 3. (State) health department (517) 335-9030 or (517)335-8024 Questions ? Centers for Disease Control and Prevention: (404)639-3532 days; Nights/weekends/holidays: (770) 488-7100