Avoidable-death-2015_16-Hogan-slides-only-(2)
advertisement
")
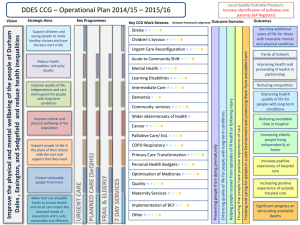
Is avoidable mortality a good measure of the quality of healthcare? Dr Helen Hogan Clinical Senior Lecturer in Public Health London School of Hygiene and Tropical Medicine Outline • What drives interest in avoidable mortality • Problems with use as a measure of hospital quality • Approaches to measurement and what we have learned • Local and national developments • The future Why it matters? Limitations of avoidable deaths a measure of quality Measuring avoidable death using population-level data • • • • • HSMR/ SHMI/ RAMI Coded adverse events linked to death Known avoidable harms linked to death Patient Safety Indicators Prospective surveillance systems Measuring avoidable deaths at patient level What have we learnt so far • Preventable Incidents Survival and Mortality studies (PRISM) 1 and 2 (co-applicants Nick Black, Frances Healy, Graham Neale, Richard Thomson, Charles Vincent, Ara Darzi) • Association between avoidable deaths (RCRR) and excess deaths (hospital-wide mortality ratios) PRISM 1 Study • 2010/2011 • Aims: – estimate proportion of avoidable hospital deaths – identify ‘problems in care’ and contributory factors – estimate years of life lost • Method: – RCRR (1000 adult deaths across 10 acute Trusts in England) – Trained, retired doctors with standard form Findings • 75% good or excellent care • 11.3% ‘problem in care’ contributing to death • 5.2% deaths probably avoidable – range 3% - 8% (low variation between Trusts) – estimate 11,859 avoidable adult deaths/year in England NHS • Life expectancy of avoidable death patients – 60% patients had life expectancy less than 12 months • Inter-rater reliability Kappa 0.49 Problems in care identified in cases of preventable death Stage of patient Types of problem identified journey Preadmission Poor monitoring of warfarin Delays in admission for hospital procedure Contraindicated drug prescribed in outpatients Early in admission Failure to diagnose Delayed diagnosis Wrong diagnosis Failure to identify the severity of underlying conditions and risks posed by the chosen therapeutic approach Failure to optimise preoperative state Care during a procedure Procedure conducted in inappropriate environment Technical error Post procedure Inadequate monitoring (fluid balance, infection) Poor assessment Ward care Inadequate monitoring of overall condition, fluid balance, laboratory tests, side effects of medications (especially warfarin), pressure areas and infection Unsafe mobilisation leading to serious falls Hospital acquired infection Prescription of contraindicated drug Delay in undertaking required procedure PRISM 2 Study • Based on recommendations emerging from the Keogh review • Relationship between ‘excess mortality rates’ and actual ‘avoidable deaths’ • Findings to support introduction of a new national outcome framework “hospital deaths attributable to problems in care” and systematic approach to local mortality review PRISM 2 Study • 2014/2015 • Extend PRISM 1 to further 24 Trusts • Similar method to permit analyses of combined data from both studies (n=3,400 records) • Random sample of Trusts across 4 strata of HSMR • Trained reviewers (70% current consultants, 30% retired) • Linear regression to determine the percentage increase in avoidable death proportion for a 10 point increase in HSMR/SHMI Findings • 78% good or excellent care • 9.4% ‘problem in care’ contributing to death • 3.0% deaths probably avoidable – range 0% - 9% (low variation between Trusts persists) • Inter-rater reliability Kappa 0.35 Combined Findings • 3.6% probably avoidable • no statistical significant association between hospital SMRs and the proportion of avoidable deaths • Local Mortality Review The future – Standardised self-assessment will ensure robust process • • • • National approach to training and materials Electronic database/ NRLS All deaths screened, high risk cases selected for in-depth Multidisciplinary process • National Tracking of Outcome Indicator • Random sample of NHS deaths • National panel of trained reviewers (multi-disciplinary) • Multiple reviewers per record • Timetable: Invitation to tender via HQIP – http://hqip.org.uk/tenders/rcrr%20tender%202015/ The future • Direct comparison of Trusts based on avoidable X deaths • Develop notional avoidable death proportions ?? • Use a coherent set of indicators known to be associated with quality e.g. hospital acquired infections and measure as robustly as possible • Develop indicators that reflect integrated care/ quality of care across health systems Thank you helen.hogan@lshtm.ac.uk