The Importance of Prioritizing Cancer Prevention at Major Academic
advertisement

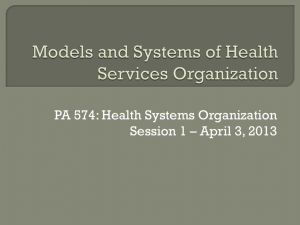
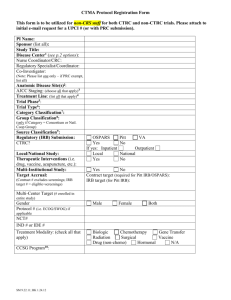
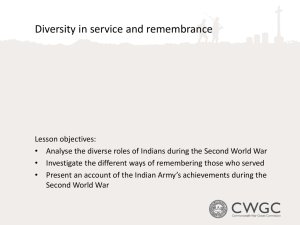
UNIVERSITY OF PITTSBURGH CANCER INSTITUTE A National Cancer Institute (NCI)-designated Comprehensive Cancer Center The Importance of Prioritizing Cancer Prevention at Major Academic Cancer Centers Ronald B. Herberman, MD University of Pittsburgh Cancer Institute http://www.upmccancercenters.com March 2009 Current Research Paradigm at Most Academic Cancer Centers Main focus on – – – Developing & improving cancer therapies Carcinogenesis Early detection Little attention on cancer prevention or risk reduction Traditional Cancer Prevention Activities at Academic Cancer Centers (1) Research on healthy lifestyles – – Strategies to reduce unhealthy behaviors Smoking prevention; exercise; better nutrition; calorie reduction Molecular carcinogenesis research (geneenvironment interactions) – – Identification of genes contributing to risk Identification of environmental risk factors Traditional Cancer Prevention Activities at Academic Cancer Centers (2) Screening of populations for genetic risk factors & genetic counseling of individuals with genetic risk Research to develop new, more sensitive and specific biomarkers for early detection of cancer Screening of populations for early detection of certain cancers Prevention Provides Greatest Impact on Wide Variety of Diseases Greatest public health advance of 19th and 20th century was prevention of infectious diseases Greatest impact on heart disease was the wide implementation of statins to reduce risk Key impact of seat belts and helmets on reduction of traumatic injuries Preventive and risk-reducing strategies also will most likely have the greatest impact on reducing burden of cancer Heart disease provides an excellent example of successful prevention Over the last 30 years heart disease has decreased significantly. 50% of this decrease is attributed to drug prevention strategies. Pharmacologic intervention using cholesterol and blood pressure lowering drugs has been used to prevent atherogenesis. UPCI and UPMC Cancer Centers: Integrates Across The Cancer Continuum To Improve Patient Care [Source: The Pennsylvania Comprehensive Cancer Control Plan, December, 2003] Epidemiology Describes Four Levels For Cancer Prevention Primordial or Societal Prevention – Avoids the emergence and establishment of social, economic, and cultural patterns of living that are known to contribute to elevated risk of disease Primary Prevention – Controlling causes and risk factors Condoms, needle exchange or vaccine to prevent spread of HIV, HBV or HPV Secondary Prevention (from onset of disease to normal diagnosis) – Develop safe accurate methods of detection (at early curable stage) and development of preventive drugs, vaccines Tertiary Prevention – Reducing ongoing morbidity or mortality once cancer is diagnosed • Monitoring for early detection of second primary cancers Modified from Basic Epidemiology, R. Beaglehole, et al, 1993 Inherited Gene Defects Do Not Explain All Cancer Risk Fewer than 1 in 10 cases of breast cancer arises in women born with genetic defects -National Cancer Institute Academic Cancer Centers Can Develop More Effective Cancer Prevention Strategies (1) Research on Environmental Risk Factors – – – Evaluation of geographic areas with probable exposures to identify risk factors and health impacts Basic research to establish links between exposures and cancer including mechanism of action Development of biomarkers to identify people at increased risk Research to develop strategies to reduce or eliminate risk factors from the environment Identification of effective ways to block carcinogenic effects of environmental carcinogens – – Discovery and development of radioprotective agents Discovery and development of free radical scavengers to prevent DNA damage and approaches to improve DNA repair Academic Cancer Centers Can Develop More Effective Cancer Prevention Strategies (2) Identify effective ways to change the social, economic, and cultural patterns of living that are known to contribute to elevated risk of disease Provide state-of-the-art, cancer center-based, interdisciplinary approaches to identify controllable or avoidable environmentally linked causes of cancer and strategies to reduce risk Develop and validate interventions that inform, educate and change individual and institutional behaviors associated with increased risk Academic Cancer Centers Can Develop More Effective Cancer Prevention Strategies (3) Development of Effective Interventions to Prevent Cancer – – – Discovery & development of chemopreventive agents for individuals at increased risk for cancer Nutraceutical research Discovery & development of preventive vaccines Development and validation of improved strategies for Early Detection – Develop improved and convenient biomarkers (e.g. blood or urine) for screening and early detection Cancer Prevention at UPCI •Center for Environmental Oncology •Biochemoprevention Program •Biomarkers of exposure, increased risk, and early stage cancers What is ‘Environmental Oncology?’ Clinical oncology detects and treats disease ‘Environmental Oncology’ seeks to identify causes of disease in order to predict and prevent cancer – – – Identifies, develops, and measures biomarkers of exposure, susceptibility Identifies windows of susceptibility Develops and implements interventions to reduce risk in people exposed and at high risk Center for Environmental Oncology (CEO) Started July, 2004 at the University of Pittsburgh Cancer Institute Focus on Environmental Risks, Exposures, Health Effects Research and Community Education – – – Provide a state-of-the-art, medical center-based, cross-disciplinary approach to identify controllable or avoidable environmentally linked causes of cancer Develop and promote key changes in environmental policies to reduce risk factors Create and validate interventions that inform, educate and change individual and institutional behaviors, or that have potential to reduce cancer in individuals at increased risk Four Divisions of the Center for Environmental Oncology Basic Research Outreach, Education, and Public Policy Molecular, Environmental, and Clinical Epidemiology Environmental Assessment and Control CEO Areas of Emphasis Basic Research – Molecular, Environmental and Clinical Epidemiology – – Behavioral modification Biochemoprevention Environmental Assessment, Monitoring, and Control – Perform community and clinical research to identify patterns and trends of disease tied to environmental exposures Preventive interventions based on epidemiologic evidence for individuals at increased risk – Provide scientific evidence on environmental carcinogens, geneenvronment interactions, & biomarkers of environmental carcinogenesis Develop institutional protocols for monitoring and control of pollutants for the hospital and the community Community and Professional Education and Public Policy – Communicate links between the environment and cancer and develop policies to reduce cancer risk for individuals and institutions Evidence Supporting Environmental Exposure as a Cause of Cancer Experimental Epidemiological Case control studies Cancer Incidence Trends Jobs With Increased Risk of Breast Cancer Solvent workers Chemists Nurses and Physicians Dentists Painters Hair Dressers Exposure Risk Assessment and Precaution Pediatric Head CT Scans-2008 Exposure – – – Pediatric CT Scans are tool of choice in ER ER Physicians are not aware of level of radiation exposure in CT Pediatric CT scans can be 200 to 6,000 chest x-ray equivalents Workshop held UPCI-March 26, 2008 with national experts White paper drafted outlining risks, benefits, and better options for ER treatment with reduced cancer risk with recommendations to reduce exposures Long-term Cell Phone Use and Brain Tumor Risk Suggestive but not Definitive Data Case-control study ((Hardell et al Int. J of Oncology. 28:509-518, 2006) – – Acoustic neuroma: OR=2.9 (CI 2.0-4.3; analogue cell phone), OR=1.5 (CI1.1-2.1; digital cell phone); OR=1.5-fold (CI 1.04-2.0, cordless phone) Acoustic neuroma > 15 years: OR=3.8 (CI 1.4-10; analogue cell phone) Review of 11 case-control published studies with > 10 years wireless cell phone use (Hardell et al. Occ Env Med. 64:626-632, 2007. – – – Increase in acoustic neuroma (4 studies statistically significant) Increase in glioma (all gave increased odds ratios, 4 statistically significant) Meta-analysis Meta-analysis (Hardell et al. Int J of Oncology, 32:1097-1103, 2008) – – 6 studies glioma: latency > 10 years, 4 studies ipsilateral OR=2.0 (CI 1.2-3.4) 4 studies acoustic neuroma: latency > 10 years, ipsilateral OR=2.4 (CI 1.15.3) Meta-analysis (Kan et al. J Neurooncol 86:71-78, 2008, UTAH study) – Acoustic neuroma (ipsilateral) OR=2.4 (CI 1.1- 5.3) Glioma (ipsilateral) ) OR 2.0 (CI 1.2-3.4) 5 case control studies with cell phone use > 10 years: brain tumor OR=1.25 (CI 1.01-1.54) INTERPHONE (2008 update) – Glioma, ipsilateral OR=1.39 (CI 1.01-1.92); Nordic study (Lahkola et al, 2007) Cell Phone Radiation is Absorbed More Deeply Into the Brains of Children Estimation of the absorption of electromagnetic radiation from a cell phone based on age (Frequency GSM 900 Mhz) (On the right, color scale showing the Specific Absorption Rate in W/kg) Gandhi, O.P.G. Lazzi, and C.M. Furse, Electromagnetic Absorption in the Human Head and Neck for Cell Telephones at 835 and 1900 MHz. IEEE Transactions on Microwave Theory and Techniques, 1996. 44(10): p. 1884-1897 Hypothesis: If the long term use cell phone studies are correct in pointing to increased risk for brain tumors, the incidence of brain tumors should be increasing, particularly in children and young adults SLER Registries for GLIOMAS age-specific incidence, 0-39 years of age 5 Incidence (per 100,000) 4 0-9 3 10-19 20-29 30-39 2 1 0 1975 1980 1985 1990 1995 Year of Diagnosis 2000 2005 Exposure Risk Assessment and Precaution 0n Cell Phones; Follow up July, 2008: Ronald Herberman, after consultation with UPCI and international experts including epidemiologists and neurosurgeons, issued e mail with precautions for safer use of cell phones, and calls for studies to more definitely determine cell phone risks Media learns about the precautionary e mail and news travels around the globe, mainly correct, but with some inaccuracies – Other countries issue precautions (France, India, Israel, Canada) October, 2008: Ronald Herberman asked to testify before Congress on the science behind cell phone risk, the rationale for his precautionary advisory, and the need for more studies October, 2008: analysis of age-specific brain tumor data shows increases in glioma rates especially for young adults-manuscript submitted for publication September, 2009: Planning in progress for an UPCI-led, Congressionally sponsored workshop on cell phones and potential risks for cancer Plans being developed to further assess ability of radiofrequency radiation to cause DNA damage, and determine underlying mechanism(s) Identification of Risks and Strategies for Reduction selected examples Pediatric CT Scans promoting awareness that CT radiation exposure for head scans in children can be 200 to 6000 chest x-ray equivalents – National workshop held at University of Pittsburgh, Spring 2008 and white paper with recommendations for emergency room use of CT scans being developed Cell phones and brain tumors – Review literature and bring attention to multiple reports linking long-term cell phone use with increased risk for glioma and acoustic neuroma – Dissemination of precautionary use memo to UPCI and UPMC Cancer Center faculty and staff – Provide testimony at congressional hearing calling for needed studies to determine safety of cell phones Passive smoking in Allegheny County-promoting smoking ban in public buildings including bars and restaurants – – – – – Senior leadership testimony to Allegheny County political leaders UPMC and University of Pittsburgh became smoke-free facilities in 2007 Allegheny County passed ban in 2007 on smoking in restaurants and bars that make a significant percentage of profit from food PA passed similar statewide ban in 2008 Fire retardants in bedding and computers-promote national and international awareness of the lack of need for chemical fire retardants and awareness of toxicities nationally and internationally – Blocked passage of requirement for fire retardants nationally and world-wide Biological Effects of Environmental Xenoestrogens • Assessment of the effect of growth of estrogen-dependent breast cancer cell line • Validation of an estrogen screening assays that show competition for receptor binding and cell growth effects Talal El-Hefnawy Estrogenic Pollutants Induce Breast Cancer Cell Proliferation 160 140 120 100 80 60 40 20 Coum 2000 Coum 400 Coum 80 BaP 2000 BaP 400 BaP 80 DDE 2000 DDE 400 DDE 80 BPA 2000 BPA 400 BPA 80 endo 2000 endo 400 endo 80 E400 E 80 0 control BrdU Value (absolute absorption) Estrogenic compounds induce MCF7 breast cancer cell proliferation Quantitative BrdU assay, dark spots indicate high DNA synthesis Talal El-Hefnawy Biochemoprevention Program University of Pittsburgh Cancer Institute Ongoing Preclinical Cancer Prevention Research (1) Cancer prevention by garlic-derived organosulfur compounds – – Cancer prevention by cruciferous vegetable-derived isothiocyanates – – – – – – Prostate cancer (Singh) Tobacco carcinogen-induced lung cancer (Singh) Prostate cancer (Singh, Dhir, Nelson) Breast cancer (Singh and Vogel) Pancreatic cancer (Srivastava) Head and neck cancer (Grandis and Singh) Bladder (Singh) Melanoma (Brown and Singh) Angioprevention – – Resveratrol (red wine) plus statins (Li) Isothiocyanates and organosulfides (Singh) Ongoing Preclinical Cancer Prevention Research (2) Prevention of colon cancer with NSAIDs (Zhang) Cancer prevention by traditional Ayurvedic remedies (Singh) Cancer prevention by vaccines or other immunologic approaches (Finn, Gorelik) Cancer prevention by combination of small molecules & biologics (Gorelik, Li) Inhibition of PC-3 Xenograft Growth by Garlic-derived Diallyl Trisulfide (DATS) A B 750 Control DATS 450 300 150 0 0 5 * 10* * * * * 15 20 25 29 600 * 450 300 Weight (g) Wet tumor weight (mg) Tumor volume (mm 3) 750 600 C Control DATS 26 23 150 0 Control DATS Days after tumor implantation 20 0 5 10 15 20 Days after tumor implanation DATS (5 μmol) was given orally three times/week *P < 0.05 by Student’s t-test. Shivendra Singh 25 Resveratrol is a chemoprevention agent derived from natural sources Natural sources: Grapes (50-100 g/g) Red wine (1-3 mg/L) Peanuts TCM Polygoum cuspidatum Phytoalexin Resveratrol Shivendra Singh Resveratrol prevents experimental cancer DMBA-induced skin cancer model. 0, 1, 5, 10, or 25 µmol of RSVL plus 5 µmol of TPA Copied from Jang et al, Science, 1997 Shivendra Singh Chemoprevention to Stop Progression of Premalignant or Stage 0 Lesions • UPCI Research Studies – – – – – NSABP Polyp Prevention Trial Evaluation of celecoxib as a breast cancer chemopreventive agent with intracellular biomarkers Serial evaluation of ductal epithelium NSABP STAR trial Muc1 vaccine for prevention of colon polyps Biomarkers Being Evaluated in Study of Celecoxib for Prevention of Breast Cancer • Changes in cytology • Changes in biological markers COX-2, • aromatase, and estradiol Changes in the fractional mutation index (defined as the number of mutated markers divided by the sum of all informative markers among 20 pre-selected genes) MUC1-Poly ICLC (HiltonolTM) Vaccine in Individuals with Advanced Colorectal Adenoma Robert Schoen & Olivera Finn Rationale • Chemoprevention of adenomas is an accepted focus – ASA, COX2, vitamins • Immunotherapy • Non toxic • Highly specific • Boost or improve native immune surveillance → prevent progression to malignant disease • Vaccine potentially more effective before tumor suppresses immune response Meta-analysis: Muc 1 Immunotherapy in CRC • 32 studies, 527 patients • Toxicity mild – flu like symptoms, injection site reactions • Humoral immune response 59%, cellular immunity – 44% • Clinical response 10-14% Nagorsen, Clin CA Res 2006;12:3064 Why Study Advanced Adenoma? • “Target” for CRC screening • Higher risk for subsequent cancer • Higher adenoma recurrence rate: followed with q3yr surveillance • Intact immune system • ↑ expression of Muc 1 • Prime candidate for vaccine administration Objectives Primary • Evaluate immune response to MUC1-Poly ICLC Secondary • To monitor MUC1 isotypes: IgG, IgM • To monitor adverse events • To evaluate correlation between anti MUC1 response and adenoma recurrence (not powered to this endpoint) Serum and Tissue-based Biomarker Discovery -- Needs • • • Comparative/differential proteomics and metabolomics – to identify and characterize protein patterns that distinguish exposed individuals from healthy controls, using biological specimens – to identify and characterize hormone or other metabolites that distinguish exposed individuals from healthy controls Comparative/differential genomics – to identify and characterize changes in DNA and nuclear DNA and protein methylation patterns that distinguish exposed individuals from healthy controls, using biological specimens Application: identification of biomarkers of exposure including: 1. Cellular signatures indicative of toxic exposures 2. Epigenetic changes linked to altered gene expression 3. Hormone metabolites and cancer risk Biomarker Discovery at UPCI • • • Establishment of tissue and serum banks with high quality specimens from healthy individuals and cancer patients Support for Bioinformatics both for tissue annotation and high complexity data analysis Development and support of integrated Cancer Biomarkers Core for Specimen Analysis • • • Platforms for genomic analysis including chip-based array technology and multiplex genotyping Platforms for high-throughput proteomic analysis Platforms for comprehensive metabolomics analysis SERUM vs. URINE IN OVARIAN CANCER SERUM 4 biomarkers SP=98% URINE 3 biomarkers SP=100% Anna Lokshin SN=90% SN=100% ROC curve for classification of endometrial cancer 1.0 A 0.8 0.6 0.4 5 BIOMARKERS AUC=0.98 0.2 PROLACTIN PROLACTIN 0.0 0.0 6 BOMARKERS AUC=0.98 0.2 0.4 0.6 AUC=0.94 AUC=0.94 0.8 1.0 SENSITIVITY SENSITIVITY 1.0 0.8 0.6 0.4 0.2 0.0 0.0 1-SPECIFICITY SENSITIVITY = 98% SPECIFICITY = 94% Prolactin, HE4, CA 72-4, MMP-3, and FasL Anna Lokshin 6 BIOM PROLA 0.2 0.4 1-SPECI Expected Outcomes As Academic Cancer Centers Focus on the 4 Levels of Cancer Prevention Rapid identification of environmental risk factors and approaches to minimize exposures Development of evidence-base to prioritize high impact cancer control strategy Improved strategies for early detection & biochemoprevention Establishment of regional and state-wide networks to facilitate rapid implementation of effective education and prevention-based interventions Identification of resources and more effective use through collaboration and cooperation will more effectively disseminate prevention strategies