PowerPoint 演示文稿
advertisement

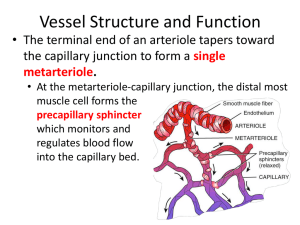
LIU Chuan Yong 刘传勇 Institute of Physiology Medical School of SDU Tel 88381175 (lab) 88382098 (office) Email: liucy@sdu.edu.cn Website: www.physiology.sdu.edu.cn Section 3 Physiology of the Blood Vessels I. Physiological Classification of Blood Vessels Windkessel Vessel --- Aorta and big arteries. Contain a large amount of elastic tissue besides the smooth muscle. Transiently store blood during systole, and then shrink to produce onward blood flow during diastole. Convert the sharp pressure fluctuations in the left ventricle (0 to 120 mmHg) into much smaller pressure fluctuations in the arteries (80 to 120 mmHg). Convert the intermittent ventricular ejection into continuous blood blood in the vessels This function of large arteries is known as Windkessel effect. 2. Distribution Vessel – Middle arteries Rich in smooth, systole or diastole under some physical and chemical factors. Together with resistance vessels, they match the blood flow to different organs with their requirements. Distribution of Cardiac Output 3. Precapillary Resistance Vessels – Small arteries and arterioles Less elastic than the larger arteries Hhave a thicker layer of smooth muscle. Provide the greatest resistance to blood flow through the arterial system since they have narrow lumina. 4. Precapillary Sphincter muscle Partially determines the amount of blood flowing through a particular capillary bed Allow only 5% 10% of the capillary in bed skeletal muscles, for example, to be open at rest. 5. Exchange Vessel – Capillary the walls are composed of only one cell layer – a simple squamous epithelium, or endothelium. permits a more rapid transport of materials between the blood and the tissues. Make Up of Blood Vessels: Capillaries 6. Capacitance Vessel – Systemic veins Have a large diameter but a thin wall, which includes a thin muscle coat. The number is about twice as much as the number of arteries, The large number and cross sectional area gives them an enormous capacity to hold blood. Capacitance Vessel – Systemic veins Most of the time, veins hold more than half the blood volume . are known as capacitance vessels. the great distensibility of veins makes their capacity adjustable. In times of need, a considerable amount of blood can be squeezed from the veins to areas where it may be needed. II Basic Concept of Hemodynamics: Blood Flow, Resistance of Blood Flow and Blood Pressure 1. Blood Flow (Q) Concept: The quantity of blood that passes a given point in the circulation in a given period of time. The overall blood flow in the systemic circulation is identical to the cardiac output (2) Factors determining blood flow (interrelationships among blood flow, pressure and resistance.) ΔP: the pressure difference between the two ends of the vessels; R: frictional force produced when blood fIows through blood vessels. Q = ΔP / R (3) Laminar flow and turbulent flow Laminar flow – blood flows in streamlines with each layer of blood remaining the same distance from the wall Laminar flow (3) Laminar flow and turbulent flow Turbulent flow – blood flow in all directions in the vessel and continually mixes within the vessel. because of the velocity of blood flow is too great, is passing by an obstruction, making a sharp turn, passing over a rough surface) C, constriction; A, anterograde; R, retrograde 2. Resistance of Blood Flow From Q = ΔP / R (1) we get R = ΔP / Q (2) According to Poiseuille’s law, Q = πΔP r4/8ηl (3) From (3) and (2), we get R = 8 ηl/ π r4 π is constant Note that the resistance (R) of a vessel is directly proportional to the blood viscosity (η) and length (l) of the vessel, but inversely proportional to the fourth power of the radius ( r ). Normally, L and η have no change or almost no change. Therefore, the diameter of a blood vessel plays by far the greatest role of all factors in determining the resistance ( R ) of blood flow. 3. Blood pressure Blood pressure means the force exerted by the blood against the vessel wall ( or the force exerted by the blood against any unit area of the vessel wall) Blood Pressure is stored energy (potential energy) Formation of the blood pressure: (1) Mean circulatory filing pressure (MCFP): when heart beat is stopped, the pressure in any point of cardiovascular system is equal. This pressure is called MCFP systemic circulation, 7 mmHg; pulmonary circulation, 10 mmHg. (2) Total peripheral resistance. Formation of the blood pressure: (3) Cardiac pumping Energy released from heart contraction is transferred into parts, 1) kinetic energy (1% of the total), 2) potential energy (pressure) (99% of the total). That means most part of energy used to create the blood pressure Blood Pressure: Generated by Ventricular Contraction Formation of the blood pressure: (4)Elasticity of Windkessel vessel ① diastolic blood pressure ② continuous blood flow in diastole ③ buffering blood pressure 4. Physical Characteristics of the Systemic Circulation (1)The velocity of blood flow in each segment of the circulation is inversely proportional to its cross-sectional area. 4. Physical Characteristics of the Systemic Circulation (2) Pressure and resistance in the various portion of the systemic circulations. The decrease in pressure in each part of the systemic circulation is directly proportional to the vascular resistance. III. Arterial Pressure 1. Concept of Arterial Pressure Blood pressure in the aorta and other big arterials. 2. Normal Range of Arterial Pressure Systolic pressure (Ps) – the maximum of the pressure during systole Diastole pressure (Pd) – the minimum pressure during diastole Pulse pressure – the difference between Ps and Pd Mean arterial pressure – the average pressure throughout each cardiac cycle. Mean arterial pressure (Pm) = Pd + Pulse pressure / 3 Mean arterial pressure Normal range of arterial pressure At rest, the arterial pressure of Chinese adult young people should be Ps 100 – 120 mmHg Pd 60 – 80 mmHg Pulse pressure 30 – 40 mmHg Measurement of the arterial pressure Direct (inserting a cannula into the artery) Measurement of the arterial pressure Indirect (auscultatory) method Stethoscope Blood Pressure (BP): 3. Factors Determining Arterial Pressure Stroke volume ---- Ps Heart rate ---- Pd Total peripheral resistance (Ps) Action of Windkessel vessel (aorta and other large arteries) – Pulse pressure Mean circulatory filling pressure IV. Venous Pressure and Venous Return Venous Pressure Central venous pressure Peripheral venous pressure Central venous pressure The pressure in the right atrium. Normally about 0 mmHg. Regulated by a balance between the ability of the right ventricle to pump blood out the tendency of blood to flow from the peripheral back into the right atrium. Clinical importance: the hemorrhage right heart failure Peripheral venous pressure Venous pressure in the organs Properties: Low pressure Affected by the hydrostatic pressure Usually veins are collapsed. (Why?) Transmural pressure = Blood pressure - The pressure adjacent tissues exerted on the blood vessel. If the transmural pressure is negative (smaller than 0), the vein is collapsed Venous Return Concept: The quality of blood flowing from veins into the right atrium per minute Factors affecting venous return Mean system filling pressure Cardiac contractility Position of the body Action of “muscular pump” Respiration movement Factors affecting venous return 1) Mean systemic filling pressure 2) Cardiac contractility Cardiac contractility – stroke volume – ventricular pressure in diastole period – blood from atria and large veins to ventricle – venous return 3) Position of the body From lying to standing – increase of the blood in veins – dilation of veins in the lower part of the body – decrease of venous return Factors affecting venous return 4) Action of “muscular pump” (or venous pump) Factors affecting venous return (5) respiration movement. Negative pressure in the thoracic cavity that changes with respiratory movement – dilation of venae cave – increase of venous return V Microcirculation 1.Functional anatomy of the microcirculation 2. “pores” in the capillary membrane A A, Continuous Capillaries B B, Fenestrated Capillary 2. “pores” in the capillary membrane Structurally, capillaries have no smooth muscle in their walls. They are lined by only a single layer of endothelial cells. There are gaps between endothelial cells to allow for exchange of nutrients and metabolites. 3. Capillary pressure. Arterial end 30 – 40 mmHg; Venous end, 10 – 15 mmHg; Middle part 25 mmHg 4. Exchange of nutrients and other substances between the blood and interstitial fluid (1) Diffusion through the capillary membrane. Lipid-solute substance can diffuse directly through the cell membranes of the capillary Water-soluble, liquid-insoluble substance, such as Na , Cl, glucose and so forth, diffuse only through the capillary pores. 4. Exchange of nutrients and other substances between the blood and interstitial fluid (2) Transport through the capillary membrane by pinocytosis. Proteins and many much large substance in the plasma (such as lipoprotein) are transported through the capillary membrane by means of pinocytosis. (3) Filtration. When the hydrostatic pressure is different on the two sides of membrane, the greater pressure on one side causes slightly increased diffusion of water and dissolved substances toward the opposite side. VI The Interstitial Fluid Water within the body accounts for 60% of the total body weight (body fluid) 2/3 intracellular compartment 1/3 extracellular compartment 80%, interstitial fluid; 20%, blood plasma The distribution of extracellular fluid between the plasma and interstitial compartments is in a state of dynamic equilibrium. Tissue fluid is not normally a “stagnant pond” but is rather a continuously circulating medium, formed from and returning to the vascular system. In this way, the tissue cells receive a continuously fresh supply of glucose and other plasma solutes that are filtered through tiny endothelial channels in the capillary walls The daily intake and excretion of body water and its distribution between different intracellular and extracellular compartment 1. Formation of the interstitial fluid • Effective Filtration Pressure = (Capillary Pressure + Interstitial Colloid Osmotic Pressure) – (Plasma Colloid Osmotic Pressure + Interstitial Hydrostatic Pressure) (crystal pressure?) 2. Factors Determining Formation of the Interstitial Fluid (Mechanism of Edema) Edema is an abnormally large collection of fluid in the interstitial space. From the physiology of capillaries and lymphatics, edema may be due to one or more of the following causes: Mechanism of Edema (1) Capillary pressure Right heart failure –systemic edema Left heart failure – pulmonary edema Late pregnancy – edema in legs and foot (pressure of uterus on inferior vena cava) Mechanism of Edema (2) Plasma colloid osmotic pressure Protein malnutrition, liver disease (inadequate albumin synthesis ) or renal disease (protein loss in urine) – hypoproteinemia – low plasma colloid osmotic pressure (3) Permeability of capillary wall Inflammation or allergy – leakage of abnormally large quantities of proteins from capillaries Mechanism of Edema • (4) Lymphatic drainage • Lymphatics are the second circulatory system. • Structurally, lymphatics are a network of blindended thin endothelial tubes. • Although the endothelial lining is not fenestrated, • the intercellular junctions are permeable to large molecules. Mechanism of Edema (4) Lymphatic drainage (continued) Lymphatics collect proteins, lipids and other large molecules which leak out of capillaries into the interstitial space, to prevent the osmotic pressure of interstitial space from rising, and thereby prevent abnormal accumulation of fluid in the interstitial space. Reduced lymphatic drainage, e.g. in filariasis, or involvement of lymph nodes in malignancy – local or systemic edema. 3. The function of lymph Removing protein from interstitial fluid. Regulating balance between plasma and interstitial fluid (reabsorption l0% of filtration fluid). Absorption nutrients (80%~90% of fat) from gastrointestinal tract. Removing the particles such as RBC, bacteria, lymphatic cell, tissue cell in the interstitium. Defense function (to ingest bacteria and to produce antibodies)