POSTER CARS 2002
advertisement

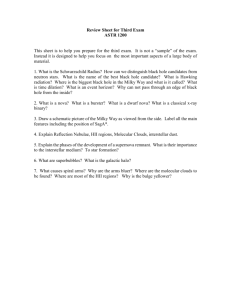
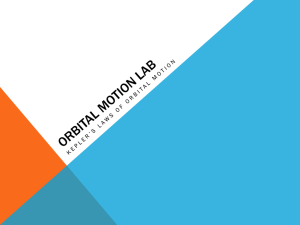
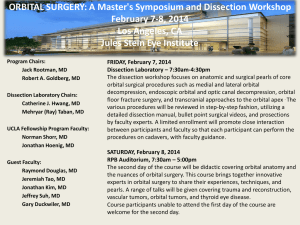
Evaluation of the exophthalmia reduction with a finite element model Luboz Vincent*, Pedrono Annaig**, Boutault Franck***, Swider Pascal**, Payan Yohan* *TIMC-IMAG Laboratory, GMCAO **INSERM, Biomechanic laboratory ***CHU Purpan, Maxillo facial surgery Summary The exophthalmia is a pathology defined by an excessive forward protrusion of the ocular globe [1] due to an increase of the orbital content behind the globe. Besides aesthetical and psychological consequences, exophthalmia has functional consequences, such as a too long cornea exposition and sometimes a distension of the ocular nerve. For disthyroidy exophthalmia, a surgery is usually needed, once the endocrinal situation has been stabilized. A classical surgical technique consists in decompressing the orbit [2] by the mean of an orbital walls osteotomy, and pushing the ocular globe in order to evacuate some of the fat tissues inside the sinuses. The planning of this osteotomy consists in defining the size and the location of the decompression hole. This gesture is very delicate and could be assisted in a computer-aided framework. A biomechanical model of the orbital soft tissues and its interactions with the walls are provided here, in order to help surgeons in the definition of the planning. The model is defined by a generic Finite Element poro-elastic mesh of the orbit, including the fat tissues and the walls. This generic model is automatically adapted to the morphologies of four patients, extracted from TDM exams. Four different FE models are then generated and used to simulate osteotomies in the maxillary or ethmoid sinuses regions. Heterogeneous results are observed, with different backwards movements of the ocular globe according to the size and/or the location of the hole. (1) Definition of the generic FE model of the orbital cavity: (a) (b) (c) (a) Segmentation of CT scan data to get the external surface of the orbital cavity. (b) Geometric reconstruction of the orbital cavity, the muscles and the ocular nerve from the splines segmented in (a) (c) Manual definition of the generic FE mesh of the orbit The model is considered to be homogeneously composed of soft tissues (fat and muscles) and is modelled with a poro elastic material. E=20kPa, =0.4 [3]. (2) Simulation of the orbital decompression: Boundary conditions: (a) A strength of 10N is applied to elements in contact with the globe to model the backward displacement (which correspond to a pressure of 20kPa at each node). (b)Nodes of the hole area are free to move to simulate the decompression in the sinuses. (c) Others nodes cannot move since the bone surrounding the orbital cavity is rigid enough to support the surgeon gesture. (d)An initial pressure of 10kPa is applied to the liquid in the poro-elastic material to take into account the increase of the soft tissues volume before the surgery. Result: the strength imposed to the eye contact elements induced a hernia (in blue) visible on the hole elements. With this medium hole, the globe has a 3.1mm backward movement and a fat tissue volume of approximately 2.2cm3 is decompressed. (3) Patient conformation and experimentation: Besides this first hole behind (called medium hole at the front of the orbit), 3 other holes are simulated: (a) a big hole at the front of the orbit, (b) a big hole at the back and (c) a medium hole at the back. Medium holes have an area of 1.4cm2 and big holes have an area of 2.9cm2. (a) 5 4 3 2 BigHoleFront 1 MedHoleFront BigHoleBack MedHoleBack 0 0 0,005 0,01 0,015 pressure on the globe (MPa) 0,02 Knowing that the big hole at the front of the orbital cavity is a good solution, 4 patients meshes have been generated automatically with the Mesh Matching algorithm [5]. Significant variations of the volume of soft tissues evacuated through this hole are obtained (a variation of 10% between patient ZJ and FJ). Those variations may result from patient geometric heterogeneities. (c) 3,5 volume of fat tissues decompressed (cm3) For the same load case, the behaviour of the orbital soft tissues depends on the four hole sizes and locations. The higher backward displacement (close to data reported in [4]) is obtained with the big hole (a), showing that this size and position of hole is the most efficient choice for an orbital decompression (with a 10% to 40% increase of the backward displacement). 6 globe backward displacement (mm) (b) 3 2,5 2 1,5 1 patientBJ patientFJ 0,5 patientLF patientZJ 0 0 0,005 0,01 0,015 0,02 pressure on the globe (MPa) References [1] Maus M., 1994. Basic anatomy of the orbit. Albert, DM, Jakobiec, FA, eds. Principles and Practice of Ophthalmology: Clinical Practice. Philadelphia: W.B. Saunders, vol. 3, pp. 1871-1880. [2] Wilson W.B., Manke W.F., 1991. Orbital decompression in Graves’ disease. The predictability of reduction of proptosis. Arch. Ophthalmol., vol. 109, pp. 343-345. [3] Fung, Y.C., 1993. Biomechanics: Mechanical Properties of Living Tissues. New York: Springer-Verlag [4] Jin H.R., Shin S.O., Choi Y.S, 2000. Relationship between the extent of fracture and the degree of enophthalmos in blowout fractures of the medial orbital wall. J. Oral Maxillofacial Surgery. vol. 58, pp 617-620. [5] Couteau B., Payan Y. and Lavallée S., 2000. The Mesh-Matching algorithm : an automatic 3D mesh generator for finite element structures, Journal of Biomechanics, vol. 33/8, 1005-1009.