child with a physical disorder
advertisement

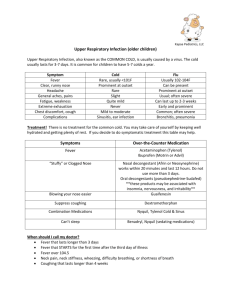
Common Problems Ages 1-18 Years White 2nd ed Christensen 5th ed Leslie Lehmkuhl, RN 2008 Terms Acanthois nigricans Comedome Encopesis Epistaxis Gowers’ sign Rhinorrhea ii Upper Respiratory Infections (viral or bacterial) See Table 57-1 Nasopharyngitis (common cold) is viral 6-9 colds per year Tx symptoms (e.g. rhinorrhea, congestion, sneezing, fever, muscle aches) and usually self resolves in 3 days Pharyngitis viral or bacterial Most common in 4-6 yo Tx symptoms (e.g. sore throat, inflammation, HA) and if caused by streptococcal infection teach parents to finish all ATB’s. Note enlarged lymph nodes, tender cervical lymph nodes. Influenza viral Treat symptoms (e.g. chills, fever, mylagia, cough, congestion, HA Highest among school age children. With all three enc. rest, use nonASA antipyretic/analgesics, PO decongestants, nasal saline gtts, warm salt water gargle, humidifier, fluids, clear or bland liquids, tea and honey. 0 Allergic Rhinitis Commonly called "hay fever," Irritation of the nose where the inside of the nose becomes inflamed after being exposed to an allergic trigger. It often is associated with asthma and sinusitis. Familial predisposition Etiology: dust, fomites e.g. mop head, feathers, animal dander, spores Manifestations: itchy nose, mouth breathing, dark circles under the eyes from congestion, “allergic salute” (transverse crease from pushing nose upward and backward in attempt to relieve itching). Allergic Rhinitis (continued) Management: allergy skin testing, CBC with elevated eosinophil count Immunotherapy includes allergy shots Antihistamines, decongestants Avoid wool and down blankets, humidifier in home, keep pets outside if possible “allergic salute” Tonsils Tonsil glands are located in the back of the throat. They contain immune cells which fight infection. Tonsils progressively enlarge at 2-10 years old and is considered normal. By pre-adolescence they reduce in size. Inflamed Tonsils Tonsillectomy is advisable when tonsillitis attacks are so frequent (5 or more a yr) or severe that they affect a child's general health or interfere with school, hearing, or breathing. However, tonsillectomies are thought to be done more often than necessary, so a second opinion should be obtained when there is any doubt. Tonsillectomy Under general anesthesia, the ear-nose-throat (ENT) surgeon holds the mouth open and pulls the tongue forward to reveal the tonsils. The tonsils are pulled away from the back of the throat and then removed by being cut away. Bleeding is controlled, and often the cut heals naturally without stitches. Tonsillits Inflammation of palatine tonsils in throat resulting from pharyngitis. Etiolgy: viral or bacterial Note: 2-10 years of age tonsil are normally enlarged and reduce in size during pre adolescence. Manifestations: sore throat, cough, vomiting, muscle ache, difficulty swallowing, tonsils enlarged and bright red, mouth breathing, if adenoids enlarged; May have sleep apnea, hearing problems Tonsillitis Tests: CBC, C&S of throat Streptococcus is cause of 15% of pharygitis for children under 3 years Peak age is 4-7 years Spread is by droplets Antibiotics for management Surgery for recurrent infection Post surgery monitor for: frequent swallowing, elevated pulse rate, restlessness not related to pain No: red liquids, popsicles, straws, carbonated drinks, citrus, very hot or very cold fluids Often vomit from anesthesia, ice collar Soft diet when able to swallow Tonsillitis Bleeding most common: Within 24 hours of surgery 7-10 days post surgery when the tissue sloughs off from the scar site Watch for restlessness, anxiety, frequent swallowing and rapid pulse. Call if temp 101 or above, earache, bleeding, avoid crowds for 2 weeks Asthma Bronchial asthma Reactive airway dz that causes narrowing or obstruction of the airway. Highest incidence in first year of life Affects 9 million children under 18 years Affects 10% of all school age children Leading cause of absenteeism school and most common admitting diagnosis. More common in boys until puberty S/S: dry hacking cough or productive, wheezing and difficulty breathing. Asthma Etiology: history of allergies in family, smoke, stress, exercise, trees, peanuts…do not have to have allergies to have asthma Assess triggers to prevent future episodes and cause no further damage. Reversible airway obstruction Tests: pulmonary function, ABG,CBC,CXR Management: bronchodialators-albuterol, theophylline (narrow therapeutic range, watch for irritability, restless, insomnia, HA, V, D) Cromolyn sodiumnonsteroid antiinflammatory-may prevent asthma. Prednisone a corticosteriods Asthma Children's airways are narrower than those of adults. This means that triggers that may cause only a slight problem in an adult can create more serious problems in children. In children, an asthma attack can appear suddenly with severe symptoms. For this reason, it is important that asthma be diagnosed and treated correctly. Some children may need to take medicine every day, even when they do not have symptoms. Foreign Body Aspiration Inhaling any foreign object into respiratory tract. At risk when playing, running, laughing Most frequent age 6 months to 4 years Etiology: popcorn, peanuts, dry beans, grapes, coins, toys, balloons, earrings, hot dog Manifestations: sudden violent spasmodic coughing, vomiting, gagging, wheezing, may have brief episode of apnea, cyanosis, resp distress. Management: laryngoscopy, bronchoscopy Cool mist for 24-48 hours, bronchodilators, corticosteroids Rheumatic fever Rheumatic Fever Multi-system (e.g. heart, joints, lungs, brain) autoimmune condition From an untreated group B hemolytic streptococcus infection (e,g. strp throat, scarlet fever). Rheumatic fever In connective tissue, heart, joints, brain.. Manifestations: high fever, headache, chills, acute Tonsillitis, red strawberry tongue by day 4, red painless rash, warm erythematous joints, inflammation of endocardium, valves, myocardium, small nontender lesions on tendon sheaths of joints, murmur Rheumatic Fever Minor S/S Fever Listlessness Anorexia Pallor Wt loss Muscle Joint or abd pain Major S/S Polyarthritis Carditis Erythema marginatum (red skin lesions) Subcutaneous nodules Elevated ASO titer * Rheumatic Fever Subcutaneous skin nodules Rheumatic Fever Skin rash (erythema marginatum) Rheumatic Fever Rheumatic Fever Because this disease has different forms, there is no specific test that can firmly diagnose it. Your doctor will perform a careful exam, which includes checking your heart sounds, skin, and joints. Your doctor may also do an electrocardiogram while testing your heart. You may have blood samples taken to test for recurrent strep infection (such as an ASO test), complete blood counts, and sedimentation rate (ESR). Several major and minor criteria have been developed to help standardize rheumatic fever diagnosis. Meeting these criteria, as well as having evidence of a recent streptococcal infection, can help confirm that you have rheumatic fever. Rheumatic Fever Goal is to treat any existing strep infection Rx: PCN, Salicilytes for pain, fever reduction and inflammation, Corticosteriods for carditis, dig and diuretics for CHF Low Na+ diet BR to reduce cardiac workload can be weeks even months depending on the severity of heart status. Heat and cold packs to affected joints Leukemia cells Acute lymphoblastic leukemia Highest in age 3-5 3,000 new cases a year Etiology: genetic altered stem cell and cells produce the defective cell rapidly forms increased number of immature or blast cells Blast cells released into circulation ….Replication continues Leukemia Patho: bone marrow replaced by malignant blast cells, neutropenia, decreased RBC’s, platelets producing anemia, thrombocytopenia All –acute leukemia lymphocyticoriginates in B lymphocytes and T lymphocytes Leukemia Manifestations: pallor, excessive bruising, leg/bone pain, abdominal pain, fever, malaise, Hepatosplenomegaly, abnormal elevation of WBC (lymphocytes), anemia, neutropenia?? and decreased RBC’s. Complications: bleeding, death, sepsis, anemia Leukemia Tests: CBC, bone marrow aspirate, lumbar puncture for mast cells, electrolytes, uric acid level, bone scan Management:combination of chemo over 2-3 years, prednisone, vincristine over 2-3 years, Prognosis is good if remission occurs. Bone Marrow Aspiration A small amount of bone marrow is removed during a bone marrow aspiration. The procedure is uncomfortable, but can be tolerated by both children and adults. The marrow can be studied to determine the cause of anemia, the presence of leukemia Leukemia Daily and weekly doses of medication Bone marrow aspirate and spinal puncture in 30 days after chemo Chemo, radiation effects: Anemia, bleeding, urinary tract infection, hair loss, nail loss Idiopathic Thrombocytopenia Purpura (ITP) Bleeding disorder characterized by too few platelets in the blood. This is because platelets are being destroyed by the immune system. Blood Platelets under 20,000 More common in age 24 years Auto immune disorder often preceded by a viral infection Child may not feel bad Manifestations: nose bleed, hematuria, melana, hematemesis, subarrachnoid hemorrhage Idiopathic Thrombocytopenia Purpura (ITP) The disease occurs when immune system cells, called lymphocytes, produce antibodies against platelets. Platelets are necessary for normal blood clotting. They clump together to plug small holes in damaged blood vessels. The presence of antibodies on platelets leads to their destruction in the spleen. A characteristic skin rash, easy bruising, abnormal menstrual bleeding, or sudden and severe loss of blood from the digestive tract may occur. Usually, no other abnormal findings are present. In children, the disease sometimes follows a viral infection, and usually runs its course without treatment (self limiting), with the platelet count returning to normal within 6 months without therapy. Idiopathic thrombocytopenia.. Tests: CBC, platelet count Replace blood, blood products, gama globulin Spleenectomy if needed to modify disease No ASA or ASA products, soft bristle tooth brush Hemophilia Hemophilia Hemophilia refers to a group of bleeding disorders in which it takes a long time for the blood to clot. This may cause abnormal bleeding. In most cases, the disorder is passed down through families (inherited) and most often affects males. Hemophilia Sex linked heredity disorder carried by x chromosome Male inherits from mother Bleeding problems by age 4 yr (however neonatal bleeding from the umbilical cord or circumcision site may be an early manifestation of severe hemophilia). Hemophilia A lack of factor viii Hemophilia B Christmas disease lack of factor ix Hemophilia Bleeding after surgery, trauma or from no apparent reason Tests: PT, ptt, fibrinogen level platelet count, factor viii, factor ix, cbc, platelet count, coagulation profile Hemophilia Medication to stop bleeding: desmopressin acetate, amicar, cyclokapron No asa or asa products factor viii or factor ix replacement Prognosis good No contact sports, ID bracelet Hemophilia Care with bicycling, hiking, bowling, golf, running, prevent falls Watch for intracranial bleed Headache, vomiting, disorientation Common GI Problems Constipation Intestinal Parasitic Infections Constipation Infrequent or difficult passage of hard dry stools d/t to medication, low fiber diet, decreased fluid intake… Manifestations: hard dry stool , cramping, pain without abd dist, blood in stool, paplpable fecal mass inside retum, xray. Management: increase fluid, fiber, increase fruit and vegetables, daily exercise, toilet training, allow plenty of time to defecate. Impaction use enema Stool softners, laxatives, mineral oil may be used Prognosois is good Parasites Giardiasis Giardiasis is an intestinal infection caused by a protozoan and is spread by contaminated water or contact with an infected person. People who are travelling or hiking should assume water sources are contaminated and either purify drinking water or drink bottled water.. Parasitic infections Giardiasis Transmission Person to person Untreated water Contaminated food Animals Soil Feces Anal sex with infected person Manifestations: diarrhea, weight loss, abdominal cramping Fecal smear Institutional Hygiene Pinworm, Close-up of the Head This is the head of a pinworm. Pinworms are most common in children. They are easily transmitted and sometimes appear in small outbreaks among school children. Pinworm Eggs Pinworms are a common problem in children and may spread to adults (typically the parents or other care-givers). The eggs may be easily seen under a microscope. To obtain a sample, a piece of cellophane tape is pressed against the patient's anal opening. The sticky side of the tape picks up the pinworm eggs and the tape is then stuck to a microscope slide. The eggs can be viewed under the microscope, as seen Parasitic Pinworm is a white threadlike worm Transmission Person to person Ingest or inhale eggs Untreated water Poor hygiene Common in school age children Manifestations: itching around anus, irritability Cellophane tape to capture eggs early am Roundworm The adult worms multiply by producing eggs called ova or larvae. The eggs usually become infectious soil Intermediate host before humans are infected. It is interesting to note that unless the worm infection is heavy, many individuals do not show signs of infestation. Parasitic Roundworm pink worm 9-12 inches Transmission eggs passed hand to mouth May migrate to liver or lungs Manifestations: abdominal pain, abdominal distention, vomiting, jaundice, pneumonitis Fecal smear Parasitic Hookworm Transmission: skin penetration and contact with contaminated soil May migrate to lungs Manifestations: anemia, dermatitis, pneumonia, malnutrition Well balanced diet with increase protein and Fe to replace lost nutrients. Fecal smear Hookworm This is the mouth part of the hookworm Ancyclostoma duodenale. The hookworm uses sharp, curved cutting plates to attach to the lining of the intestine where it sucks blood for nourishment The oral opening of this species contains cutting "plates" as opposed to "teeth". Endocrine Type 1 Type 2 DM Type 1 Type 2 Diabetes Mellitus in Children Type 1 formally called “juvenile onset diabetes” and/or “insulindependant diabetes” Most common is type 1 increase of number in type 2 associated with childhood obesity Children often manifest with polyuria, polydipsia, polyphagia Weight loss, fatigue and blurred vision Children may need glucose or snacks after exercise Toddlers are difficult to control as they can refuse to eat Diabetes Mellitus in Children Most school-age children are able to learn and give their own insulin injections. Diet and exercise for DM II. However, most may need drug therapy eventually. Musculoskeletal D/O’s in Childhood Scoliosis Legg-Calve’-Perths Duchenne Muscukar Dystrophy Juvenile Arthrirtis Fractures Scoliosis Signs of Scoliosis One shoulder appears to be higher than the other, there is a curvature in the spine, or the pelvis appears to be tilted. The treatment of scoliosis can involve the use of a brace or surgery. Treatment is determined by the cause of the scoliosis, the size and location of the curve, and the stage of bone growth of the patient Scoloisis Lateral curvature of the spine more in female adolescents Manifestations Unequal hip and shoulder height, rib asymmetry Scapular and rib prominence Posterior hump when child bends forward at the waist Forward Bend Test The forward bend test is a test used most often in schools and doctor's offices to screen for scoliosis. During the test, the child bends forward with the feet together and knees straight while dangling the arms. Any imbalances in the rib cage or other deformities (e.g. uneven shoulder or pelvic heights, posterior rib hump) along the back could be a sign of scoliosis. Scoliosis Test: x-ray Management: curvature under 20 degrees- no treatment Orthotic brace: boston or thoracolumbosacral Surgery-spinal fusion and stabilizing rod as harrington rod or l rod With brace continuous monitering of curvature. Suspect non-compliance if curavture becomes more pronounced. Post operative: log roll q2h, vs, pain level, wound care, monitor for bleeding, bowel and bladder function, neuro checks with vital signs (warmth, color, sensation, movement, pulses, swelling, burning)in legs Legg-Calve-Perthes Disease Etiology: decreased blood supply to femoral head resulting in epiphyseal necrosis and degeneration of femoral head and calcification Unknown cause Ages 4-8 yr caucasion boys most affected S/S include pain, limp, limited rom, worse with activity Decreased pain with rest Tests: x-ray Management: traction, bed rest, cast, brace or harness Goal: to maintain head of femur in acetabulum and preserve normal shape as regeneration occurs Blood Supply to Bone Bones require their own blood supply which travels through the periosteum to the inner bone marrow. Surgical tx is often treatment of choice as it reduces time and eliminates compliance issues. Legg-Calve-Perthes Duchenne’s Muscular Dystrophy Sex-linked (X-link recessive) inherited disease with progressive muscle wasting, and weakness Ages 2-4.. Onset of disease almost exclusively in males. Onset subtle and later progresses rapidly waddling gait, difficulty running, climbing.. By 12 years the child may lose the ability to walk. Genetic Counseling is recommended for parents, female siblings and maternal Aunts. Genetic Counseling and Prenatal Diagnosis Muscular dystrophy Juvenile arthritis JRA occurs in 50-100 per 100,000 children in the United States. It usually occurs before age 16. S/S- stiffness, edema, loss of motion, synovial thickening, macular rash on trunk, pain, joint swelling Tests: ESR erythrocyte sedimentation rate Prognosis is good if caught early Juvenile arthritis Drug therapynonsteroidal antiinflammatory medication as naprosyn, motirn, aspirin, gold, corticosteroids(spari ning), cytoxic meds, Rest, normal exercise, heat Greenstick Fracture Only one side of the bone has been broken. The bone usually is "bent" and only broken of the outside of the bend. It is mostly seen in children because of incomplete ossification, and is considered a stable fracture due to the fact that the whole bone has not been broken. As long as the bone is kept rigid healing is usually quick. Fractures Common sites long bones, wrist, clavicle, fingers, skull Can be complete or incomplete fracture Nx intervention calm and reassure child, assess pain, color, sensation, motion, pulses management cast or splint Fracture Immune System/ Communicable Diseases Chix pox Diptheria Fifth disease Hep B Mesles Mono Mumps Whooping Cough Poliomyelytis Roseola German measles Scarlet fever tetanus Varicella Chicken pox, varicella zoster (Viral) Transmission direct contact with resp tract secretions Manifestations: low grade fever, pururtic rash, starts as a macule progressing to fluid filled papule, vessicles rupture and ooze, crusting lesions occurs Treat with antihistamines, oatmeal baths and lotion to deter itching. Vaccine available Varicella-Zoster Macular rash that progresses to papules to crusted lesions Diptheria corynebacterium dipheriae Direct contact (e.g.nasal drainage),or indirect through contaminated atrticles. Pharyngitis, anorexia, low grade fever, laryngeal cough.. Complications: airway obstruction, thrombocytopenia Treat with antibiotics and analgesics Vaccine available Diptheria Membraneous lesions on tonsils Erythema Infectiosum Fifth’s disease human parovirus b 19 transmission: resp tract secretions, blood Manifestaions: fever, malaise. Fiery-red cheeks (“slapped face”). Rash red rash on face— maculopapular, rash on upper extremities to trunk and thighs. Lasting 1 week or more Treatment supportive measures No vaccine available Erythema infantosum Hepatitis B Transmissionvia blood and sexual contact Flu like symptoms, jaundice Hep B vaccine available Rubeola Measles paramyxovirus Transmission via direct contact from resp secretions, blood, urine of infected person Manifestations: malaise, kopilk’s spotsblue/white spots with a red base in buccal mucosa…. Maculopapular red rash, lasting 7 days Rash begins behind the ears or at the hairline and spreads downward on body Supportive treatment Vaccine Available Mononucleosis Epstein-barr virus Transmission via saliva, blood products Manifestations: fever, sore throat, enlarged lymph nodes, hepatospleenomegaly Treatment includes supportive care, antipyretics, analgesics No vaccine available Mononucleosis Mumps or Paratitis Etiology: paramyxovirus Transmitted by direct contact of respiratory secretions S/S fever, malaise, headache…tenderness of parotid gland unilateral or bilateral edema Treat w/ supportive care, antipyretics and analgesics Vaccine available Mumps or Paratitis Enlarged parotid gland, earache aggravated by eating ususally accompanied w/fever Pertussis AKA Whooping cough. Bordetella pertusis Respiratory droplets transmission, including running nose. Manifestations: cough, dry, hacking cough paroxysms of coughing, followed by prolonged inspiratory “whoop”, sound when child takes a breath, lasts 1-2 weeks Complications: otitis media, atelectasis, pneumonia, weight loss, hemorrhage from expistaxis Management antibiotics, anti-seizure treatment for those with seizures, iv therapy, cool mist Prevention: vaccine Pertussis Paroxsmal cough, followed by a whoop sound Roseola infantum 6th disease Children age 6-24 months Sudden onset, high fever last to 4 days child seems well Rose-pink macular rash on trunk going to rest of body Lasts 1-2 days Complication: febrile seizures Treat with antpyretics and supportive care 6th disease Rubella German Measles, 3 day measles Airborne, direct contact with droplets, transplacental S/S fever, HA, malaise, running nose, maculopapular rash progressing fro head to extremities. Supportive care Vaccine available Rubella Maculopapular rash over entire body Rubella Scarlet Fever Group A hemolytic strep Airborne, resp droplets and contaminated items S/S strawberry tounge, abd pain, sore throat, skin that peels on hands Scarlet Fever Treat with PCN, antipyretics, analgesics Tetanus Lockjaw Direct contact of skin wound w/contaminated soil of a bactyeria spore S/S Stiffness of neck and jaw, difficulty breathing. Supportive care Vaccine available Tetanus Integ Impetigo Cellulitis Fungal infections Viral infections Infestations Animal bites Spider bites Tick bites Insect bites Contact dermatitis Acne Burns Impetigo Common skin infection, often begins in open skin S/S macules that change to papules vesicles that rupture with crusty honey colored over red base. See 57-11 Impetigo Cellulitis Cellulitis staph a strep b Haemophilus influenzae Manifestations: pain, redness, edema, lymph node enlargement Management:antibiotics , moist compresses, hydration, bedrest, may elevate affected extremity Tinea capitis, tinea corporis, tinea cruis.. Fungal infections of the skin Tinea capitis-scalp Corporis-trunk and extremities Cruis-inguinal area Pedis- athletes foot Treatment: antifungal medication, lotritmin, monostat, oxistat Treatment: antifungal medication, lotritmin, monostat, oxistat Tinea capitis Herpes Simplex Type 1 HSV-1 in 30-60% of youth Termed cold sore, fever blister Virus that remains dormat within nerve cells and is reactivated by fever, stress, trauma, sun exposure immune suppressed Transmitted by direct contact with body fluid Pediculosis Head lice , pediculosis capitus Causes intense pruritus Louse attaches to skin and sucks blood .. lays eggs in hair shaft.. Eggs hatch in 7-10 days Treatment: kwell, rid, pronto, triple x, repeat in 1-2 weeks Check head and body Lice cannot transmit from hand to hair so the use of gloves is unecessary. Pediculosis Parasitic Scabies are mites that burrows under the skin with feces and eggs left under skin papular rash with pruritus Transmission by direct contact Management: kwell/lindane rid, elimite retreat in 1 week Wash all clothing in hot water Scabes Traumatic injuries Human bites Insect bites Sunburn Dogs: laceration/avulsion Cats: puncture Bite area: face, scalp, upper extremities Dog bite Animal Bites Children under 4 years of age are often biten most frequently because of their ht and close proximity to a dogs face. Atb, tetnus Spider Bites Black widow: red edematous area, dizziness, weakness, abd pain, paraylsis, shock, renal failure Brown reculse: bite causes a necrotic ulcer that takes months to heal, nausea, vomiting, joint pain These spiders are nonaggressive, avoid light (e.g. closets, woodpiles) and bite only in self defense Black widow Venom is neurotoxic and may cause dizziness, weakness Abd, pain, paralysis, seizures, and possibly death. Black widow bite Brown recluse spider Venom is necrotoxic, with the bite progressing to a necrotic Ulcer within 1-2 weeks. This bite is not fatal, but ulcer may take months to heal. Brown recluse bite Skin Impetigo=staph aureus infection Honey crusting over an ulcerated base Mouth and nose Manifestations: lesions bleed if crusting removed Soak off crusts wash with soap and water 3 times a day Contact dermatitis Inflammatory reaction to allergens soap, wool, dyes, citrus, bubble bath Manifestations: dry, inflamed pruritic skin, may have macules or papules Tests: skin testing for allergen Management: cool wet dressings of burow’s solution or aveeno bath, a&d, desitin, antihistamines To not use caladryl (benedryl) due to possible toxicity calamine recommended for children Steroid 1% cream BID Contact Dermatitis Acne Vulgaris Inflammatory process common in adolescence Involves face, neck, shoulders, back, upper chest Management: retin-a, tretinoin Use sunscreen Topical: benzoyl peroxide inhibits organism growth Management: antibiotics for topical use clindamycin, erthromycin, metronidazole Systemic antibiotics if local do not work: tetracycline, erythromycin, clidamycin… Accutane monitor for depression Acne Vulgaris Burns Carless adults, children curiosity, increasing mobility, failure to adequately supervise contribute to high incidence of burns in children. Urinary tract infection Infection of kidney, ureters, bladder.. Bacteria, congenital anomaly manifestations: Painful urination, flank pain, hematuria, vomiting, fever, weight loss, feeding problems Tests: c&s of urine Management: antibiotics, push fluids, repeat urine culture after antibiotics completed Complications: kidney infection, renal failure Acute glomerulonephritis Inflammation of glomeruli of kidney Patho: strep, pneumococcal, viral, hemolytic beta strep, throat infection=strep fixed to glomeruli of kidney…edema occurs.. Filtration decreases.. Accumulate sodium and water in blood… causes edema and circulary congestion..Protein escapes in urine Glomerulonephritis S/S: Hematuria, proteinuria, hypoalbuminemia, oliguria, urine brown to tea colored , abd pain, pallor, low grade fever, hypertension, heart failure Glomerulnephritis Tests: urinalysis, culture and sensitivity, antistreptolisin titer for strep management: Bed rest, restrict: fluid, sodium and potassium VS, weight, I&O, antibiotic, antihypertensive medication.. Prognosis good, No treatment lab values usually self resolve in 612 weeks. Glomerulnephritis Nephrosis Nephrotic Syndrome Protenuria, edema, hyperlipidemia, hypoproteinemia Types: primary or idiopathic Secondary or caused by another disease congenital Patho: autoimmune response Allows protein to escape in urine ..Proteinuria and low level in blood or hypoproteinemia Decreased osmotic pressure allows fluid to leak interstitual=edema Nephrosis.. Low fluid volumeretention of sodium and water-increases edema Manifestations: preorbital edema, weight gain, anasarca, decreased urine output, pallor Tests: cbc, urine-fat bodies in urine, bun, creatinine, serum protein level.. Flu and pneumonia vaccinations recommended when the child is in remission. Nephrosis Management: low sodium intake, bed rest, prednisone for 7-21 days to initiate remession, diuretics, increase protein Monitor urine output, elevated glucose, abdominal pain, check urine for protein, vs, weight Nephrosis Enuresis Involuntary urination after control has been established Etiology: urinary tract infection, stress, pinworms, diabetes mellitus, sexual abuse, sickle cell anemia Management: ua, c&s, fluid restriction after 6pm, ditropan Review Obestiy Anorexia Bulemia Attention deficit Suicide Obesity Obesity Obesity is a term used to describe body weight that is much greater than what is considered healthy. Excessive body fat >20%. Factors: overeating, lack of parental knowledge on nutrition and food preparation, unstructured mealtime, genetic predisposition, peer pressure. Anorexia Anorexia and Bulimia Eating d/o that is self inflicted starvation Binge eating and purging Body wt , 15% IBW Higher incidence in caucasion girls in higher socioeconomic class. Antidepressants Wt gain at a teady rate 0.1-0.2 kg QD until desired wt is achieved Autism Autism is a developmental disorder that appears in the first 3 years of life, and affects the brain's normal development of social and communication skills. Behavior modification Consistent care schedules. Prognosis varies good if caught early. Many autistic children achieve independence by adulthood. Hyperactivity ADHD D/O with limited attention spans, overactive, easily distracted, excessive talking, difficulty following instructions. Modifying bx, setting limits, consistant routine, reward system, praise Ritalin, cylert, dexdrine stimulate concentration Suicide Suicide 3rd leading cause of death in adolescents Males complete suicide 75% more than females Males use lethal methods Females drug OD or slit wrists No Suicide contracts, chemical restraints- benadryl, mellaril, thorazine, ativan. Psychotherapy Child Hodgkin’s Treatment: radiation therapy chemo surgery High success in early diagnosis 75% success rate in advanced cases 90% success in early diagnosis Patent ductus arteriosus Failure of ductus arteriosus to close completely after birth Abnormal blood flow from aorta to pulmonary artery Left to right shunt Chf, endocarditis, tachypnea, retractions, hypoxemia, murmur Patent ductus Normallly closes 10-18 hours after birth Complications: chf, endocarditis, pulmonary vascular obstructive diseaselater in life, Management: diuretics, digoxin Surgery Ventral septal defect Abnormal opening in interventricular septum resulting in blood flow from left to right ventricle Heart failure, holosystolic murmur Diuretics for chf, digoxin Ventral septal defect Other treatments: Pulmonary artery banding Surgery- repair with a dacron patch Tetrology of fallot Pulmonary stenosis, ventral septal defect, right ventricular hypertrophy, overriding aorta Right to left shunt Severe cyanosis, poor growth, syncope, chronic hypoxemia, harsh murmur Tetrology Monitor for anemia, dehydration Blalock-taussing shunt.. Close ventral septal defect Redirects blood flow back into lungs and allows oxygenation Crates artificial connection between pulmonary artery and aorta Tetrology Repair overiding aorta Long term complications: heart block, ventricular arrhythmias, severe right ventricular dysfunction, sudden death Complications phrenic nerve injury Transportation of the great vessles Pulmonary artery arises from left ventricle and Aorta rises from right ventricle Venous blood returns to right side of heart from aorta without being oxygenated Transportation… Unoxygenated blood returns from the pulmonary system and returned to pulmonary artery to lungs Management: createing an atrial septal defect or surgery to correct the vessels to proper position Coarctation of the aorta Defect narrowing the lumen of the aorta Increased pressure to head and arms Lower pressure to body and legs Which is reverse of normal Coarctation Manifestations: bounding pulse in legs, heart failure, leg cramps with exertion Treat for chf, digoxin, diuretics, baloon dilation of aorta - graft replacement if narrowing extensive Iron deficiency anemia Most common blood disorder in infancy, early childhood Etiology: decreased iron in diet malabsorption syndrome, diarrhea Decreased rbc production or premature destruction of rbc Milk without iron Iron deficiency Patho: bone marrow produces rbc’s but hemoglobin is decreaed and ineffective to carry o2 Too little o2 increases work load of heart Manifestations: pallor, tired, tachycardia, irritability Iron therapy oral liquid given with straw or dropper vit c Iron deficiency Medication ferrous sulfate, ferrous gluconate, ferrous fumarate, fer-in-sol Iron rich foods liver, cream of wheat, dark green leafy vegetables, dried fruit, egg yolks give with vitamin c foods Sickle cell anemia Genetic disorder sickle hemoblobin Inherited autosomal recessive disease african american, mediterranean, middle east.. Life long disease Each parent has trait=50% change of each child carrying the trait Sickle cell 25% chance of each child without the trait, and 25% chance of each child having the disease Newborn screening cbc, Path: low oxygen causes shape to sickle and slump together Sickle cell Lifespan of cell reduced from 120 days to 12 days Manifestations: Pallor, jaundice, delayed growth, renal dysfunction crying when joint touched, fever, fatigue Sickle cell Eye, liver, kidney, lungs, skin affected Sickled cells cause occlusion of small vessles Usually not diagnosed until 6 months Sickle cell crisis Joint pain bone pain, fever, cough swelling of hands/feet, seizures tachycardia, pripism, pallor Iv fluids, pain management Antibiotics due to high infection rate, pneumoccal vaccine at 1,2,5 yr h influenza at 2 mos hepatitis b positive response to bone marrow transplant in some… Sickle cell crisis Complications: Spleen often removed as it is not functioning Septicemia cause of deat from 1-3 year olds highest period of mortality to infection Child is susceptible to infection Aplastic anemia Etiology: failure of cell generating ability of bone marrow All elements of blood are defective, not developed or absent Related to toxic chemicals, neoplastic disease of bone marrow Some antibiotics, radiation Aplastic anemia Tests: bone marrow aspiration Manifestations: severe anemia, thrombocytopenia, leukopenia Treatment: bone marrow replacement is treatment of choice Hodgkin’s disease Malignant lymphoma Highest in 15-19 year olds Manifestations: painless growth of lymph tissue in neck, weight loss, fever, night sweats Success depends on stage of disease Hiv Etiology: human immunodeficiency virus Transmission: breast milk, blood, urine, body fluid From mother to infant before or during birth via placenta Infant can be positive at birth and negative at 18 months Hiv Manifestations: failure to thrive, viral bacterial infection, pneumonia Kaposis sarcoma rare in adolescents Over 18 months diagnosed by elisa and western blot Hiv Management: Antiretroviral meds to prevent reproduction of virus Combination of medication due to drug resistance Monitor cd4 count Respiratory distress syndrome Hyaline membrane disease Patho: lack of surfactant in newborn making lungs difficult to inflate Alveoli collapse at end of expiration Respiratory distress Manifestations: nasal flaring, expiratory grunt, tachpnea, low body temperature Tests: abg Management: oxygen, pulmonary surfactant, respiratory support Bronchopulmonary dysplasia Patho: chronic pulmonary disorders associated with meconium aspiration Lung becomes thicker and necrosis of alveolar walls with o2 impaired…alveoli can collapse Bronchopulmonary dysplasia Manifestations: wheezing, nasal flaring, irritability, cyanosis Management: tpn, feed by lavage when infant able, mechanical ventilation, oxygen bronchodilators…. Laryngotracho bronchitis Croup common 3 mos to 3 yrs Patho: viral or bacterial as h influenza Manifestations: hoarsness, inspiratory stridor, tachypnea, nasal flaring, barking cough Larygotracheo bronchitis Tests: cbc, c&s of tracheal secretions, c&s of blood Management: cool mist, oxygen, epinephrine by aerosol, npo, iv fluids, antibiotics, fowlers position Epiglottal edema reduced after 24 hours Acute epiglottitis Definition: bacterial infection of epiglottis … in older child cause can beh influenzae Manifestations: epiglottis cherry red, can obstruct airway, drooling, respiratory distress treatment: Cool mist, iv fluids, antibiotics Acute bronchiolitis Patho: inflammation of bronchioles inflammation causing edema often to respiratory synctial virus Most in child under 2 yr Manifestations: tachypnea, rstractions, wheezing, fussy, Bronchiolitis Eating problems, fever Test: x-ray Treatment: high humidity, mist tent, oxygen , iv therapy, liquify secretions, corticosteroids Lasts 3-10 days Prognosis good Respiratory synctial virus Associated with bronchiolitis Rsv or respiratory synctial virus Causes an infection usually More infall and peaks in winter Tests: x-ray shows atelectasis, hyperinflation Respiratory synctial virus Nasal secretions positive for elisa and immunofluorescent antibody ifa Ribavirin has antiviral activity Respiratory isolation, good handwashing Prognosis good Pulmonary tuberculosis Etiology: mycobacterium tuberculosis Many strains resistant to medication Seen in young, old, those with hiv, immune suppressed Test: tb skin test, chest x-ray, cultures Tb Some children have no signs of disease Success dependent on: compliance to therapy and parent to give medication for as long as ordered Sudden infant death syndrome Etiology: unknown Child under 1 year peak age 2-4 months Most occur in sleep More during winter Sids Associated with: maternal smoking, premature birth, respiratory infections, prone position for sleep Prevention: Place infant on back or side to sleep Pharyngitis Inflammation of the pharynx Etiology: viral bacterial Common age 4-12yr Manifestations: low grade fever, malaise, anorexia, pharyngeal erythema, cough, hoarseness, rhinitis.. Pharyngitis Management:c&s of throat, cool liquids, saline gargles, warm compress to neck, tylenol Viral treated symptomatically Strep causes high fever, white exudate on posterior pharynx… Pneumonia Acute inflammation of pulmonary tissue Etiology: viral bacterial Often foreign body aspiration Manifestations: cough, wheeze, respiratory distress, anorexia, irritability Pneumonia Tests: cbc, c&s of blood, urine, and sputum Management: oxygen, chest physiotherapy, suction as needed, fluids, bronchodilator, antipyretic Prognosis good Cystic fibrosis Inherited disease autosomal recessive trait—both parents must have gene for child to be affected patho: Abnormal thick mucus obstructs organs producing resp, digestive, integumentary, and reproductive dysfunction Cystic fibrosis Stasis of secretions-bacterial growth-chronic infection-actelectasis and fibrosis-lung destruction Hypoxia-increased pulmonary resistance-right heart failure Pancrease ducts blocked-trypsin, amylase, lipase not secreted for digestion islets of langerhans can be decreased=insulin dependence Cystic fibrosis Sweat glands secrete excess sodium and chloride=chloride over 60meq/l In forearm Wheezing, bronchitis pneumonia, copious mucus with infections, hypoxia, crackles,steatorrhea Growth failure, corpulmonale, chf, clubbing of nailbeds Cystic fibrosis Tests: prenatal testing Sweat test, pancreatic enzymes Management: high calorie, high protein diet, High salt in diet Breathing exercises, blow bubbles Cystic fibrosis Pancreatic enzymes before meals, pulmonary therapy, postural drainage, immunization, nurtition, prevent exposure to persons with respiratory disease, emotional suppport Many live into adulthood with antibiotics Cleft lip cleft palate Patho: failure of medial nasal and maxillary process to join Unilateral or bilateral Feeding problems, gagging, choking, otitis media Surgical closure of cleft lip at 1-2 months cleft palate repaired before 1 year Cleft lip cleft palate Special feeding nipple with head of child elevated Burp frequently as child swallows air can feed by syringe Post surgery npo until anesthesia gone.. Rubber tip used with syringe to feed and clean mouth.. No pacifiers…clean mouth with water after feeding Gastroesophageal reflux Regurgitation of stomach contents into esophagus Begin within 1 week of birth Occurs immediately after infant lies down manifestations: Spitting up, pneumonia, anemia, hematemesis, growth and weight gain problems Gastroesophageal reflux Tests: barium swallow, bronchoscopy Management: feed upright, cereal added, antacids, head elevated surgery- nissen fundoplication Hypertrophic pyloric stenosis Etiology: unknown patho: congenital hypertrophied pyloric muscle that surrounds the valve between stomach and duodenum Manifestations: forceful vomiting– projectile noted at 4-6 weeks Vomiting shortly after eating, hunger, sunken fontanel, decreased urine, weight loss.. Pyloric stenosis Tests: ultrasound, barium swallow Management: ng to empty stomach, iv fluids, pyloromyotomy-release obstruction Pyloric stenosis.. Feed pedialyte in 4-6 hours then ½ strength formula or undiluted breast milk, advance formula as tol Complications: dehiscence, Obstruction Prognosis good Dehydration Number one killer of children world wide Causes: bacterial, viral, parasites, irritable bowel syndrome ….. patho: increased motility, loss of water, electrolytes Vomiting, diarrhea, pyloric stenosis, malabsorption Dehydration Fluid loss- isotonic fluid and eletroyte loss Etiology: burns, fever, diarrhea, malabsorption syndrome, cystic fibrosis….. Manifestations: 3-5% loss mild 6-9% loss moderate 15% or more severe Dehydration Manifestations: weight loss, decreased urine output, sunken fontanels, no tears, low bp, rapid respirations…. Weigh diapers and count, iv fluid, i&o, electrolytes, daily weight Fluids and electrolyte replacement Diarrhea gastroenteritis Etiology: bacterial, viral, parasites, salmonella.. Loss of water and electrolytes in stool Manifestations: large volume of stool, light in color greasy foul smelling sunken fontanels, rapid pulse Diarrhea Management: Npo, iv solution -- in 24 hours begin pedialyte, gatorade Antibiotics as needed brat diet=banana, rice cereal, applesauce, toast I&o, electrolytes, stool for c difficile, cbc, ova and parasites Intussecption Common cause of intestinal obstruction 3 mos to 6 yr Patho: telescoping of one part of the bowel into another part of the bowel often at distal ileum manifestations: Vomiting, lethargy, abd pain, currant jelly stools.. Intussecption Tests: Barium enema, rectal exam Barium enema can correct the problem or Bowel resection with end to end anstamosis Post surgery: npo, iv, vs, bowel sounds, oral feedings when peristalsis returns Hirschsprung’s disease Congenital aganglionosis or megacolon Absence of ganglion cells in rectum and in colon Patho: ganglions provide parasympathetic nerve action to colon Constipation, ribbonlike stool, poor weight gain Hirschsprung’s Management: stool softeners, enema, oral antbiotics, colostomy or ileostomy to rest the bowel and regain tone Later colostomy closure Fluid and electrolyte replacement, monitor: bowel sounds, vs, stools… Hernias Protrusion of a portion of an organ through a structural defect Complication: circulation to organ impaired Incarcerated=cannot be reduced Strangulated=circulation impaired Hernias Types: diaphragmatic=protrusion of stomach through part of diaphragm Hiatal=protrusion of stomach through esophageal opening in diaphragm Inguinal=protrusion of organ through inguinal ring Umbilical=protrusion of intestine through weak abd wall Hernias Manifestation: buldging sac Management: most have surgical repair Inguinal may have scrotal truss or surgical repair Urinary Define: Hypospadia=urethral opening along ventral surface of shaft Epispadia=urethralopening along dorsal surface of shaft Phimosis=narrowing of opening of foreskin Urinary.. Hydrocele=fluid in scrotal sac Cryptorchidism=failure of one or both testes to descend into scrotum Wilm’s tumor Nephroblastoma Most common renal or intrabdominal malignant tumor of childhood Peak age 2-3 yeaars Patho/etiology: most common in left kidney both hereditary and non hereditary origin Wilm;S Manifestations: Asymptomatic enlarging abdominal mass, abd pain, hematuria, fever, hypertension, weight loss, fatigue Metastasis: liver, lungs, lymph nodes, brain, bone Wilm’s Tests: x-ray, abdominal ultrasound, abdominal and chest ct, chemistry, biopsy Management: surgical resection 24-48 hours after diagnosis Radiation therapy, chemotherapy treatment ranges 6-15 months Wilm;S Post operative : monitor vs, renal output, bowel sounds,parents feelings regarding diagnosis, avoid contact sports, prompt treatment of geniturinary symptoms Hypothyroid Hypothyroid to decreased production of thyroid hormone By thyroid gland Patho: congenital or acquired Insufficient stimulation of gland or systemic resistance to hormone Hypothyroid Manifestations: Lethargy, poor appetite, dyspnea, hypothermia, delayed growth, dry skin, constipation, mental slowness Management: Thyroid hormone replacement Hyperthyroid Patho: autoimmune, unknown etiology Manifestations: nervousness, tremors, irritability, hypertension, tachycardia, Tachpnea, heat intolerance Tests: tsh, t3, t4, radioactive iodine uptake Hyperthyroid Management: Antithyroid medication: propylthioracil, tapazole… Subtotal thyroidectomy… Post-op: monitor breathing, bleeding, calcium levels, head elevated, trach tray at bedside Dysplasia of the hip Developmental abnormality of the femoral head, acetabulum or both associated with other problems Associated with first pregnancy, spina bifida, breech presentation Subluxation or incorrect position of the femoral head in acetabulum is the most common in infants Dysplasia of the hip Manifestations: click when hip moved thigh and gluteal folds are not even when infant prone Shorter femur on affected side Older child can have affected leg shorter or waddling gaint or limp Dysplasia of the hip Tests: sonography, x-ray Management: varies with severity of deformity Pavlik harness-for infants under 6 months to maintain hip in abduction and alignment Hip spica cast-infants 6-18 months Other: open reduction, osteotomy, arthroplasty Hip dysplasia Nursing: maintain position of hip joint, prevent complications, provide stimulation, involve parents in caring for child, neurovascular assessment of extremity, report erythema, tenderness, teach cast care… smooth edges of cast with tape Taipes Clubfoot Congenital deformity of foot and ankle unilateral/bilateral Cause: unknown Noted at birth may be related to environmental conditions, intrauterine position, restricted movement in uterus Talipes Special shoes, short leg cast Passive stretching exercises, corrective splints, brace Corrective shoes Management: neurovascular check on feet, check cast edges for rough edges… Septic arthritis Infection of a joint From bacteria or existing osteomylitis, bites from human, cat, dog, rat, tick.. Infection causes damage to synovial membrane, synovial fluid increases, pus breaks down cartilage=permanent damage Septic arthritis Infants= found in both girls and boys Adolescent=more in males Joints=hip, knee, shoulder, wrist, ankle Organisms: b streptococcus, gram negative enterics h influenza, staph aureus.. Septic arthritis Manifestations: pain, warmth, edema, redness of joint Fever, occurs rapidly and is an emergency Tests: x-ray, aspiration of joint, c&s of fluid, blood culture, cbc, elevated esr Septic arthritis Management: surgical aspiration and drainage of joint, iv therapy, iv antibiotics for 10-14 days, then oral antibiotics for 4 weeks Long term disability can develop Meningitis Definition: infection of meninges Most cases in children under 5 years Etiology: bacterial, viral, fungus, haemophilis influenza Meningitis Inflammation of meninges causes inflammation and thick exudate and wbc accumulation…cfs becomes occluded and brain becomes edematous Manifestations: fever, vomiting, photophobia, stiffness in neck when flexed Meningitis High pitched cry, kernig sign, brudzinski sign, poor feeding.. Cs fluid… cloudy Tests: c&s of spinal fluid, lumbar tap management: Iv fluid, antibiotics for 10 days, isolation, rest, vs, i&o, decrease stimuli Monitor for: seizure, pupil reaction, change in loc Encephalitis Definition: inflammation of brain and spinal cord Etiology: bacteria, viral, fungi, protozoa, spirochetes… Manifestations: malaise, fever, headache, dizziness, nuchal rigidity, nause, vomiting, ataxia, tremors, seizures, coma.. Encephalitis Tests: serology, csf culture Management: hospitalization, hydration, nutrition, vs, medication, i&o, neurological status Hydrocephalus Excess fluid in the cranial vault subarachnoid space or both Can obstruct the ventricle system Congenital or acquired—related to meningitis, tumor, hemorrhage Hydrocephalus Cfs fluid accumulates in cranium and brain is compressed creating increased intracranial pressure When hydrocephalus occurs before the fusion of cranial sutures, the skull becomes enlarged Hydrocephalus Manifestations: increased head circumference, bulging fontanel, poor feeding,sluggish, high pitched cry, depressed eyes with sun sign (sclera seen above iris) lethargy, slow pupil response to light Hydrocephalus Tests: head crcumfrance, mri, ct Management: reduce accumulation of fluid Ventriculoperitoneal shunt =from ventricle to peritoneal cavity to drain fluid from ventricle and place into body fliud Post op care: place on nonoperatiave side, small feedings… Hydrocephalus Place on side after feeding Observe for intracranial pressure, sheepskin under head Monitor vs, vomiting, swelling along shunt tract, dressing for glucose.. Cerebralspinal fluid makes a halo on gauze when glucose is present… Cerebral palsy Most common permanent disability in childhood Affects visual, intellectual, language, neurological, motor dysfunction etiology: Infection, maternal drug use, birth trauma, anoxia, anesthesia during labor, head trauma.. Cerebral palsy Manifestations: Delayed motor development, arching of back, hearing and/or vision impairment, poor feeding/sucking, hypertonic muscles, developmental disabilities… Cerebral palsy Management: botox for spacticity, baclofen.. Corrective orthotic equipment, braces, casts, wheelchair, protective headgear, wheeled scooters, walkers, Stretching exercises, special classes, encourage independence Seizures Definition: sudden, disorderly discharge of electrical impulses from neurons No known cause-idiopathic Some from trauma, tumors, toxins, poisons, fever Child most prone from birth to 2 years Seizures Management: prevent from injury, airway , id Reduce fever, eeg, medication as: dilantin, tegretol, depakote, cerebryx, phenobarbital Others: neurontin, lamicatal, felbatol Meyelomenigocele Spina bifida failure of neural tube to close Etiology: folic acid deficiency during pregnancy, malnutrition Manifestations: absence of sensory and motor function beyond the defect flaccid paralysis, bowel and bladder incontinence, clubfoot, subluxated hip.. Meyelomenigocele Tests: alpha-fetoprotein afp, ct Management: surgery to replace neural contents in the sac .. Vp shunt for hydrocephalus, surgery for hip and extremity deformities Preop: position on abd, cover sac with saline soaked gauze.. Meyelomenigocele Protect sac from feces/urine Post op: position on abd for 10-14 days, monitor vs, watch for bleeding or infection Long term concerns: motor movement, bladder and bowel control, urinary tract infection, pulmonary infections Neonatal abstinence syndrome Opiod withdrawl of infant Manifestations: irritability, feeding problems, sleep problems, tremors, seizures…can persist for 3-4 months Management: urine tested for substance, tightly swaddled, decrease light and stimuli,i&o, vs, pacifier referred to intervention program due to potential neurological deficits Neuroblastoma Malignant tumor of the cells that give rise to sympathetic ganglia Most in children under 2 years 70% have metastasis at diagnosis Manifestations: palpable, firm mass at midline of abdomen Neuroblastoma Anorexia, bowlel and bladder alteration, if in chest=dyspnea, dificulty swallowing,neck and face edema Tests: ct, bone scan, mri, abd ultrasound, bone marrow aspiration, biopsy, urine for catecholamines Neuroblastoma Management: surgery, radiation, chemotherapy The younger the diagnosis the bettter the survival rates Lead poisoning Most common preventable problem in children in us Lead poisoning=blood level over 10mg/dl Etiology: inhaled, ingested, lead-based paint, caulking chips, lead contaminated soil or dust Lead poisoning Manifestations: anemia, anorexia, learning disability, decreased attention span, hearing deficits, growth and development failure, pica Tests: x-ray of abdomen, x-ray of long bones, ua for proteinuria, keytonuria, glycosuria to kidney damage Lead poisoning Management: chelation therapy Prevent future exposure to lead High levels: lead encephalopathy Cognitive impairment, behavior changes seizures.. Diaper dermatitis Contact dermatitis often due to prolonged exposure to feces, urine, inadequate cleaning of diaper area Manifestations: erythematous papular lesion on buttock, labia, scrotum, inner thighs Diaper dermatitis Management: keep area clean and dry desitin, a&d ointment zinc oxide Expose area to air several times a day Atopic dermatitis Eczema Pruritic allergic response or allergy Family history of allergy, asthma, allergic rhinitis Cause unknown Atopic dermatitis Manifestations: erythema, vesicles, papules that ooze and crust on cheeks, scalp, trunk.. Affected skin dry and pruritis intense Tests: skin testing, history of allergy Atopic dermatitis Management: hydration of skin, decrease inflammation, prevent infection Tepid bath, lotion, topical steroid cream, oral antihistamines,burow’s solution, corstarch added to bath, neutrogena soap.. Seborrheic dermatitis Cradle cap Chronic inflammatory reaction of skin in infancy etiology: unknown Manifestation: scalp thick, white, yellow, crusty, scaly patches, mild pruritis Seborrheic dermatitis Management: patches removed by mineral oil and shampoo daily Hair brush with soft brush antiseborrheic shampoo or topical corticosteroids can be used Psoriasis Proliferation os skin disorder Manifestations: thick, scaly patches and inflammation Remission and exacerbations Humifiers help in winter Candidiasis Thrush etiology: candidia albicans Etiology: contaminated nipples, pacifiers, hands Manifestations: white or whitish yellow lesions in infected area..Mouth, gi tract.. Management: nystatin oral or cream Fluconazole…. Otitis media Common in age 2-6 year after upper resp infection Manifectations: fever, rhinitis, irritability, pulling rubbing affected ear.. Management: antibiotics for 10 days ..Tympanostomy tubes can be in place 6 months before being spontaneously rejected Refractory errors Light rays bent and fall infront or behind retina Myopia-nearsighted Hyperopia-farsighted Management: corrective lenses and screening Strabismus Lack of coordination in extraocular muscle results in cross eyed appearance Congenital or paralysis of muscle Manifestations: squinting, tilt head to block out image, closing one eye Strabismus Management: patching the stronger eye a few hours a day Surgical correction If untreated: amblyopia can develop if untreated Preorbital cellulitis Inflammation of eyelid and periorbital area Manifestations: pain, tendrness, fever, erythema, headache, purulent nasal drainage Management: iv antibiotics, antipyretics, analgesics