The Present and Future Role of
Biomarkers in Clinical Development
A Partnership Journey towards Precision Medicine
Presented by
Sponsored by
Copyright © 2015, Oracle and/or its affiliates. All rights reserved. |
Welcome & Introductions
Moderators
• Robert A. Lindberg, PhD, RAC Senior Director, Technology Transfer and Entrepreneur
Programs
• MaryAnne Rizk, PhD Global VP, CRO Business Partnerships & Alliances, Oracle Health
Sciences
Speakers
• Jeffrey Shuster, PhD - General Manager at the Biomarker Factory
• Thomas Turi, PhD - Vice President of Science & Technology for Covance Central
Laboratory Services
• Thomas Povsic, M.D., PhD - Associate Professor of Medicine at Duke University Medical
Center
• James Streeter – Global Vice President, Life Science Strategy
Copyright
Oracle ©
Confidential
2015, Oracle
– Internal/Restricted/Highly
and/or its affiliates. All rights
Restricted
reserved. |
2
The Present and Future Role of
Biomarkers in Clinical Development
• Importance of Biomarkers in Clinical Trials and Precision Medicine
– Cost to Develop New Pharmaceutical Drug Now Exceeds $2.5B
– Fit-for-Purpose: How Biomarkers Can Be Leveraged to Improve Return on Investment
(ROI) in Drug Development
• Getting Precise on Precision Medicine
– Patient Stratification
• The Collaboration & Partnership Journey
– Innovation Solutions to accelerate Drug Development
– Leveraging CROs and Sponsor Engagement Strategies
Copyright
Oracle ©
Confidential
2015, Oracle
– Internal/Restricted/Highly
and/or its affiliates. All rights
Restricted
reserved. |
3
Cost of drug development has increased in recent years
According to PhRMA1:
• –In 1970, the average cost to develop a drug (including failures) was $140M
• –In late 1990s, the cost was $800M
• –In early 2000s, cost was $1.2B
• 10-15 years from discovery to the marketplace
According to a 2013 article in FORBES2:
• –The cost to develop a drug is as high as $5B
1 http://www.phrma.org/sites/default/files/pdf/PhRMA%20Profile%202013.pdf
2 http://www.forbes.com/sites/matthewherper/2013/08/11/how-the-staggering-cost-of-inventing-new-drugs-is-shaping-the-future-of-medicine/
Copyright
Oracle ©
Confidential
2015, Oracle
– Internal/Restricted/Highly
and/or its affiliates. All rights
Restricted
reserved. |
4
Why is the cost of drug development going up?
High failure rate
– 5,000 to 10,000 compounds enter the pipeline for every 1 FDA-approved medicine1
– Even medicines that reach clinical trials have only a 16% chance of being approved. 2
Clinical trials are becoming more complex, less likely to succeed.
• Personalized medicine and accompanying diagnostics development
• more procedures, more data, more numerous and complex eligibility criteria for
enrollment, longer study duration. 3
Difficulty recruiting volunteers extends the original timeline of phase 2 to 4 trials by
nearly double on average across all therapeutic areas.4
– 1 http://www.phrma.org/sites/default/files/pdf/PhRMA%20Profile%202013.pdf
– 2 Tufts Center for the Study of Drug Development. “Large Pharma Success Rate for Drugs Entering Clinical Trials in 1993–2004: 16%.”
– Impact Report 2009; 11(4
– 3 K.A. Getz, R.A. Campo, and K.I. Kaitin. “Variability in Protocol Design Complexity by Phase and Therapeutic Area.” Drug Information Journal 2011; 45(4): 413–420.
– 4 Tufts Center for the Study of Drug Development. “89% of Trials Meet Enrollment, but Timelines Slip, Half of Sites Under-Enroll.” Impact Report 2013; 15(1).
Copyright
Oracle ©
Confidential
2015, Oracle
– Internal/Restricted/Highly
and/or its affiliates. All rights
Restricted
reserved. |
5
Reduced profits after approval
• Fierce competition reduces revenue after approval
• After FDA approval, the average effective patent life
of a brand name medicine is about 12 years
• Only 2 of every 10 brand name medicines earn
sufficient revenues to recoup average R&D costs
1 H.G. Grabowski, et al. “Evolving Brand-name and Generic Drug Competition may Warrant a Revision of the Hatch-Waxman Act.” Health Affairs 2011; 30(11): 2157–2166.
2 J.A. Vernon, J.H. Golec, and J.A. DiMasi. “Drug Development Costs When Financial Risk is Measured Using the Fama-French Three-factor Model.” Health Economics 2009;
19(8): 1002–1005.
Copyright
Oracle ©
Confidential
2015, Oracle
– Internal/Restricted/Highly
and/or its affiliates. All rights
Restricted
reserved. |
6
How can use of biomarkers increase ROI?
• “Biomarker” = a laboratory measurement that reflects the activity of a disease process1
• Quantitatively correlates with disease progression.
• Examples include:
–
–
–
–
Blood pressure
Cholesterol
Fasting glucose
Positron emission tomography (PET)
• –Magnetic resonance imaging (MRI)
1 Russell Katz, Biomarkers and Surrogate Markers: An FDA Perspective, NeuroRx, Apr 2004; 1(2): 189–195. doi:
10.1602/neurorx.1.2.189
Copyright
Oracle ©
Confidential
2015, Oracle
– Internal/Restricted/Highly
and/or its affiliates. All rights
Restricted
reserved. |
7
Importance of Biomarkers in Clinical
Trials and Precision Medicine
Bringing Biomarkers to Clinical Practice
Jeffrey Shuster, PhD
jshuster@biomarkerfactory.com
Translational Medicine in Diagnostics
A diagnostic is of use if it changes clinical practice.
Biomarkers in Clinical Practice
Utilities of Biomarkers
Disease diagnosis
Prognosis, for selection of treatment
Predictive, for optimizing therapy
Companion diagnostics
Studies must identify and validate
biomarkers in clinical materials
Specimen obtainment and assay
technology must be suitable for
use in clinical practice
Areas of Interest for Biomarkers
Chronic disease
Cardiovascular
Diabetes
Mental health
Cancer
Arthritis
Autoimmune diseases
Health
Acute illness
Nutrition
Aging
Microbiomes
Immune system functions
Performance training
Cardiovascular events
Infectious disease
Cancer
Toxicology
Trauma
Translational Medicine in Diagnostics
Biomarker Study Components
Four Questions
1. Clinical need
What is the medical need for a new test over and above current clinical practice?
2. Patient population to be tested
What patient criteria will a physician use to order the test?
3. Actionable in clinical practice
Based on the test result, what will the physician do differently than he/she does today?
4. Number of patients
How many patients are estimated to be tested and how often?
Bringing Biomarkers to Clinical Practice
A diagnostic is of use if it changes clinical practice.
A focus on the utility of the biomarker
Diagnostic, prognostic, predictive, or companion
Screening in the general population
Screening in at risk populations
Diagnosis in symptomatic patients
Patient stratification to prescribe drug treatment
Drug efficacy
Drug side effects/toxicity
One biomarker may have more than one utility and
can be used in multiple tests and product lines.
Example - Focus on the utility of the biomarker
Prostate-Specific Antigen (PSA) Biomarker for Prostate Cancer
1979: Discovery of PSA (Wang et al., Invest. Urol. 17:159-63)
1980: PSA levels in serum as a biomarker of prostate cancer (Kuriyama et al., Cancer Res. 40:4658-62)
1986: FDA approval for PSA test as a monitoring test for patients already diagnosed with prostate cancer
1994: FDA approval for PSA test (with DRE) as a screening test for prostate cancer in asymptomatic men
Experimental Design
Have the right specimens, and have enough of them
Pre-define the target patient population
Do not settle for samples of convenience
o You cannot make a good test with bad specimens
Make sure you understand all possible confounding variables
Understand the possible limitations of retrospective studies
Quality assurance for all samples in experimental design
Understand potential regulatory affairs issues up front
In translational work, very careful attention to
detail is necessary in sourcing specimens
Example - Experimental Design
Attention to detail is necessary in sourcing specimens
Biomarkers for Early Detection of Ovarian Cancer
Discovery Experimental
Design, Case-control,
Cancer vs. non-cancer*
Test Utility for Early Detection,
≤ 12 months before Diagnosis**
Reported Reported
Sensitivity Specificity
Study 1
100.0
95.0
Study 2
86.5
93.0
Study 3
95.3
99.4
Study 4
74.0
97.0
Petricoin et al., Lancet. 2002, 359(9306):572-7
2. Gorelik et al., Cancer Epidemiol Biomarkers Prev. 2005, 14(4):981-7
3. Visintin et al., Clin Cancer Res. 2008, 14(4):1065-72
4. Zhang et al. Cancer Res. 2004, 64(16):5882-90
*1.
Sensitivity
at 95%
Specificity
CA125
64.6
95.0
Panel A
32.8
95.0
Panel B
64.6
95.0
Panel C
25.4
95.0
Panel D
52.3
95.0
**ref. Cancer Prev Res 2011;4 (3)
Consider Design Options Early
Enlist biostatisticians throughout the discovery phase
Plan biomarker discovery as close to clinical specimens as possible
If the test will need clinical parameters
Include the clinical parameters in the discovery phase
Does the new test out-perform current state of care
Sensitivity, specificity, PPV, NPV
ROC analysis, area under the curve
Calibration, reclassification
Costs of false positive and false negative results
Test Performance
Gold Standard
Positive
Negative
Sensitivity = TP / (TP+FN)
Specificity = TN / (TN+FP)
TP
FP
PPV = TP / (TP+FP)
NPV = TN / (TN+FN)
Negative
Test Result
Positive
FN
TN
Rule In test [high specificity]
Rule Out test [high sensitivity]
Test performance requirements are based on the medical need.
What is the consequence of a false positive test ? Of a false negative?
Sensitivity, Specificity, and
Positive and Negative Predictive Values
If the test has
PPV
- NPV > 20 years of age
Diabetes screening
in patients
1.00
0.95
95% sensitivity
0.90
1.20
0.85
0.80
95% specificity
Ovarian cancer screening in asymtomatic womenPPV
age 50NPV
1.10
0.75
0.70
1.00
0.65
0.55
Positive Predictive
Value = 0.70
0.80
0.50
0.70
0.45
0.40
0.60
0.35
0.30
0.50
0.25
0.40
0.20
0.15
Positive Predictive
Value = 0.004
0.30
0.10
0.05
0.20
100%
95%
90%
85%
NPV
0.0100
PPV
80%
75%
70%
65%
60%
55%
50%
45%
35%
30%
25%
40%
Prevalence
0.0010
0.0001
0.00
20%
10%
0.10
15%
0.00
5%
or like this:
0.90
0.60
0%
it looks like this:
Biomarkers in Clinical Trials
A Few Preliminary Questions on the
Use of Biomarkers in Clinical Trials
At what stage of your clinical trial would you use a biomarker?
Would you use a non-validated biomarker in a clinical trial?
Would you not use a validated biomarker in a clinical trial?
Clinical Trials with Biomarkers
Some metrics
Year first received
Trials with "biomarker"
2015 (to June 30, 2015)
2014
2013
2012
2011
2010
2009
2008
2007
2006
2005
2004
2003
2002
2001
2000
Trials
1035
2100
1835
1685
1616
1625
1618
1341
1092
860
795
178
124
115
96
91
Percent with
"biomarker"
11598
8.9%
23270
9.0%
20444
9.0%
19639
8.6%
18228
8.9%
17736
9.2%
17156
9.4%
17020
7.9%
13397
8.2%
10932
7.9%
12907
6.2%
1797
9.9%
1664
7.5%
1589
7.2%
1349
7.1%
1986
4.6%
In 2005, the International Committee of Medical Journal Editors (ICMJE) began to require
trial registration as a condition of publication.
(data from clinicaltrials.gov, 08/07/2015)
Biomarkers in Clinical Trials
Integral, Integrated, or Exploratory
Integral: Required for trial to proceed
Patient inclusion/exclusion criteria
Assignment to specific trial arm
Continue/discontinue treatment
Integrated
Validation of biomarker to be used in future trials
Experimental design and statistical analysis pre-specified
Exploratory
Biomarker discovery/ mechanistic studies/ hypothesis generation
Which Biomarker Technology?
Provides Best and Economic Use and
Suitable with Regulatory Requirements
Film image
Digital imaging
Digital image analysis
Gene-by-gene
Gene panels
Genome sequencing
Western blot
ELISA
Mass Spectrometry
Microarray
H&E
RT-qPCR
IHC
RNA-seq
FISH
and...
Biomarkers in Clinical Trials
Use of Analytically Validated Assays
Accuracy and Precision
Sample obtainment and processing
Defined and obtainable standards
Qualified reagents
Analytical sensitivity
Analytical specificity
Stability
Example: Biomarkers in Clinical Trials
Use of Analytically Validated Assays
Validation of a multiplex assay for simultaneous quantification of
amyloid-β peptide species in human plasma with utility for
measurements in studies of Alzheimer's disease therapeutics
Lachno et al., J Alzheimers Dis. 2012;32(4):905-18
Abstract.The
The
aim
of this
study
was
to validate
the INNO-BIA
plasma(Aβ)
amyloid-β
(Aβ)forforms
assay for
Abstract.
aim
of this
study
was to
validate
the INNO-BIA
plasma amyloid-β
forms assay
quantification
of
Aβ1-40
and
Aβ1-42
according
to
regulatory
guidance
for
bioanalysis
and
demonstrate
its
fitness
for
clinical
trial
quantification of Aβ1-40 and Aβ1-42 according to regulatory guidance for bioanalysis and demonstrate
applications.
Validation
were evaluated
by repeated
testing were
of human
EDTA-plasma
pools. Intesting
6 separate
its fitness for
clinicalparameters
trial applications.
Validation
parameters
evaluated
by repeated
of
estimates,
intra-assay
coefficients
variation
(CV) forcoefficients
repeated testing
of 5 plasma
pools
human EDTA-plasma
pools.
In 6 separateofestimates,
intra-assay
of variation
(CV)
for
were≤9%
relative
(RE) varied
–35%
and
+22%. error
Inter-assay
(n = 36)
rangedand
from
5% to
repeated and
testing
of 5error
plasma
pools between
were≤9%
and
relative
(RE) variedCV
between
–35%
+22%.
Inter-assay
CV (nfrom
= 36)
ranged
from
5% to 17%linearity
and RE varied
from
–17% to +8%.
Dilutional
linearity
17%
and RE varied
–17%
to +8%.
Dilutional
was not
demonstrated
for either
analyte using
was
not
demonstrated
for either
analyte using
diluent
buffer,gave
but results
dilution
with20%
immuno-depleted
diluent
buffer,
but dilution with
immuno-depleted
plasma
by 1.67-fold
within
of target. Analyte
plasma by 1.67-fold gave results within 20% of target. Analyte stability was demonstrated in plasma at
stability was demonstrated in plasma at 2–8◦C for up to 6 h. Stability during frozen storage up to
2–8◦C
for and
up to
6 h. Stability
during
frozen
storage
todemonstrated
12 months and
through
3 freeze-thaw
cycles
12 months
through
3 freeze-thaw
cycles
at ≤–70◦C
wasup
also
in 5 of
6 individuals
but deteriorated
at ≤–70◦CNeither
was also
demonstrated
in 5 of 6interfered
individuals
deteriorated
thereafter.
Neither
thereafter.
semagacestat
nor LY2811376
with but
the assay
but solanezumab
at 500
mg/L reduced
semagacestat
nor LY2811376
interfered
with
the assay
butvolunteer
solanezumab
500
mg/L reduced
recovery of Aβ1-42
by 53%. Specimens
from
a Phase
I human
study ofatthe
β-secretase
inhibitorrecovery
of
Aβ1-42were
by 53%.
from
Phase up
I human
volunteer
study
of the
β-secretase
inhibitor
LY2811376
testedSpecimens
at baseline and
at a
intervals
to 12 h after
single oral
doses,
demonstrating
a clear
treatment
LY2811376
were
tested
at
baseline
and
at
intervals
up
to
12
h
after
single
oral
doses,
demonstrating
a
effect. During 1,041 clinical assay runs from semagacestat studies over 10 months, the CV for plasma quality
clear treatment effect. During 1,041 clinical assay runs from semagacestat studies over 10 months, the
control pools at three levels were≤15% and RE were <10%. In conclusion, the INNO-BIA plasma assay was
CV for plasma quality control pools at three levels were≤15% and RE were <10%. In conclusion, the
successfully validated and qualified for use in clinical research.
INNO-BIA plasma assay was successfully validated and qualified for use in clinical research.
Example: Integral Biomarkers in
Oncology Clinical Trials
BRAF V600E mutation in melanoma
Vemurafinib and Dabrafenib
Example: Integral Biomarkers in Oncology
Clinical Trials
Vemurafenib
Phase 1 - NCT00405587, Solid Tumors
Paired melanoma biopsies must have a V600E+ BRAF mutation
Phase 2 - NCT00949702, Melanoma
BRAF V600E positive mutation (by Roche CoDx BRAF mutation
assay)
Phase 3 - NCT01006980, Melanoma
positive for BRAF V600E mutation
Phase 4 - NCT01307397: Melanoma
BRAF V600 mutation determined by Cobas 4800 BRAF Mutation
Test
Dabrafenib
Phase 1 - NCT01262963, Solid Tumors
BRAF mutation-positive tumor (V600 E/K mutation) as
determined via relevant genetic testing
Phase 2 - NCT01153763, Melanoma
BRAF mutation-positive (V600 E/K) as determined via central
testing with a BRAF mutation assay
Phase 2 -NCT01336634, Lung Cancer.
BRAF V600E mutation confirmed in a CLIA-certified laboratory
(or equivalent)
Phase 3 - NCT01584648, Melanoma
BRAF V600E/K mutation-positive using the bioMerieux (bMx)
investigational use only (IUO) THxID BRAF Assay (IDE:
G120011).
A Few Additional Questions
If a biomarker result is required for use of a drug and
If biomarker positive patients respond to a drug, and
If biomarker negative patients are harmed by a drug
What is the consequence of a false positive test ? Of a false negative?
Example: Integral and Integrated Biomarkers in
Immuno-oncology Clinical Trials
PD-1 Antibodies in Oncology
Pembrolizumab and Nivolumab
Example: Integral and Integrated Biomarkers in
Immuno-oncology Clinical Trials
Pembrolizumab in lung cancer*
Biomarker
Response
*from Garon et al., Pembrolizumab for the treatment of non-small-cell lung cancer
N Engl J Med. 2015 May 21;372(21):2018-28.
Example: Integral and Integrated Biomarkers in
Immuno-oncology Clinical Trials
Nivolumab in melanoma*
Biomarker / Response
"In the subgroup with positive PD-L1 status,
the objective response rate was 52.7%
(95% CI, 40.8 to 64.3) in the nivolumab group"
"In the subgroup with negative or indeterminate PD-L1 status,
the objective response rate was 33.1%
(95% CI, 25.2 to 41.7) in the nivolumab group"
*from Robert et. al., Nivolumab in Previously Untreated Melanoma without BRAF Mutation
N Engl J Med. 2015 Jan 22;372(4):320-30
Immuno-oncology
PD-1 Antibodies
Questions for consideration:
If 40-50% of biomarker positive patients respond to a drug, and
If 10-20% of biomarker negative patients respond to a drug,
How would this test be useful in future clinical trials?
In clinical practice?
What is the consequence of a false positive/negative test ?
Example: Alzheimer's Disease
Integral and Integrated Biomarkers in
Clinical Trials
Biomarkers in Alzheimer's Disease
Bapineuzumab
Phase 1 - NCT00397891
Total plasma amyloid-beta (x-40) was determined
using a validated ELISA method
Phase 3 - NCT00575055
Bapineuzumab in Patients With Mild to Moderate
Alzheimer's Disease (ApoE4 Carrier)
Phase 3 - NCT00574132
Bapineuzumab in Patients With Mild to Moderate
Alzheimer's Disease (ApoE4 Non-Carrier)
Solanezumab
Phase 3 - NCT00905372: Progression of Alzheimer's Disease
Change from baseline to endpoint in plasma A Beta
Phase 3 - NCT00904683: Progression of Alzheimer's Disease
Change from Baseline to Week 80 in Plasma Amyloid Beta Levels
Importance of Biomarkers in Clinical Trials and Precision Medicine
Summary
Focus on Biomarker Utility
•
•
•
•
•
Diagnostic, Prognostic, Predictive, and/or Companion
Drug Efficacy: On Target, Clinical Response
Drug Side Effects/Toxicity
Patient Stratification
Integral, Integrated, or Exploratory
Some Questions in the Use of Biomarkers in Clinical Trials
1. At what stage of your clinical trial would you use a biomarker?
2. Would you use a non-validated biomarker in a clinical trial?
3. Would you not use a validated biomarker in a clinical trial?
4. If a high percentage of biomarker positive patients respond to a drug, and
a low percentage of biomarker negative patients respond to a drug,
How would this test be useful in clinical trials? In clinical practice?
5. What is the consequence of a false positive test ? Of a false negative?
Importance of Biomarkers in Clinical
Trials and Precision Medicine
Bringing Biomarkers to Clinical Practice
Jeffrey Shuster, PhD
jshuster@biomarkerfactory.com
Oracle Health Sciences
Strategic Vision for Precision
Medicine
James Streeter
Global Vice President Life Sciences Strategy
October 16th, 2015
@OracleHealthSci
#PrecisionMedicine
Copyright © 2015, Oracle and/or its affiliates. All rights reserved. |
Safe Harbor Statement
The following is intended to outline our general product direction. It is intended for
information purposes only, and may not be incorporated into any contract. It is not a
commitment to deliver any material, code, or functionality, and should not be relied upon
in making purchasing decisions. The development, release, and timing of any features or
functionality described for Oracle’s products remains at the sole discretion of Oracle.
Copyright © 2015, Oracle and/or its affiliates. All rights reserved. |
40
Oracle Health Sciences
Strategic Vision for Precision
Medicine
James Streeter
Global Vice President Life Sciences Strategy
October 16th, 2015
@OracleHealthSci
#PrecisionMedicine
Copyright © 2015, Oracle and/or its affiliates. All rights reserved. |
Safe Harbor Statement
The following is intended to outline our general product direction. It is intended for
information purposes only, and may not be incorporated into any contract. It is not a
commitment to deliver any material, code, or functionality, and should not be relied upon
in making purchasing decisions. The development, release, and timing of any features or
functionality described for Oracle’s products remains at the sole discretion of Oracle.
Copyright © 2015, Oracle and/or its affiliates. All rights reserved. |
42
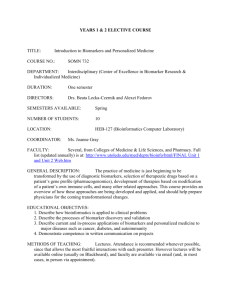
Industry Trends
Significant reduction in cost of
Increase in real world data
Cost
Will you use secondary
health data within the next
2 years?
70%
61%
Provider Pharma
Aggregation and analysis of Big Data
54%
Payer
Time
More than half of clinical trials already
have a molecular biomarker component
Patient stratification to identify population
subsets most likely to respond to a therapy
are
enhancing R&D collaboration
Copyright © 2015, Oracle and/or its affiliates. All rights reserved. |
Results
Formulated To
Accelerated Drug Discovery Through Biomarkers
Imatinib (Gleevec)
First in class targeted cancer therapeutic
Targets the BCR-ABL protein only
occurring in Chronic Myelogenous
Leukemia (CML)
Now considered standard of care for
Myelogenous Leukemia (CML)
Crizotinib (Xalkori)
Ivacaftor (Kalydeco)
Targets ALK protein, mutated in 7% of
lung cancers
Targets CFTR G551D mutation, present in
5% of cystic fibrosis patients
FDA approved from a trial of only 255
patients with the biomarker
Phase-III trial approval based on 161
subjects (Placebo 78; Ivacaftor 83)
Indication expanded to Gastrointestinal 3 years from biomarker mutation
Stromal Tumors (GIST) with KIT mutations discovery to approval
10.5% mean absolute improvement in
lung function
Copyright © 2015, Oracle and/or its affiliates. All rights reserved. |
Biomarker Uses in Drug Development
Discover
Develop
Deliver
Copyright © 2015, Oracle and/or its affiliates. All rights reserved. |
Requirements for Incorporating Molecular Analytics
a
Systematic way to manage genomic
data generated in a clinical trial
Integrates with EDC
Individual
Clinical Trial
Genomic profile
and analysis reporting
Single study and cross-study
analysis of biomarkers
Integrates with well-established public
domain data for joint
analysis with your own data
Copyright © 2015, Oracle and/or its affiliates. All rights reserved. |
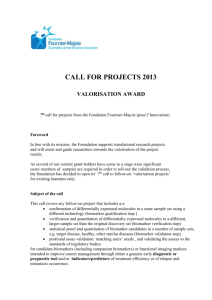
Oracle Products enabling Precision Medicine
Specimen
Doctor / Nurse
Clinical Data
InForm AMA
(Advance Molecular Analysis)
Genomic profiling
Molecular data analysis for
statisticians
FDA submission
Molecular
measurements
Enrolled
Patient
InForm/DMW
(Study Data)
IRT
Laboratory
(Enrollment Decisions)
Cohort
Explorer
(Data
Analysis)
Data Warehouse
Purchased or Public Domain
Data
(Data Models)
Big Data
(Prescription, Institutional, Government, etc.)
Copyright © 2015, Oracle and/or its affiliates. All rights reserved. |
Case Studies from Leading Molecular Data Initiatives
• To power Center for Individualized Medicine (CIM)
• Translational Research & Clinical use of 100k genomes
• $100M personalized medicine effort
• UPMC strategy – Science Driven, Patient-centric Care
• To power Moon Shots program
• To change 8 cancer types from terminal to chronic diseases
• To support Total Cancer Care program
• 19 hospitals, 10 states, 90k cancer patients
Copyright © 2015, Oracle and/or its affiliates. All rights reserved. |
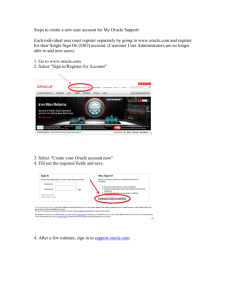
MD Anderson
CASE STUDY
Background / Needs
Moon Shots initiative to cure 6
cancers in 5 years
Single platform for clinical and
genomic data aggregation and
analysis
Scalability to address data growth
Results With Oracle
In less than 6 months, deployed a
reporting environment that contains in
excess of 1 million patients many
thousands with genomic tests
Reduced time to run complex cohort
identification queries from weeks to
minutes in self service mode
One source of truth for all data
Copyright © 2015, Oracle and/or its affiliates. All rights reserved. |
Strategic Vision for Precision Medicine
A world wide Genomic/Biomarker data warehouse
Patient consent and biomarker collection is standard of care and industry shared
Increase tools and data linkage to increase the precision
Post linked and processed data is also warehoused and openly available
Patients provides additional life long device data
Is standard for Drug Discovery and Clinical Trials and Submission
Copyright © 2015, Oracle and/or its affiliates. All rights reserved. |
healthsciences_ww_grp@oracle.com
+1.800.633.0643
www.oracle.com/healthsciences
Copyright © 2015, Oracle and/or its affiliates. All rights reserved. |
Copyright © 2015, Oracle and/or its affiliates. All rights reserved. |
The Present and Future Role of
Biomarkers in Clinical Development
A Partnership Journey towards Precision Medicine
Presented by
Sponsored by
Copyright © 2015, Oracle and/or its affiliates. All rights reserved. |