pain - Texas Tech University Health Sciences Center
advertisement

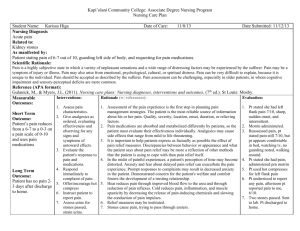
This PowerPoint file is a supplement to the video presentation. Some of the educational content of this program is not available solely through the PowerPoint file. Participants should use all materials to enhance the value of this continuing education program. Nursing 311112 Pain Management: Acute Pain Brenda Threadgill, RN, BSN, MS, CHPN, Retention Counselor, Traditional Undergraduate Program TTUHSC, Lubbock, TX Nursing 311112 Objectives 1. Recognize basic principles and barriers. Nursing 311112 Objectives 2. Indicate outcomes, history, and processes. Nursing 311112 Objectives 3. Identify expectations and assessment principles. Talking Points • Define basic principles of pain management • Describe barriers to good pain management • Differentiate outcomes of good vs poor pain management • Discuss the history of pain and pain treatments Talking Points • Discuss a brief overview of pain processes • Identify expected findings in acute vs chronic pain • Describe the principles of a thorough pain assessment Perceptions of Pain • John is lying in bed, watching TV • He appears to be uncomfortable, grimacing occasionally, changing position with difficulty, and gritting his teeth • Blood pressure (BP): 145/92 • Respirations: 28/minute • Pulse: 92 Perceptions of Pain • He had 2 acetaminophen and hydrocodone 5/500 (Lortab) 2 hours ago and his pain went down from 7/10 to 3/10 • When you ask how his pain is doing, he tells you his pain level is now 8/10 • What will you do? Perceptions of Pain • Jane is sitting up at the side of her bed, playing cards with her sister • They are laughing and she appears comfortable • BP: 115/76 • Respirations: 18/min • Pulse: 84 Perceptions of Pain • She had morphine 5 mg intravenous push (IVP) 2 hours ago and her pain went from 7/10 to 3/10 • When you ask how she’s feeling, she states that her pain is back up to an 8/10 • What are you going to do? Perceptions of Pain • Bill has been admitted to your floor • He has lung cancer with metastasis to the bone • He came into the emergency room (ER) with complaints of uncontrolled pain for the past 3 days Perceptions of Pain • His ordered pain medication is acetaminophen and hydrocodone 5/500 (Lortab) – 1 to 2 tabs every 6 hours pro re nata (PRN), of which he has been taking 2 tabs 6 times a day Perceptions of Pain • He rated his pain in the ER as 10/10 and was given morphine 5 mg IVP 6 hours ago, with minimal relief of pain • He was then given 10 mg morphine IVP 5 hours ago, with partial relief of pain (6/10) Perceptions of Pain • He was given another 10 mg morphine IVP 4 hours ago, with complete relief of pain (0/10) • He is now asleep Perceptions of Pain • When you go into his room to assess him, he does not wake until you call his name and shake him • He talks to you appropriately and takes a drink of water • He states that his pain is coming back a little and rates it as 2/10 at this time Perceptions of Pain • • • • BP:105/76 Respirations: 12/minute Pulse: 74 As soon as you turn to write down his vital signs, he has fallen asleep again • What is your next step? How do you feel about these patients? Pain management is a holistic combination of science and art Science Research and Technology Person Mind, Body, and Spirit Holistic Universal Human Experience Art Unique Experience, Potential for Meaning Environment Family, Friends, Way of Being “When we honestly ask ourselves which persons in our lives mean the most to us, we often find that it is those who, instead of giving advice, solutions or cures, have chosen rather to share our pain and touch our wounds with a warm and tender hand.” -Henri Nouwen Basic Principles 1. 2. Prevent pain whenever possible Control pain to the level that is acceptable to the patient Who has pain? • Every living creature is capable of experiencing some degree of pain • Every person alive has experienced pain of some sort • Every nurse has cared for a person experiencing pain of some sort Why should we care? • Pain is a universal human phenomenon • There are as many ways to experience pain as there are people in the world • Every person’s pain is unique to that person • Nurses are the one constant in most people’s journey to optimal pain relief Why should we care? • The good: – optimal pain relief leads to better quality of life and better patient outcomes • The bad: – poor pain relief leads to negative disturbances in health • The ugly: – poor pain relief leads to increased financial drains on the healthcare system Stand and Defend • Nurses are the front line defenders against pain: – suggest and carry out medication orders – stand guard against pain increasing or returning – suggest and carry out non-pharmacological interventions – perception of caring Frontline Advocate • Nurses are the frontline advocates for optimal pain relief, especially if there are inadequate orders for pain relief • Nurses must advocate for their patients with: – scientific, evidence-based knowledge about pain and pharmacology – caring determination to get the appropriate orders to obtain optimal pain relief for our patients Can we do a better job? • Multiple studies have shown that the most important barriers to optimal pain relief are: – beliefs and attitudes of healthcare practitioners – lack of organizational support • training • prioritization of pain assessment • support for evidence-based practices Can we do a better job? – general expectations that good pain relief is often not possible or is not a priority concern of • healthcare practitioners • doctors • nurses Does it have to be this way? • The quickest and easiest part of the system that can be changed is you – taking part in learning more about pain relief – changing your own beliefs and attitudes – having the determined will to be a strong patient advocate for excellence in pain relief • Numerous studies have consistently identified nurses as the key players in making a difference in the best practices for pain relief History of Pain • We assume that pain has been around for as long as there have been people • We know that people in pain seek relief from pain • Earliest records of prescriptions go back to the Babylonians around 3000 B.C. History of Pain • The Chinese (2700 B.C.) had a compendium of herbal remedies (40 volumes) called the Pen Tsao • The early Egyptians (1500 B.C.) had their own documented remedies called Ebers Papyrus Wonder Drugs • Decoctions from the bark of the willow tree are some of the first recorded treatments for pain and became the basis from which we derived aspirin • Aspirin is the original wonder drug and remains one of the most widely used medications for pain in the entire world Wonder Drugs • Other early remedies for pain included fermentation and distillations of various fruits and grains, such as: – grapes – barley – corn – wheat Morphine • Opium has been used for centuries for relaxation, euphoria, and relief of pain • The first recorded isolation of morphine from opium occurred around 1805 by the German chemist Friedrich Serturner – he tested his discovery on himself and three young friends by dosing each of them with 100mg of unrefined morphine – they spent the next three days suffering from acute morphine intoxication Morphine – despite this inauspicious beginning, morphine proved to be the wonder drug of the century and remains the gold standard to which all other pain medications are compared What is pain? • International Association for the Study of Pain defines pain as: – “an unpleasant sensory and emotional experience arising from actual or potential tissue damage” • Margo McCaffery defines pain as: – “whatever the experiencing person says it is, occurring whenever he/she says it does.” • Cox defines pain as: – “a complex, physiological, and psychological phenomenon that is subjective in nature.” Pain Concepts • The word “pain” comes from the Latin word poena, meaning penalty or punishment – this concept still has relevance even today • Pain is multidimensional – it has many aspects: • • • • physical mental emotional spiritual – it is rarely comprised of only one aspect and often all aspects are involved Pain Concepts • Most important - it is subjective in nature – we can look for clues to support the claim of pain • they may or may not be there – never look for clues to discount a report of pain Why does pain hurt? • Easy answer: we don’t know • Complicated answer: we don’t know everything – so many pathways – so many complicating factors – every person is unique Kinds of Pain • There are multiple ways of classifying pain, including: – underlying pathophysiology • nociceptive vs neuropathic pain – length of time • acute pain vs chronic pain – mixed pain classification systems • chronic noncancer pain • chronic pain syndrome Kinds of Pain • Does it matter how pain is categorized? – only in that it helps guide treatment options – mixed pain classification systems • chronic noncancer pain • chronic pain syndrome Acute Pain • • • • Acute pain is a warning There is a physical reason for it It is time-limited We expect acute pain to decrease as healing takes place and eventually go away completely Injury healed Injury Healing continues High pain rating Healing taking place Chronic Pain • Pain lasts longer than expected (even after the injury is healed) • Not time-limited (lasts longer than 3-6 months) • There is a large psychosocial component to most chronic pain states • Chronic pain is usually much harder to manage successfully Injury Chronic: Meds may not be effective Persistent pain after original injury has healed Chronic pain Acute: Meds effective Little to no pain after injury has healed How do we do it? • The nursing process gives us a map to follow to provide the best practices in excellent pain relief: – assessment – nursing diagnosis – planning – implementation – evaluation Assessment 1. 2. Believe the patient’s self-report of pain Do something about it Pitfalls of Assessment • Assessment is where we tend to “slip up” and trust our own judgment, instead of believing the patient’s self-report of pain Tools • Easiest to use: scales – numeric scale • 0 = no pain to 10 = worst pain – verbal descriptor scale • mild pain • moderate pain • severe pain – Wong-Baker faces scale • happy face to crying face – colors scale • white for no pain to red for worst pain Filling out the Picture • Location of the pain • Pattern of the pain – When does it happen? – What causes it to start or get worse? – What causes it to stop or get better? – How long does it last? – How does it affect your activities/your quality of life? – How have you coped with pain in the past? Filling out the Picture • One thing that is often overlooked is asking the patient about his/her beliefs about pain, as well as his/her expectations and goals for pain relief Helping with the Words • Quality of the pain – nociceptive pain descriptors • • • • • • dull sharp aching pressure gnawing cramping Helping with the Words – neuropathic pain descriptors • burning • tingling • numbing Helping with the Words • Intensity of the pain: – mild pain • • • • annoying nagging uncomfortable troublesome – moderate pain • • • • distressing miserable grueling horrible Helping with the Words – severe pain • • • • • intense excruciating dreadful unbearable agonizing Helping with the Words • It is perfectly acceptable to combine a scale and a list of descriptors and intensity words, as long as you do not guide the patient to a rating or words Intangible Aspects of Pain • Emotional and spiritual pain need additional assessment • Ask questions (gently, but thoroughly) • Be present to hear the answers • Listen to what is not said – pursue the obvious, but listen for what is not being said • Emotional and spiritual pain relate to the physical • People fear pain (the great spoken dread) – people fear abandonment even more (the great unspoken dread) Special Circumstances • Psychosocial issues can confuse and complicate pain management – our own psychosocial issues come into play when we work with patients – chronic pain generally has more psychosocial context than acute pain – some patients may feel that they need to suffer or be punished (for a variety of reasons) – some caregivers may feel that the patient needs to suffer or be punished Suffering • All suffering involves pain but not all pain is suffering • Suffering is multidimensional pain, taken to a deeper level, usually involving more than just physical pain • Grief and existential despair can be catalysts for suffering Suffering • May grieve the loss of: – relationship – health – life • May ask existential questions: – Why? Why is this happening? – Is this all there is? – Am I alone? – Am I being punished? Suffering • The best way to help those who are suffering is to be present with them in their pain • Help them to find meaning in their pain – ask them to tell you about their pain and what it means to them • Give them the opportunity to talk • Refer to counseling or to a spiritual practitioner of their choice, if agrees Medications • Patients may have very real fears about using medications, particularly opioids – fear of addiction – fear of worsening disease process – fear that medications won’t be strong enough later on if used now – fear of hastening death – fear of losing control – fear of being sedated and abandoned • Intractable pain is our “skeleton in the closet”, but it is real Nursing 311112 Pain Management: Pain Acute If you have any questions about the program you have just watched, you may call us at: (800) 424-4888 or fax (806) 743-2233. Direct your inquiries to Customer Service. Be sure to include the program number, title and speaker. Nursing 311112 Release Date: 5/01/2012 The accreditation for this program can be found by signing in to www.ttuhsc.edu/health.edu Nursing 311112 The Texas Tech University Health Sciences Center Continuing Nursing Education Program is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center's Commission on Accreditation. Provider approved by California Board of Registered Nursing, Provider #CEP11800, for the designated number of contact hours for each program. Provider approved by Florida Department of Health Board of Nursing, Provider #FBN2060. Provider approved by West Virginia Board of Examiners for Registered Professional Nurses, Provider #WV1998-0262RN. Iowa Board of Nursing approved provider #325. Accepted by the North Carolina Board of Nursing. Reminder to all PARTICIPANTS, certificates should be retained for a period of four (4) years. Health.edu reports Florida Continuing Education (Contact Hours) to CE Broker. This activity provides 1.5 contact hours. Nursing 311112 This activity is presented for educational purposes only. Participants are expected to utilize their own expertise and judgment while engaged in the practice of nursing. The content of the presentations is provided solely by presenters who have been selected for presentations because of recognized expertise in their field. Nursing 311112 DISCLOSURE TO PARTICIPANTS Requirements of successful course completion: •Complete the program via video presentation, PowerPoint slides, audio presentation, and/or manuscript. •Complete the course evaluation. •Complete the posttest with a score of 80% or greater. •Complete the time utilized in course completion including the posttest. Nursing 311112 Conflicts of Interest: Brenda Threadgill, RN, BSN, MS, CHPN has disclosed that no financial interests, arrangements or affiliations with organization/s that could be perceived as a real or apparent conflict of interest in employment, leadership positions, research funding, paid consultants or member of an advisory board or review panel, speaker’s bureau, major stock or investment holder, or other remuneration. Commercial Support: There is no commercial support and/or relevant financial relationships related to this educational activity. Commercial support is defined as financial (or in-kind) contributions given by a commercial interest, which is used to pay all or part of the costs of a CNE activity. Relevant financial relationships are defined as financial relationships of any amount, occurring within the past 12 months, including financial relationships of a spouse or life partner that could create a conflict of interest. Nursing 311112 Non-endorsement of Products: Brenda Threadgill, RN, BSN, MS, CHPN has disclosed that no significant relationships with commercial companies whose products or services are discussed in educational presentations. For speakers, significant relationships include receiving from a commercial company research grants, consultancies, honoraria and travel, or other benefits or having a self-managed equity interest in a company. Disclosure of a relationship is not intended to suggest or condone bias in any presentation, but is made to provide participants with information that might be of potential importance to their evaluation of a presentation. Off-label Use: Brenda Threadgill, RN, BSN, MS, CHPN has disclosed that no products with off-label or unapproved uses are discussed within this activity. Nursing 311112 Individual programs are provided for a two (2) year period. Participants should check with their site coordinator, sign in to Health.edu’s internet site, http://www.ttuhsc.edu/health.edu or call Education Services at 1-800-424-4888 for information on the date through which this learning activity is provided. For questions or comments regarding accreditation, please call Education Services at 1-800-424-4888.To speak to a Customer Service representative, please call 1-800-424-4888. Institutional refund is available to subscribing organizations according to Health.edu’s tuition refund policy. See your site coordinator to view this program.