Wittmers_Ventilation_10.21.09
advertisement

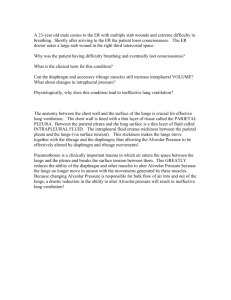
Ventilation – 10. 21.09 Wittmers – Resp 1 S. Eisenschenk Abbreviation: RQ = CO2 eliminated / O2 consumed Muscles of Respiration: Vectors: chest work vector and lung vectors are equal and opposite in direction during initial tidal vol. Chest work vector inverts when musc stop contracting and elastic recoil starts to pull it back in. Inspiration: active Diaphragm: innervated by phrenic (C3,4,5) & is most impt muscle for inspiration. -contract to gen neg P grad, inc axial length & transverse diameter (abdl contents down & forward rib ribs upward & outward.) -paralyzed: moves up instead of down w/inspiration Extl intercostals contract – move ribs up & out, innervated by intercostal nerves from that same spinal level, little consequence if paralyzed. Used during exercise & resp distress. (anat mnemonic hands in front pocket cuz fibers slope down and forward) Accessory musc of breathing: scalene (rib 1 &2), Sternocleidomastoids (sternum), alae nasi (flare nostrils) -little affect on quiet breathing, help during exercise Expiration: passive (Muscles used during exercise or inc airway R bc of disease, ie. Asthma) -potential energy stored in elastic elements of the resp musc passive recoil to resting position -Can contract abs in forced exhalation inc intra-abdominal P push diaphragm up & air out of lungs. Internal intercostals can also be contractedribs downward & inward. Ventilation Overview: avg vent data (L below, know values) VD=VT x (PACO2 – PECO2)/PACO2 PACO2=PCO2 of alveolar gas (mmHg)=PCO2 of arterial blood. PECO2=PCO2 of expired air (mmHg) Basically PDS, is TV x a fraction (represents dilution of alveolar P CO2 by dead-space air, which does not participate in gas-exchange & does not therefore contribute CO2 to expired air. Ventilation terms: Tidal Vol (TV): amt inhal/ex w/ea norm breath Vital capacity: amt exhaled w/max inspiration & expiration. Residual Vol: amt remaining in lungs after max exhalation (cannot be measd by spirometry) Func Residual Capacity: amt left in lung after norm expiration(TV) (cannot be measd by spirometry) Total (Minute) ventilation: total vol each lung receives in 1 min = TV x Resp freq Alveolar Vent: Total vent – anat dead space = amt that reaches alveoli/min =(VT – VD) x resp freq Anat dead space: vol of conducting airways (~150mL) Phys dead space: Fxnal unit, vol of lungs that does not participate in gas exchange. Approx = ADS in normal lungs, but may be greater in diseased lungs w/ vent/perf (V/Q) defects. that doesn’t elim/produce CO2 (see eqn to left). Know the concept, not the calculations Know the model, not the equations. We get an equation sheet for the exam. Ventilation – 10. 21.09 Wittmers – Resp 2 S. Eisenschenk Measuring Ventilation: -Spirometer: Tidal vol & vital capacity -expire bell up pen down on chart -Gas dilution technique: Func residual capacity, total lung capacity, and residual volume -set-up: spirometer + helium of known conc (insol in bld). -assumption: helium will not get out and will distribute evenly -Mass balancing relationship: C1 x V1 = C2(V1+V2) where C1, V1, C2 related to helium, and V2 is FRC or RV -Use V2 =V1 (C1-C2)/C2 to solve for FRC & RV. -The biggest error you can get is not getting good equil between all the parts of the lung. -Nitrogen Washout Technique: FRC, total lung capacity, and residual vol -set up: Nitrogen meter, expired gas collector, and 100% oxygen -assumption: all the N2 collected in the bag comes from the FRC -there is a fixed conc of N2 in the lungs and it dec with each breath, chart this to get FRC -FRC x Cx = VB x CB, solve for FRC. -Body Plethysmograph: FRC, total lung capacity, RV -set up: person in box, control P & V. -Errors: system doesn’t distinguish if gas pockets are connected, so will measure GI gas too -ask to have lungs at FRC then inhale harder w/mouth piece in that measures mouth pressure thorax expands compresses air in box -Boyle’s law states that P & V are constant at fixed temp, so we can solve for FRC (V2) -Conditions in Box: Conditions in Lung: P3V2 P4 (V2 V) P3 & V2 conditions before inspiration P4 & (V2 V) conditions after inspiration Relationship between thorax and lungs: -lungs lined by parietal and visceral pleura (hand in balloon) -interpleural space has a few mL of fluid that allow the pleura to stick together & slide -keeps lungs connected to thorax wall actions (when wall expands, so do the lungs) -break by leaking air into interpleural space -At FRC, the lungs have tendency to recoil inwards; the chest wall a tendency to recoil outwards. If lungs were removed from the thorax, they would be almost airless & the thorax would expand. Static examples, no flow Elastic elements are loaded w/pot energy during inspiration, passive recoil in expiration. Patm = Palv = 0, Pip = -7mmHg The neg transpulmonary P dec even more cuz of greater force vectors. Lung vol incd by TV. Patm = Palv = 0 – no gas exchange -Neg intrapleural P cuz lungs pull in and thorax out. Pip = -4 mmHg Lung vol returns to FRC. Know the concept, not the calculations Know the model, not the equations. We get an equation sheet for the exam. Ventilation – 10. 21.09 Wittmers – Resp 3 S. Eisenschenk Pressures, Flows, and Volumes During Breathing. (right) At Rest: FRC – elastic recoil of lungs = elastic recoil of chest wall in opp direction. -alveolar P = 0 = Patm cuz no airflow = no pressure drop in system (ZERO) -intrapleural P – start at -5cmH20 cuz of elastic recoil in lung (REST NEGATIVE) -Flow is zero. Inspiration: musc contractionthoracic VolPalvair flow -alveolar P falls (bc of decd thorax vol), est driving pressure (NEGATIVE) -extent of fall depends on flow rate & resistance of airways -Norm = Palv fall to -1cmH20, disease states can cause greater drops -Middle of inspiration flow is max. -Pip falls during inspiration (-8cmH20)cuz: (MORE NEGATIVE) 1. as lung expands , the elastic recoil inc (alone this ABC above) 2. further fall in Pip is assoc w/hatched area so real course is AB’C (left image) -At the end of inspiration the flow is zero. Expiration: Palv becomes greater than atm P. (POSITIVE) Pip is less neg (resting value) than it would be in the absence of airway R because Palv is positive. (REST NEGATIVE) -Middle expiration flow = max, at end flow = zero. Force expiration the Pip goes above zero. (POSITIVE) In COPD, “purse lips” to prevent airway collapse that may occur w/ forced expiration. Note: Alveolar P & flow curves are identical (bc recoil P drives flow). PipSolid line= dynamic - flow occurring (stretch (elastic)P + work against P), dotted line=static (only stretch P (elastic). Restrictive dx of muscles, rubs, bones will be seen in dynamic line, obstructive dx that affects diameters of airways will be see in dotted line. Another way of saying it is that solid line demonstrates F reqd to overcome compliance of lungs & airway R, while the hatched line demonstrates only F needed to overcome compliance o flungs. Total (Minute) Ventilation = total vol leaving lung/min -Total vent measured by collecting expired gas -VT=TV Alveolar vent = vol of fresh gas entering alveoli/min (differs from TV) -rep amt of fresh inspired air available for gas exchange -regulated -harder to measure – -calc total vent and subtract anat dead space vent -physiological measurement of alveolar vent. -all the CO2 produced comes from alveolar gas, so…(below) Alveolar vent can be inc by: -inc tidal vol (best cuz red portion in anat dead space) -inc resp frequency. VCO2 FACO2 x VA where : FACO2 is the fractional content of CO in the alveolar gas proportional to P rearranging the above to get VA ACO2 2 , VCO2 K PACO2 * In normal pt Anat dead space = Phys dead space. Named because measured by dif means *Pt with lung disease may have larger phys dead space due to inequity of bld flow & vent in lung Anatomical dead space: conducting airways -estimate anat dead space: weight mL (150 lbs 150mL) -affected by size and posture of subject -measure anat dead space w/Fowler’s Method (anat method) -set up: following single breath 100% O2 the subject breathes through valve box and N2 is measured at mouth -N2 rises as the dead space is washed out by alveolar gas. -plateau = pure alveolar gas (flat in norm, steep in pt w/lung disease) Know the concept, not the calculations Know the model, not the equations. We get an equation sheet for the exam. Ventilation – 10. 21.09 Wittmers – Resp 4 S. Eisenschenk Physiological Dead Space: Vol of lung that doesn’t eliminate CO2 -measured by Bohr’s Method (functional measure) -All expired CO2 comes from alveoli, not dead space so based on V & P’s you get a ratio of VD & VT VD VT FACO2 - FECO2 FACO2 (5) Bohr' s equation the normal ratio of VD & VT is 0.2 -0.35 at rest. F P and PA Pa where P a is the arterial partial pressure VD P - PECO2 aCO2 (5) VT PaCO2 -Since the PCO2 of alveolar gas & art bld are almost identical in norm individuals you can rearrange for the second equation. Regional Dif in Ventilation: -due to gravity, base (lower P) vent better than apex (higher P) if standing and apical=basal if supine -measured using radioactive xenon gas, recorded as it penetrates chest wall ID region w/greatest conc Study Questions: What do these abbreviations mean? 1. 2. 3. 4. Define the following terms and identify what tests are best used to measure them: tidal volume, vital capacity, functional residual volume, and residual volume 5. Calculate Total Ventilation and Alveolar Ventilation: Where: f = 12 breaths/min VT = 500 ml/breath VDS = 150 ml 6. Flower’s Method measure ______________ while Bohr’s Method Measures ________________. A. Anatomical Dead Space B. Physiological Dead Space 7. Region differences in ventilation in a normal person depends primarily upon ____________. A. gas conc B. gravity C. perfusion D. lung disease Know the concept, not the calculations Know the model, not the equations. We get an equation sheet for the exam. Ventilation – 10. 21.09 Wittmers – Resp 5 S. Eisenschenk Answers: 1. The partial pressure of oxygen in the Alveolar gas. 2. The amount of carbon dioxide produced 3. The amt of C02 produced = alveolar ventilation x Fractional alveolar conc of carbon dioxide 4. Ventilation terms: Tidal Vol: amt inhaled w/ea norm breath Vital capacity: amt exhaled w/max inspiration & expiration. Residual Vol: amt remaining in lungs after max exhalation Func Residual Capacity: amt left in lung after norm expiration Tidal vol & vital capacity measured by simple spirometer Total lung capacity, Func Residual Capacity, and Residual Volume by gas dilution or plethysmograph 5. Minute Ventilation: VE = 12 breaths/min x 500 ml/breath VE = 6000 ml/min = 6 L/min Alveolar Vent: VA = 12 bre/min ( 500 ml/bre -150 ml/bre) VA = 4200 ml/min = 4.2 L/min 6. A, B 7. B Know the concept, not the calculations Know the model, not the equations. We get an equation sheet for the exam.