Shoulder Pain and the Shoulder Exam
advertisement

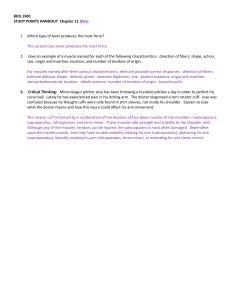
Shoulder Pain and the Shoulder Exam CHA Ambulatory Didactics Kate Lupton, MD Shoulder Overview • Very complex structure with tremendous ROM • 4 joints – sternoclavicular, acromioclavicular, glenohumeral, scapulothoracic • Glenohumeral – ball and socket joint (golf ball on a tee), glenoid only covers 25% of humeral head Anatomy Shoulder Activity/ROM • Static glenohumeral stability – joint surfaces, capsule and labrum • Dynamic stability – RC & scapular rotators (trapezius, serratus anterior, rhomboids, levator scapulae) • Rotator cuff – depress humeral head against glenoid • Internal rotation - Subscapularis • External rotation - Infraspinatus, teres minor • Abduction - supraspinatous • Scapular stability – trapezius, serratus anterior, rhomboids • Upward scapular rotation – trapezius & serratus anterior • Scapular retraction – trapezius & rhomboids History • Background – Handedness, occupation, recreational activities • CC: Pain vs instability vs decreased movement • Characterize CC: “loose” arm, “dead” arm • Injury? -> Mechanism • Associated Sx – neurovascular, stiffness, crepitus • Function – putting on jacket, overhead activities, sleeping Principles of the MSK Exam • Good exposure (clothing removed, in gown) • • • • LOOK FEEL MOVE SPECIAL TESTS Look/Feel - Surface Anatomy Look • SEADS – swelling, erythema, atrophy, deformity, scars • Dominant shoulder usually slightly lower than non-dominant side • Head forward posture, shoulders rolled forward, scapula protracted • Squaring of shoulder – r/o dislocation • SC joints, clavicle deformity - ?fracture • AC joints – step deformity - ?separation • Atrophy – trapezius, infraspinatus, teres minor Feel • Palpate joints – SC joint, along clavicle, AC joint, coracoid process, along scapula • Palpate muscles and tendons – trapezius, posterior shoulder, biceps tendon, supraspinatus insertion • Feel for crepitus while rotating the arm Move – Active Range of Motion Flexion/Extension • Trace arc while reaching forward with elbow straight • Normal flexion to 160°180°, extension to -60° Abduction/Adduction • Trace arc reaching to side with straight arm • Normal range is 0°-180° Move – Active Range of Motion Abduction & internal rotation • Should be able to reach to ~C-7 level (prominent bump on C-spine) Adduction & external rotation • Should be able to reach lower border of scapula (~T7 level) Move – Passive ROM • If pain or limitation w/ active ROM, assess with passive ROM testing • Grasp humerus, move through flexion/extension, abduction, adduction • Feel for crepitus with hand on shoulder • Note movements that precipitate pain – pain/limitation on active but not passive ROM suggests muscle/tendon problem • Note limitations in movement – where in arc does it occur? Due to pain or weakness? Symmetric or asymmetric? Move • Painful arc on abduction? Glenohumeral joint from 60-120°, AC joint 170-180° • Watch scapular motion – look for asymmetry, jerky motion • Wall push-up for scapular winging Rotator Cuff Anatomy and Function • 4 Major Muscles • Depress humeral head, keep it in contact with glenoid throughout wide ROM • Supraspinatus – abducts shoulder (to ~80°) • Infraspinatus – external rotation • Teres minor – external rotation • Subscapularis – internal rotation Special Tests - Supraspinatus Empty/Full Can Test • Hold arms at 1:00 and 11:00, abducted 30 ° • Internally rotate so thumbs point down (“empty can”), pt lifts up against resistance. Repeat with thumbs pointed up • Note pain (tendinopathy, partial tear), weakness (tear) • Deltoid is responsible for abduction beyond 70-80 ° Special Tests – Infraspinatus External Rotation • Fully adduct arm, flex elbow to 90 °, medially rotate humerus 45 ° (hand at 12:00) • Have pt try to externally rotate while you resist against their forearms Special Tests - Subscapularis Posterior (Gerber’s)Lift Off • Pt places hand behind back, palm facing out • Pt lifts hand away from the back • Note pain, weakness Belly Press • Place hands on abdomen, elbows out • Press in on abdomen or keep elbows out while posteriorly directed force is applied to elbows • Positive test if unable to keep elbows out Shoulder Impingement/Bursitis • 4 tendons of the RC pass under the acromion and coracoacromial ligament and insert in the humeral head • Space between arcromion, coracoacromial ligament and tendons can narrow, causing impingement of tendons (esp supraspinatus) • Resulting friction inflames tendons and subacromial bursa • Causes shoulder pain, esp with reaching overhead Special Tests - Impingement Neer’s Test • Place hand on pt’s scapula, other on forearm • Pt fully internally rotates (thumb pointed down) • Passively forward flex arm through full range of motion • Pain = impingement Special Tests - Impingement Hawkins-Kennedy Test • Flex arm to 90° • Stabilize shoulder with one hand • Forcibly internally rotate shoulder, thumb pointed down • Pain = impingement Special Tests - Bursitis Subacromial Palpation • Identify acromion by following scapular spine to distal end • Palpate in subacromial space • Pain = inflamed bursa and/or tendons Biceps Tendon • Long head of biceps tendon runs in the bicipital groove of humerus, inserts at superior glenoid • Biceps flexes and supinates forearm • Subject to similar stresses as RC tendons • Inflammation causes pain in top and anterior shoulder, especially with flexion/supination Special Tests – Biceps Tendon Palpation • Palpate along biceps tendon/bicipital groove • Confirm location by having pt supinate while palpating Yergason’s Test • Flex elbow to 90°with arm adducted (elbow against side) • Grasp pt’s hand, resist while they supinate • Pain = tendinopathy Special Tests – AC Joint Palpation • Palpate point at which distal clavicle articulates with acromion O’Brien • Flex shoulder to 90° while internally rotated (thumb down) • Adduct arm 10-15° from 12:00 • Apply downward force to arm while pt resists • Repeat with thumb pointed up • If there is pain with first maneuver and not second, indicates labral or AC joint pathology Cross Arm /Forced Flexion • Flex shoulder to 90°, flex elbow, then actively adduct Special Tests – Shoulder Instability Apprehension/Relocation • With patient supine, abduct shoulder 90°, flex elbow 90° • Externally rotate shoulder by moving forearm from perpendicular to parallel with body • Pain or sense of instability with further external rotation is a positive test, indicating anterior shoulder instability • If sx are relieved with posterior force applied to proximal humerus, that is a positive relocation test and further supports dx Sulcus Sign • Arm hangs relaxed at the side • Pull arm straight down, look for stepoff under lateral acromion • Indicates inferior instability Many Thanks • Anthony Luke, MD – UCSF • Charlie Goldberg, MD - UCSD