Hepatic encephalopathy (cont'd)
")
Focus on
Cirrhosis of the Liver
(Relates to Chapter 44,
“Nursing Management:
Liver, Pancreas, and Biliary Tract Problems” in the textbook)
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Description
• A chronic progressive disease of the liver
Extensive parenchymal cell degeneration
Destruction of parenchymal cells
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
2
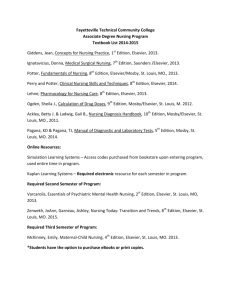
Cirrhosis
Fig. 44-4. Cirrhosis that developed secondary to alcoholism. The characteristic diffuse nodularity of the surface is due to the combination of regeneration and scarring of the liver.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
3
Description
• Liver cells attempt to regenerate.
Regenerative process is disorganized.
• Abnormal blood vessel and bile duct formation
• New fibrous connective tissue distorts liver’s normal structure, impedes blood flow.
• Poor cellular nutrition and hypoxia result.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
4
Description
• Insidious, prolonged course
• Ninth leading cause of death in
United States
• Fourth leading cause of death in persons ages 35 to 54
• Twice as common in men
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
5
Etiology and Pathophysiology
• Factors that can lead to cirrhosis
Chronic alcohol abuse
• Excessive alcohol ingestion is the single most common cause of cirrhosis.
• Alcohol has a direct hepatotoxic effect.
• First change from excessive alcohol intake is fat accumulation in liver cells.
• With continued abuse, scar formation occurs.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
6
Etiology and Pathophysiology
Nonalcohol fatty liver disease (NAFLD)
Malnutrition that occurs concurrently with excessive alcohol intake, extreme dieting, malabsorption, and obesity
Environmental factors, as well as a genetic predisposition
Postnecrotic cirrhosis
• Complication of viral, toxic, or idiopathic hepatitis
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
7
Etiology and Pathophysiology
Biliary cirrhosis
• Associated with chronic biliary obstruction
• Diffuse fibrosis of liver with jaundice
Cardiac cirrhosis
• From long-standing severe right-sided heart failure
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
8
Clinical Manifestations
Early manifestations
• Onset usually insidious
• GI disturbances:
Anorexia
Dyspepsia
Flatulence
Nausea/vomiting
Change in bowel habits
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
9
Clinical Manifestations
Early manifestations (cont’d)
• Abdominal pain
• Fever
• Lassitude
• Weight loss
• Enlarged liver or spleen
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
10
Clinical Manifestations
Late manifestations
• Two causative mechanisms
Hepatocellular failure
Portal hypertension
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
11
Pathophysiology of Cirrhosis
Fig. 44-5. Continuum of liver dysfunction in cirrhosis and resulting manifestations. ADH,
Antidiuretic hormone; ALT, alanine aminotransferase; AST, aspartate transaminase.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
12
Clinical Manifestations
Fig. 44-6. Systemic clinical manifestations of liver cirrhosis.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
13
Clinical Manifestations
Late manifestations (cont’d)
• Jaundice
Decreased ability of liver cells to conjugate and excrete bilirubin
Functional derangement of liver cells
Compression of bile ducts by overgrowth of connective tissue
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
14
Clinical Manifestations
Jaundice (cont’d)
Minimal or severe, depending on liver damage
Late stages of cirrhosis
• Patient usually will be jaundiced.
If biliary tract obstructed, pruritus can occur.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
15
Clinical Manifestations
• Skin lesions
Due to increase in circulating estrogen caused by inability of liver to metabolize steroid hormones
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
16
Clinical Manifestations
• Skin lesions (cont’d)
Spider angiomas
• Small dilated blood vessels with bright red center and spiderlike branches
• Nose, cheeks, upper trunk, neck, shoulders
Palmar erythema
• Red area on palms of bands that blanches with pressure
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
17
Clinical Manifestations
• Endocrine disorders
Steroid hormones of the adrenal cortex, testes, and ovaries are metabolized and inactivated by the normal liver.
Damaged liver is unable to metabolize these hormones, and various manifestations occur.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
18
Clinical Manifestations
• Hematologic disorders
Splenomegaly
• From backup of blood from portal vein
Bleeding tendencies
• Decreased production of hepatic clotting factors
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
19
Clinical Manifestations
• Peripheral neuropathy
Dietary deficiencies of thiamine, folic acid, and cobalamin (vitamin B
12
)
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
20
Complications
• Portal hypertension
• Esophageal and gastric varices
• Peripheral edema and ascites
• Hepatic encephalopathy
• Hepatorenal syndrome
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
21
Complications
Portal hypertension
• Characterized by
Increased venous pressure in portal circulation
Splenomegaly
Ascites
Large collateral veins
Esophageal varices
Systemic hypertension
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
22
Complications
Portal hypertension (cont’d)
• Primary mechanism is increased resistance to blood flow through the liver.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
23
Complications
Portal hypertension (cont’d)
• Esophageal varices
Complex of tortuous veins at lower end of esophagus
Develop in areas where collateral and systemic circulations communicate
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
24
Complications
• Esophageal varices (cont’d)
Contain little elastic tissue and are fragile
Bleeding esophageal varices
• Most life-threatening complication of cirrhosis
80% of variceal hemorrhages
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
25
Complications
Portal hypertension (cont’d)
• Gastric varices
Located in upper portion of stomach
20% of variceal hemorrhages
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
26
Complications
Portal hypertension (cont’d)
• Internal hemorrhoids
Occur because of the dilation of the mesenteric veins and rectal veins
• Caput medusae
Ring of varices around the umbilicus
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
27
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
28
Complications
Peripheral edema and ascites
• Edema
↓ Colloidal oncotic pressure from impaired liver synthesis of albumin
↑ Portacaval pressure from portal hypertension
Occurs as ankle/presacral edema
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
29
Complications
Peripheral edema and ascites (cont’d)
• Ascites
Accumulation of serous fluid in peritoneal or abdominal cavity
Abdominal distention with weight gain
Common manifestation of cirrhosis
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
30
Ascites
Fig. 44-7. Mechanisms for development of ascites.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
31
Gross Ascites
Fig. 44-8. Gross ascites.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
32
Complications
• Ascites (cont’d)
Factors involved in the pathogenesis
• ↓ Serum colloidal oncotic pressure
• ↑ Levels of aldosterone
• Portal hypertension
• ↑ Flow hepatic lymph
• Impaired water excretion
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
33
Complications
Hepatic encephalopathy
• Neuropsychiatric manifestation
• Terminal complication in liver disease
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
34
Complications
Hepatic encephalopathy (cont’d)
• Etiologic factors
Disorder of protein metabolism and excretion
• Liver unable to convert ammonia to urea, or blood shunted past liver through, so ammonia stays in systemic circulation
• Ammonia crosses blood-brain barrier and causes neurologic toxic manifestations.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
35
Complications
Hepatic encephalopathy (cont’d)
• Etiologic factors (cont’d)
Altered astrocyte function
• Regulate blood-brain barrier and detoxification of ammonia
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
36
Complications
Hepatic encephalopathy (cont’d)
• Clinical manifestations
Changes in neurologic and mental responsiveness
• Ranging from sleep disturbance to lethargy to deep coma
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
37
Complications
Hepatic encephalopathy (cont’d)
• Grading system used to classify stages
Stages 0 through 4
4 is most advanced.
• Asterixis
Characteristic symptom
Flapping tremors involving arms and hands
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
38
Complications
Hepatic encephalopathy (cont’d)
• Fetor hepaticus
Musty, sweet odor on patient’s breath
Accumulation of digestive by-products that liver is unable to degrade
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
39
Complications
Hepatorenal syndrome
• Serious complication of cirrhosis
• Functional renal failure with
Azotemia
Oliguria
Intractable ascites
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
40
Complications
Hepatorenal syndrome (cont’d)
• No structural abnormality of kidney
• Splanchnic and systemic vasodilation and ↓ arterial blood volume
Renal vasoconstriction occurs with renal failure.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
41
Diagnostic Studies
• History/physical examination
• Laboratory tests
Liver function tests
Serum electrolytes
CBC
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
42
Diagnostic Studies
• Laboratory tests (cont’d)
Prothrombin time
Serum albumin
Stool for occult blood
Analysis of ascitic fluid
• Liver biopsy
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
43
Collaborative Care
• Rest
• Administration of B-complex vitamins
• Avoidance of alcohol, aspirin, acetaminophen, and NSAIDs
• Management of ascites
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
44
Collaborative Care
• Prevention and management of esophageal variceal bleeding
• Management of encephalopathy
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
45
Collaborative Care
• Ascites
High-carbohydrate, low-Na + diet
(2 g/day)
Diuretics
Paracentesis
• Removes fluid from abdominal cavity
• Temporary measure
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
46
Collaborative Care
• Ascites (cont’d)
Peritoneovenous shunt
• Continuous reinfusion of ascitic fluid from the abdomen to the vena cava
• Not first-line therapy
• Complications : Thrombosis, infection, fluid overload, DIC
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
47
Collaborative Care
• Esophageal and gastric varices
Goal: Avoid bleeding/hemorrhage
Avoid alcohol, aspirin, and irritating foods.
Respiratory infection promptly treated
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
48
Collaborative Care
If bleeding occurs, stabilize patient, manage airway, provide IV therapy.
Drug therapy may include
• Octreotide (Sandostatin)
• Vasopressin (VP, Terlipressin)
• Nitroglycerin (NTG)
• β-adrenergic blockers
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
49
Collaborative Care
• Endoscopic sclerotherapy
Treatment for acute/chronic bleeding varices
Agent (morrhuate [Scleromate])
• Thromboses and obliterates distended veins
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
50
Collaborative Care
• Endoscopic ligation
Banding of varices
Fewer complications than sclerotherapy
• Balloon tamponade
Controls hemorrhage by compression of varices
Uses Sengstaken-Blakemore tube
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
51
Sengstaken-Blakemore Tube
Fig. 44-9. A, Sengstaken-Blakemore tube. B, Tube inserted into esophagus and stomach.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
52
Collaborative Care
• Supportive measures for acute bleed
Fresh frozen plasma
Packed RBCs
Vitamin K
Histamine receptor blockers
Proton pump inhibitors
Lactulose (Cephulac)
Neomycin
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
53
Collaborative Care
• Long-term management
β-adrenergic blockers
Repeated sclerotherapy/band ligation
Portosystemic shunts
Propranolol (Inderal)
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
54
Collaborative Care
• Shunting procedures
Used more after second major bleeding episode
Surgical vs. nonsurgical
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
55
Collaborative Care
• Nonsurgical procedure
Transjugular intrahepatic portosystemic shunt (TIPS)
• Tract (shunt) between systemic and portal venous system
• Used to redirect portal blood flow
• Decreases portal venous pressure and decompresses varices
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
56
Total Portal Division After TIPS
Fig. 44-10. Total portal diversion after transjugular intrahepatic portosystemic shunt (TIPS). A, Portal venogram before TIPS shows filling of large esophageal varices (arrows). B, After insertion of a TIPS, flow to varices is eliminated. Intrahepatic portal vein flow is now reversed, with the direction of intrahepatic flow toward the TIPS.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
57
Collaborative Care
• Surgical procedures
Portacaval shunt
• Decreases bleeding episodes
• Does not prolong life; patient dies of hepatic encephalopathy
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
58
Portosystemic Shunts
Fig. 44-11. Portosystemic shunts. A, Portacaval shunt. The portal vein is anastomosed to the inferior vena cava, diverting blood from the portal vein to the systemic circulation. B, Distal splenorenal shunt. The splenic vein is anastomosed to the renal vein. The portal venous flow remains intact while esophageal varices are selectively decompressed. (The short gastric veins are decompressed.) The spleen conducts blood from the high pressure of the esophageal and gastric varices to the low-pressure renal vein.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
59
Collaborative Care
• Surgical procedures (cont’d)
Distal splenorenal shunt (Warren shunt)
• Leaves portal venous flow intact
• ↓ Incidence of hepatic encephalopathy
• With time, blood flow to liver ↓
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
60
Collaborative Care
• Hepatic encephalopathy
Goal: Decrease ammonia formation
• Sterilization of GI tract with antibiotics
(e.g., neomycin)
• Lactulose (Cephulac) traps NH3 in gut.
• Cathartics/enemas
Treatment of precipitating cause
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
61
Collaborative Care
• Drug therapy
No specific drug therapy
Drugs are used to treat symptoms and complications of advanced liver disease.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
62
Nutritional Therapy
• Diet for patient without complications
High in calories (3000 kcal/day)
↑ carbohydrate
Moderate to low fat
Protein restriction rarely justified
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
63
Nutritional Therapy
• Protein supplements if proteincalorie malnutrition
• Low-sodium diet for patient with ascites and edema
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
64
Nursing Management
Nursing Assessment
• Past health history
Chronic alcoholism
Viral hepatitis
Chronic biliary disease
• Physical examination
• Medications
• Weight loss
• Jaundice
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
65
Nursing Management
Nursing Assessment
• Abdominal distention
• Nausea/vomiting
• Altered mentation
• RUQ pain
• Abnormal laboratory values
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
66
Nursing Management
Nursing Diagnoses
• Imbalanced nutrition: Less than body requirements
• Impaired skin integrity
• Ineffective breathing pattern
• Excess fluid volume
• Dysfunctional family processes:
Alcoholism
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
67
Nursing Management
Planning
• Overall goals
Relief of discomfort
Minimal to no complications
Return to as normal a lifestyle as possible
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
68
Nursing Management
Nursing Implementation
• Health promotion
Treat alcoholism.
Identify hepatitis early and treat.
Stress importance of adequate nutrition.
Identify biliary disease early and treat.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
69
Nursing Management
Nursing Implementation
• Acute intervention
Rest
Oral hygiene
Between-meal nourishment
Explanation of dietary restrictions
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
70
Nursing Management
Nursing Implementation
• Acute intervention (cont’d)
Accurate I/O
Daily weights
Abdominal girth
• Kneeling position, if possible
Extremities measurement
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
71
Nursing Management
Nursing Implementation
• Acute intervention (cont’d)
Paracentesis
• Patient void immediately before
• High Fowler’s or side of bed
• Monitor for electrolyte imbalances.
• Monitor dressing for bleeding/leakage.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
72
Nursing Management
Nursing Implementation
• Acute intervention (cont’d)
Check respiratory status frequently.
• Semi- or high Fowler’s
Skin care
• Turning schedule, at least every 2 hours
ROM exercises
Coughing/deep breathing exercises
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
73
Nursing Management
Nursing Implementation
• Acute intervention (cont’d)
Monitor for electrolyte disturbances.
• Diuretic therapy alters electrolytes.
• Hypokalemia
• Cardiac dysrhythmias, hypotension, tachycardia, muscle weakness
Observe for bleeding disorders.
Always be a supportive listener.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
74
Nursing Management
Nursing Implementation
• Acute intervention (cont’d)
Bleeding varices
• Close observation for signs of bleeding
• Balloon tamponade care
• Explanation of procedure
• Check for patency.
• Position of balloon verified by x-ray
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
75
Nursing Management
Nursing Implementation
• Acute intervention (cont’d)
• Balloon tamponade (cont’d)
• Saline lavage/NG suction to remove blood
• Monitor for complications (i.e., aspiration pneumonia).
• Scissors at bedside
• Semi-Fowler’s position
• Oral/nasal care
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
76
Nursing Management
Nursing Implementation
• Acute intervention (cont’d)
Hepatic encephalopathy
• Maintain safe environment.
• Assess carefully.
• Level of responsiveness
• Sensory and motor abnormalities
• Fluid/electrolyte imbalances
• Acid-base balance
• Effects of treatment measures
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
77
Nursing Management
Nursing Implementation
• Acute intervention (cont’d)
Hepatic encephalopathy (cont’d)
• Neurologic assessment every 2 hours
• Prevention of constipation
• Limited physical activity
• Control of hypokalemia
• Ensuring proper nutrition
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
78
Nursing Management
Nursing Implementation
• Ambulatory and home care
Symptoms of complications
Written instructions with adequate explanations for patient/family
When to seek medical attention
Remission maintenance
Abstinence from alcohol
Caring attitude always
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
79
Nursing Management
Evaluation
• Maintenance of food/fluid intake to meet needs
• Maintenance of muscle tone and energy
• Maintenance of skin integrity
• Normalization of fluid balance
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
80
Nursing Management
Evaluation
• Maintenance of blood pressure and urinary output
• Reports increased ease of breathing
• Experiences normal respiratory rate/rhythm
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
81
Audience Response Question
A patient with advanced cirrhosis with ascites is short of breath and has an increased respiratory rate. The nurse should:
1. Initiate oxygen therapy at 2 L/min to increase gas exchange.
2. Notify the health care provider so a paracentesis can be performed.
3. Ask patient to cough and deep breathe to clear respiratory secretions.
4. Place the patient in Fowler’s position to relieve pressure on the diaphragm.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
82
Case Study
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
83
Case Study
• 35-year-old woman was admitted with hepatic coma.
• History of numerous hospitalizations since age 19
Usually for psychosomatic and nervous disorders
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
84
Case Study
• Denies alcoholism and having more than 3 oz of alcohol per day
States “the girls and I have social drinks”
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
85
Case Study
• Review of old medical records shows progressive weakness, weight loss, anorexia, jaundice, edema, ascites, and mental disorientation.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
86
Case Study
• Accepts treatment only during crises
• Upon admission, she is stuporous and hypotensive, and has twitching and asterixis.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
87
Case Study
• She is thin and malnourished with marked edema on lower extremities and ascites.
• Liver and spleen are both palpable.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
88
Case Study
• Jaundice and spider angiomas are present.
• Evidence of bruising throughout body
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
89
Case Study
• Previous liver biopsies indicated
At age 29, fatty liver
At age 31, cirrhosis with hyaline necrosis
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
90
Case Study
• Laboratory values
Total bilirubin 11 mg/dL
AST 80 U/mL
ALT 70 U/mL
LDH 700 U/mL
Serum ammonia 220 mg/dL
WBC 21,450/uL
Hematocrit 24%
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
91
Discussion Questions
1.
What clinical manifestations of cirrhosis does she have?
2.
Explain the results of her diagnostic findings.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
92
Discussion Questions
3.
What is the priority of care for her?
4.
What patient and family teaching is essential?
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
93