ImmunoPathology I
advertisement

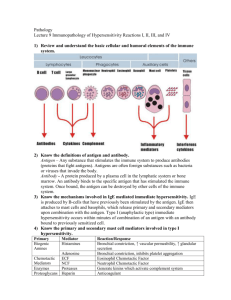
ImmunoPathology I R. Pat Bucy, MD, PhD Professor of Pathology, Microbiology, and Medicine Type I Hypersensitivity (AKA: Anaphylactic type, immediate hypersensitivity) • Due to activity of IgE • Cross-linkage of Fce resulting in mast cell degranulation • Anaphylaxis - local vs systemic • Skin test peaks in ~10 minutes • Normal function of IgE Immediate Hypersensitivity (Type I) Type II Hypersensitivity (AKA: Antibody mediated cytotoxic type) • Ab coating of cells → phagocytosis & ADCC • Ab + complement → direct lysis • Ab interaction with cell surface receptor → activation or inhibition of bioactivity Examples of Antibody-Mediated Diseases (Type II Hypersensitivity) Disease Autoimmune hemolytic anemia Autoimmune thrombocytopenic purpura Pemphigus vulgaris Target Antigen Erythrocyte membrane proteins (Rh blood group antigens, I antigen) Platelet membrane proteins (gpllb:Illa integrin) Clinicopathologic Mechanisms of Disease Manifestations Opsonization and phagocytosis Hemolysis, anemia of erythrocytes Opsonization and phagocytosis Bleeding of platelets Proteins in intercellular junctions of epidermal cells (epidermal cadherin) Vasculitis caused by Neutrophil granule proteins, ANCA presumably released from activated neutrophils Goodpasture syndrome Noncollagenous protein in basement membranes of kidney glomeruli and lung alveoli Acute rheumatic fever Streptococcal cell wall antigen; antibody cross-reacts with myocardial antigen Antibody-mediated activation of Skin vesicles (bullae) proteases, disruption of intercellular adhesions Neutrophil degranulation and Vasculitis inflammation Myasthenia gravis Acetylcholine receptor Graves disease (hyperthyroidism) Insulin-resistant diabetes Pernicious anemia TSH receptor Insulin receptor Intrinsic factor of gastric parietal cells Complement- and Fc receptormediated inflammation Nephritis, lung hemorrhage Inflammation, macrophage activation Myocarditis, arthritis Antibody inhibits acetylcholine binding, down-modulates receptors Antibody-mediated stimulation of TSH receptors Antibody inhibits binding of insulin Neutralization of intrinsic factor, decreased absorption of vitamin B12 Muscle weakness, paralysis Hyperthyroidism Hyperglycemia, ketoacidosis Abnormal erythropoiesis, anemia Type III Hypersensitivity (Immune complex type) • Immune complex physical chemistry and IC deposition • IC deposition in vessel walls and glomeruli – complement deposition and neutrophil activation • Skin test peaks in ~10 hours – Skin test called Arthus reaction Examples of Immune Complex-Mediated Diseases (Type III Hypersensitivity) Clinicopathologic Manifestations Nephritis, skin lesions, arthritis, others Disease Systemic lupus erythematosus Antigen Involved Nuclear antigens Poststreptococcal glomerulonephritis Streptococcal cell wall antigen(s); may be "planted" in glomerular basement membrane Nephritis Polyarteritis nodosa Reactive arthritis Serum sickness Hepatitis B virus antigen Bacterial antigens (Yersinia ) Various proteins, such as foreign serum protein (horse anti-thymocyte globulin) Systemic vasculitis Acute arthritis Arthritis, vasculitis, nephritis Arthus reaction (experimental) Various foreign proteins Cutaneous vasculitis Type IV Hypersensitivity (Cell mediated type) • Delayed Type Hypersensitivity (DTH) - CD4+ T cell mediated macrophage and endothelial activation • Granulomatous inflammation - continual T cell drive with lack of complete M digestion of Ag • Cytolytic T Lymphocytes (CTL) - direct lysis of target cells involving TCR recognition at effector phase • NK cell activity - no specific recognition (no TCR). Require IL-2 and perhaps other cytokines. • Technical difficulties in experimental determination of cellular vs Ab mediated immune mechanisms. Granulomatous Inflammation • Aggregation of macrophages with fibrosis • Associated with chronic T cell and macrophage activation • Antigen that is resistant to macrophage degradation Examples of T-Cell-Mediated (Type IV) Hypersensitivity Disease Type 1 diabetes mellitus Specificity of Pathogenic T cells Antigens of pancreatic islet βcells ( o i n t s h u e l r i s n , g l u t a m i c a c i d d e c a r b o x y l a s e , ) Clinicopathologic Manifestations Insulitis (chronic inflammation in islets), destruction of βcells; d i a b e t e s Multiple sclerosis Protein antigens in CNS myelin (myelin Demyelination in CNS with basic protein, proteolipid protein) perivascular inflammation; paralysis, ocular lesions Rheumatoid arthritis Unknown antigen in joint synovium (type II collagen?); role of antibodies? Chronic arthritis with inflammation, destruction of articular cartilage and bone Peripheral neuropathy; Guillain-Barré syndrome? Inflammatory bowel disease (Crohn's disease) Protein antigens of peripheral nerve myelin Neuritis, paralysis Contact dermatitis Environmental chemicals, e.g., poison ivy (pentadecylcatechol) Unknown antigen; may be derived from Chronic inflammation of ileum intestinal microbes and colon, often with granulomas; fibrosis, stricture Dermatitis, with itching; usually short-lived, may be chronic with persistent exposure Relationship of antibody vs cell mediated hypersensitivity • Radical difference in assay/detection methodology • Usually both are present in a strong immune response • Presence of antibody can be a marker of a specific T cell mediated lesion • Passive transfer is the key experimental approach to determine primary cause of response. Classification Scheme Mechanism vs Antigen • Classical system focuses on mechanism – Don’t know all mechanisms (especially early) – Actual disease mechanisms overlap • Alternative system focused on antigen drive – The kinetic course of antigen concentration is the key immunoregulatory entity. – Often don’t know the specific driving antigens – Infection, environmental, tumors, iatrogenic, self. Leprosy • Two forms of disease; one bug (Mycobacterium leprae). • Tuberculoid leprosy - intense immune response with low organism load • Lepromatous leprosy - suppressed immune response with high organisms load • Different cytokine patterns in T cell response correlate with forms of disease Contact Dermatitis • Exposure of the skin to multiple agents can cause sensitization. On repeated exposure, an eczematous eruption occurs. • Histologically, the lesion is a mononuclear infiltrate, epidermal spongiosis (intercellular edema), and vesicle formation (bullae). • Depends on ability covalently conjugate to proteins. • Exposure to poison ivy is a common example of this process. Penicillin Allergy • Since penicillin is fairly reactive with proteins, sensitization is common. • Depending on the idiosyncratic nature of the immune response and subsequent exposure, several clinical syndromes may develop. • Formation of IgE can result in systemic anaphylaxis after penicillin therapy (particularly after intravenous administration). • Formation of IgG and drug conjugates of serum proteins (albumin) can lead to a "serum sickness" syndrome, involving fever, skin rash, lymphadenopathy, and edema. Occasionally arthritis, nephritis, and vasculitis may result. • Conjugation to red blood cells with high dose IV therapy and IgG formation can result in development of hemolytic anemia. Tumor Antigens for CD8+ T cells Organ/Tissue Transplants Alloantigen Recognition Direct Presentation Indirect Presentation Recipient APC Donor APC Many endogenous peptides T Donor peptide T Recipient T cells Mechanisms of transplant rejection (classical) • No “real” physiologic mechanism (evolutionarily selected) • Hyperacute rejection • Acute vascular rejection • Acute cellular rejection • Chronic rejection Mechanisms of transplant rejection • Cytotoxic damage to endothelial cells with coagulation • “DTH” in interstitium - CD4+ T cells & M activation • CTL activity on parenchymal cells (tubules, cardiomyocytes, bile ducts, hepatocytes) • T cell mediated arteritis with intimal proliferation and infarction • ADCC and NK cell activity in interstitium • Antibody mediated injury to endothelia with intimal proliferation and infarction Clinical Monitoring of Allograft Rejection • • • • • Kidney - serum creatinine/Biopsy Heart - Blind Biopsy Liver - Bilirubin, transaminases/Biopsy Lung - Pulmonary Function tests/Biopsy Pancreas - No good method, (urinary amylase, or cytology) IgE Ab Immune Complex T cells