Head and Face Injuries
advertisement

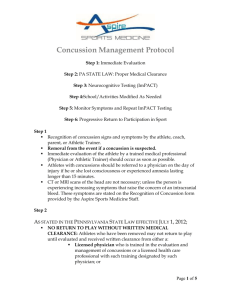
Injuries to the Head, Neck & Spine Cerebral Conditions Impact or injuries causes bleeding within the brain called HEMATOMAS Artery damaged: quick decline in mental status and functioning of the brain (10 – 20 minutes) Vein damaged: slower onset (24 to 72 hours), slower bleeding and swelling Both are life-threatening!!!!!! Concussions Definition = the temporary impairment of brain function caused by impact to the head, or rotational force Usually caused by a direct hit to the head, plus the injury to the opposite side of the brain where the brain bounces off of the skull. The more concussions you sustain, the more severe they become, and the easier it is to get one! Concussions Football Softball Basketball Mechanisms Direct impact causes two conditions 1. deformation 2. acceleration Direct blow can cause fracture at the site of impact Direct blow can cause fracture at site away from area of impact Signs and Symptoms Dizziness Headache Excessive Drowsiness Unable to focus or concentrate »Irritable and Confused » Convulsions * Nystagmus *Visual problems - Bleeding from nose or ears -Tinnitus (ringing in ears) ~Paralysis ~Weakness in limbs or face ∞Memory problems ∞Balance problems Nausea Vomiting Concussions Treatment: Careful removal from play Thorough physical and neurological examination Refer to physician for follow-up examination Assessment of Concussions Concussions Assessment: Neuropsychological Testing If possible, preseason testing on a computerized system (ImPACT). If a concussion occurs, retest injured athlete following recommended protocols. Thorough evaluation of athlete: (Sport Concussion Assessment Tool (SCAT 2) is a tool that can be used to evaluate a concussed athlete. Physical Examination – evaluation of athletes physical symptoms as listed previously. Assessment of Concussions Concussions Assessment Cognitive testing Immediate memory testing What month is it? What time is it?, etc. Concentration Months of year backward 100-7, continue backward Delayed Recall – have athlete remember words, repeat at later time Assessment of Concussions Concussions Assessment Balance/Coordination testing Balance Error Scoring System (BESS) Romberg Test Finger to Nose Common Injuries – Head/Neck Return to Play Guidelines: Depends on the level of play of the athlete involved. Currently, the NCAA, UHSAA, and a new Utah State law regarding youth sports (HB 204) will dictate a specific plan for concussion management and return to play guidelines. It will include some variation of the following : Progression through Return-To-Play stages on a case by case basis with final clearance by an approved, licensed health care professional: Common Injuries – Head/Neck Common Injuries – Head/Neck Second Impact Syndrome Rapid swelling of the brain from additional head trauma; life threatening Second impact could be minor Could be caused by blow to chest that accelerates head. Signs and Symptoms No initial loss of consciousness Rapid worsening leading to: LOC progressing to coma Dilated pupils Loss of eye movement Respiratory failure Treatment: Immediate transport to medical facility Prevention DO NOT LET THIS SITUATION OCCUR! Careful decision making regarding return to play following initial head trauma Common Injuries – Head/Neck Post-Concussion Syndrome Persistent symptoms following concussion May begin immediately following injury and may last for weeks to months Persistent headache Impaired memory Lack of concentration Anxiety Irritability Fatigue Depression Continued visual disturbances Treatment – No clear guidelines Treat symptoms to greatest extent possible Return athlete to play when all signs and symptoms have fully resolved ESPN Concussions OTL: College Football Concussions Scalp Injuries Highly vascularized; bleeds freely Laceration Control bleeding Prevent contamination Assess for skull fracture (fx) Management: If no fx, cleanse, cover, and refer Abrasions and contusions Cleanse; ice and pressure 24 hours: no improvement – refer Skull Fracture Types Linear Comminuted Depressed Basilar Skull Fracture (cont.) Potential for varying signs and symptoms Visible deformity–do not be misled by a “goose egg”; a fracture may be under the site Deep laceration or severe bruise to scalp Palpable depression or crepitus Unequal pupils Raccoon eyes or Battle’s sign Skull Fracture (cont.) Bleeding or CSF from nose and/or ear Battle Sign Raccoon Eye’s “Halo” Sign Loss of smell Loss of sight or major vision disturbances Unconsciousness 2 minutes after direct trauma to the head Management: activation of EMS Facial Conditions Facial soft tissue conditions Contusions, abrasions, and lacerations are managed the same as elsewhere on the body Complicated injuries—immediate physician referral Nasal Conditions Epistaxis (nose bleed) Anterior – bleeding from anterior septum Posterior – bleeding from lateral wall Management: ice, mild pressure, slight forward head tilt; nasal plug; 5 minutes – physician referral Deviated septum S&S Consistent difference in airflow between the 2 sides of the nose when one nostril is blocked Confirm using otoscope Management: physician referral Nasal Conditions (cont.) Fractures Most common: lateral displacement Range of severity varies S&S Asymmetry – especially with lateral force Epistaxis Crepitus Management: control bleeding; refer Ear Conditions Cauliflower ear (auricular hematoma) Repeated trauma Untreated – forms a fibrosis Management: ice; possible aspiration by physician Key is prevention Eye Conditions Preorbital ecchymosis (black eye) Assessment Management: ice, referral to ophthalmologist Foreign bodies S&S: intense pain, tearing Management Not embedded: removal, inspection Embedded: do not touch, activate EMS Eye Conditions (cont.) Orbital “blowout” fracture Impact from a blunt object, usually larger than the eye orbit S&S: Diplopia Numbness below eye Lack of eye movement Recessed downward displacement of globe Management: ice; immediate referral to physician Cervical Spine Fracture S&S Pain Numbness Tingling Management Spinal immobilization Refer to a physician Brachial Plexus 31 pairs of spinal nerves “Stinger” Brachial C5-T1 Numbness Loss of function Management Remove from play Allow RTP once symptoms resolve Guess the Injury! Ouch…that hurts! DIRECTIONS: For each of the following slides, try to identify the type of injury that has occurred. Write your answer on your paper. #1 #2 #3 #4 #5 #6 #7 #8 #9 #10 Answers 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. Concussion Scalp Laceration Battle Sign Deviated Septum Foreign object Preorbital Ecchymosis (Black Eye) Epistaxis (nose bleed) Cauliflower Ear Orbital Fracture Brachial Plexues