Frailty pathway - West Lothian
advertisement

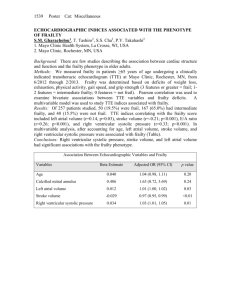
Frailty pathway Latana A. Munang Consultant Physician and Geriatrician St John’s Hospital Outline The status quo Frailty Comprehensive Geriatric Assessment The Frailty Pathway Summary & Discussion Projected population change West Lothian General Register Office for Scotland MEDICAL ADMISSIONS BY AGE <65 65-75 >75 7 14 12 7 4 12 3 4 8 8 4 8 8 16 15 9 MONDAY 4 6 TUESDAY 9 WEDNESDAY THURSDAY 10 6 FRIDAY SATURDAY SUNDAY FRAILTY SCREENING FOR >65 IN MAU Frail Screen positive, but not frail Not frail 5 4 7 5 2 4 2 6 10 7 3 5 1 11 6 5 7 6 3 2 2 MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY SATURDAY SUNDAY Frail Non-frail 47 56 79.3 (8.1) 68 - 101 75.8 (6.3) 65 - 90 <0.05 18.2 (20.7)* 11 (4.25 – 22.75)* 1 – 85* 7.6 (12.1) 3 (1 – 6) 1 - 57 <0.05 Readmission (%) 7 day 30 day 60 day 2 (4.3) 8 (17) 8 (17) 6 (10.7) 12 (21.4) 15 (26.8) NS NS NS Mortality (%) Inpatient 7 day 30 day 60 day 7 (14.9) 3 (6.4) 7 (14.9) 8 (17) 5 (8.9) 1 (1.8) 2 (3.6) 7 (12.5) NS NS <0.05 NS n Age, years Mean (SD) Range Length of stay, days Mean (SD) Median (IQR) Range p-value * 2 patients are still inpatients Frailty ‘A biologic syndrome of decreased reserve and resistance to stressors, resulting from cumulative decline across multiple physiologic systems, and causing vulnerability to adverse outcomes' Walston et al. Research Agenda for Frailty in Older Adults: Toward a Better Understanding of Physiology and Etiology: Summary from the American Geriatrics Society/National Institute on Aging Research Conference on Frailty in Older Adults. JAGS 2006; 54: 991-1001 Vulnerability of frail elderly people to a sudden change in health status after an illness Clegg, Young, Iliffe, Rikkert, Rockwood Frailty in elderly people Lancet 2013; 381: 752 - 762 Survival curve estimates by frailty status at baseline Fried L P et al. J Gerontol A Biol Sci Med Sci 2001;56:M146-M157 Comprehensive Geriatric Assessment Multidimensional diagnostic and treatment process that identifies medical, psychosocial, and functional limitations of a frail older person in order to develop a coordinated plan to maximize overall health with aging Domain Medical Assessment Mental health Cognition Mood & anxiety Fears Spirituality Functional capacity Basic activities of daily living Gait & balance Activity / Exercise status Instrumental activities of daily living Social circumstances Support from family & friends Social network eg. Visitors, daytime activities Finances Eligibility for care resources Environment Home facilities, comfort & safety Potential use of telehealth technology Transport facilities Access to local resources Co-morbidity & disease severity Medication review Nutritional status & dentition Continence Vision & hearing Advance care preferences Geriatrician GP Pharmacist Social Worker Case Manager Physiotherapist Occupational Therapist Dietician Speech & Language Therapist Nurse Assessment Intervention CGA Goals Problem list CGA vs. usual care Outcome Living at home Up to 6 months End of follow up Mortality Up to 6 months End of follow up Institutionalisation Up to 6 months End of follow up Death or deterioration No. of studies No. of participants Effect size 14 18 5117 7062 1.25 [1.11, 1.42] 1.16 [1.05, 1.28] 19 23 6786 9963 0.91 [0.80, 1.05] 0.99 [0.90, 1.09] 14 19 4925 7137 0.76 [0.66, 0.89] 0.78 [0.69, 0.88] 5 2622 0.76 [0.64, 0.90] Ellis G, Whitehead MA, O'Neill D, Langhorne P, Robinson D. Comprehensive geriatric assessment for older adults admitted to hospital. Cochrane Database of Systematic Reviews 2011, Issue 7 CURRENT MODEL OPD SJH Front door Gen Med Ward Refer PT OT MoE A&E GP PAA Rehab ward Discharge Unwell frail older person Templar Day Hospital REACT Boarding ward MAU GP Principles Right to medical diagnosis and equal access to specialists Patient-centred Home is best The right patient looked after by the right team in the right setting Planned care better than emergency care Simple Sustainable Focus on quality and quality improvement Case-finding for targeted intervention Frail patients identified as soon as possible to enable timely assessment and management Specialist nurse supported by Consultant Geriatrician Systematic MDT on all medical wards Robust referral system from other parts of the system Health Improvement Scotland: Think Frailty MAU SJH MAU SJH MAU SJH MAU SJH Right patient, right team, right setting Prompt decision on care trajectory and transfer to most appropriate setting Complex frail patients managed by consultant geriatricians Tracking of less complex frail through liaison Effective MDT in each ward with regular discussions for goal setting and discharge planning Home is best Admission avoidance Hospital at Home Rehab at Home Templar Rapid Access Frailty Clinic Rapid access CGA in a specialist multidisciplinary ambulatory setting A ‘one-stop’ clinic offering specialist assessment and same-day diagnostics with realtime decision-making led by a geriatrician Referrals via telephone to the MoE Single Point of Contact (SPOC) with appointments for the same or the next working day given in the same conversation Aim to reduce avoidable admissions and facilitate timely discharge when acute hospital care no longer necessary Close working with REACT, MAU/PAA, Reablement, Crisis care, Primary Care, Social Work, Mental Health and other specialties Home is best Admission avoidance REACT Templar Rapid Access Frailty Clinic Discharge to assess Improving Flow Patient Admitted D2A Assessment Seen by Doctor Seen by nurse Rehabilitation OT and PT assessment Care at home Discharge Home Care at Home Discharge Home Discharge Planning Rehab in hospital Physio Assessment OT Assessment Home is best Admission avoidance REACT Templar Rapid Access Frailty Clinic Discharge to assess “Medically stable” vs. “No longer in need of acute hospital care” Rehab at home Closer working with community services Simple Single point of contact Telephone or electronic contact Reproducible and scalable Good post-acute care CGA initiated and completed Reassessment Identify patients with highest risk of readmissions, deterioration Advance care plans SJH Front door A&E PAA Frailty nurse MAU Inpatient admission required GP Rest of SJH Discharge hub Referral or MDT pick up Rehab ward REACT Safe for discharge Unwell frail older person Screen all ≥65s FRAILTY PATHWAY ST JOHN’S HOSPITAL Medical ward under a geriatrician Consultant Geriatrician Single Point of Contact OPD Templar Day Hospital GP care + agreed plan Subacute care Summary Frailty is our core business Early identification allows targeted CGA CGA is multidimensional, multidisciplinary and iterative Evidence-based changes to system to allow great frailty care everywhere Discussion