Slide 1
advertisement

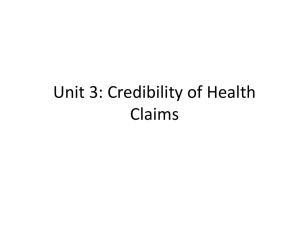
Theoretical, ethical, contextual, practical and critical foundations for future epidemiology Raj Bhopal, Bruce and John Usher Professor of Public Health, Public Health Sciences Section, Division of Community Health Sciences, University of Edinburgh, Edinburgh EH89AG Raj.Bhopal@ed.ac.uk Educational objectives On completion of your studies you should understand that Theory, method and application are interrelated. Epidemiology serves the community in a number of ways, but predominantly through its role as one of the underpinning sciences of public health and medicine. Ongoing vigorous debate on the future of epidemiology probably heralds a paradigm shift. Epidemiology is both broadening and specialising. The context in which epidemiology is learned and practised is important in determining its nature. The interrelationship of theory, methods and application: a question of values Epidemiology has entered the 21st century with both its exponents and critics questioning its foundations, record and future. Epidemiology has been accused of: being atheoretical; divorced from its source of problems, theories and applications (public health); the source of spurious, confusing and misleading findings; over-dependent on the ‘black box’ risk factor approach; and irrelevant in resolving some major problems, e.g. the growing consumption of illegal drugs, the rising prevalence of smoking in developing countries and health inequalities. Underlying philosophy of epidemiology The philosophy and theory underpinning epidemiology, as in most other disciplines, is seldom explicit. Philosophically, epidemiology takes a positivist stance. Problems can be solved through data which are usually, but not always, quantitative. However, advances may follow inspiration and insights that are not based on quantitative data. Future epidemiology is likely to involve closer ties between qualitative and quantitative approaches. The fundamental epidemiological question is why differences in disease prevalence and Exercise: fundamental influences on health List 5 or 6 broad and fundamental influences on health and disease, i.e. those influences that change the population patterns of disease. Fundamental influences generating disease patterns Changes in the physical, chemical and radiation environment. Genetic evolution of microbes, animals and humans. interaction between humans, microbes and animals. Human social and economic circumstances Cultures and behaviours. Human inventions and discoveries Figure 10.1 Natural environmental change Human interventions, discoveries and manipulations of the environment Changes leading to altered interaction between microbes, animals, and plants Social change in human populations - in material circumstances, and behavior Influence on individuals and families - varies by place Genetic changes in microbes, plants, animals and humans The phenomena underlying population variations Over time population differences host, agent or environment factors Population variations in health and disease patterns Demonstrate population differences in disease rates by time, place and person/population Analysis and interpretation of differences to gain insight into the evolution of these patterns, and hence the causes Use information to improve health Epidemiology tries to understand above phenomena Uses of epidemiology Morris, in his classic book, “Uses of Epidemiology” published in 1957, portrayed epidemiology as a discipline with multiple applications. In most contemporary textbooks, by comparison, the vision of epidemiology is narrower, and probably narrowing. Question under current debate is whether epidemiology is primarily an applied discipline or primarily a science where methods, technique and theory dominate. I think it is an applied discipline where methods, technique and theory are very important Interdependence of application, theory and methods To illustrate how theory, method application are interdependent I have chosen two topics of personal interest: setting priorities in health care and assessing the impact on health of local polluting industries. Setting priorities in health and health care Priority setting within health and health care mixes science and politics. Epidemiological data on disease frequency, patterns, causes, risk factors and effectiveness can feed the debate Theories on causation, and predictions of the changing size of the problem, are central to prioritising. Understanding of causation is complementary to descriptive data on the burden of disease. Needs of policy and practice have provided the stimulus for modes of analysis (PYLL, attributable risk, NNT etc) that are not essential to causal epidemiology. Teesside study of environment and health Heavy industry is vital but there is a price to pay - pollution. Industries are facing complaints, adverse publicity, litigation and public inquiries. Our study of the impact of petrochemical and steel industries on the health of people in Teeside typifies applied public health. Teesside study of environment and health First step was for us to devise the theoretical framework within which the problem is to be resolved. Positivist approach based on hypotheses, epidemiological study design, data collection and an understanding on how the data would be interpreted. If a disease or health problem was causally related to living close to industry, then there would be a gradient with distance of residence, those closest having the highest rates, those furthest the lowest. Teesside study of environment and health Underlying theory of health and disease was that long-term exposure to low levels of industrial air pollution does harm, rather than good. Causal thinking was based on the epidemiological criteria (guidelines) for causality. Outwardly atheoretical, pragmatic, public health orientated projects may be founded on important epidemiological theories and concepts. Readers who do not share these theories and concepts, and who are either not familiar with or confident about the methods, will not be comfortable with the results. However, these were not made explicit at all before, during or after publication of the Teesside study, but after much reflection. Four components of a paradigm, or a disciplinary matrix as identified by Kuhn Symbolic generalisations e.g. The laws of physics as given in mathematical formulae. Beliefs in particular models e.g. heat as a kinetic energy. Values e.g. the key goal of science being accurate predictions. Exemplars i.e. classic examples of problems and their solutions, upon which Kuhn places especial emphasis. Paradigms: the evolution of epidemiology In this essay, ‘normal science’ means research firmly based upon one or more past scientific achievements, achievements that some particular scientific community acknowledges for a time as supplying the foundation for its further practice. Thomas Kuhn. The Structure of Scientific Revolutions In 1996 Susser and Susser called for a paradigm shift in epidemiology. To call for a new paradigm is a severe provocation for it declares the current paradigm inadequate. Vigorous debate and resistance to change are identified by Kuhn as precursors to change. Four paradigms in epidemiology identified by the Sussers Exploratory description of disease (e.g. Graunt's analysis of the London Bills of Mortality in 1662: and Ramazzini and occupational exposures, 1700). In this period there was a change from sickness being seen as a result of disease entities not as humoral imbalance. Miasma theory of disease - the idea that disease arose from foul emanations from pollution (18th Century). Germ theory of disease (19th Century). Multiple causes as captured in the black box metaphor (20th Century). Exercise: waning of diseases Reflect on the diseases that contemporary doctors either do not, or extremely rarely, see. Now, reflect on diseases that may not be seen by doctors in 100 years time. Waning of diseases Physicians in 100 years time may not see mesothelioma (a cancer resulting from asbestos), tuberculosis, polio, measles, guinea worm. stroke and heart disease. AIDS How has epidemiology adapted to cope with such changes? Scope of epidemiology and specialisation Epidemiology has broadened and specialised Subdivisions of epidemiology Infectious disease epidemiology Chronic disease epidemiology Health care epidemiology Public health epidemiology Social epidemiology Clinical epidemiology Genetic epidemiology The benefits are those of all forms of specialisation. Costs of specialisation are fragmentation of the discipline. The scope for specialisation is reliant upon context The context of epidemiological practice in the USA and UK The vision of public health problems has become more scientific with issues of theory, measurement and method receiving close attention, so academic and service public health goals have diverged. U.S. School of Public Health environment is large enough to offer a career path within this system for professional researchers. Professional epidemiologists set up and sustain organisations such as the Society for Epidemiological Research and the American College of Epidemiology. Question for epidemiologists in such settings is this - what is the role of epidemiology in such partnerships for public health? The context of epidemiological practice in the USA and UK Epidemiologists in Britain, perceive themselves first as statisticians, physicians, public health specialists or social scientists. Work in multidisciplinary departments. Question for epidemiologists working in such settings is - what is the role of epidemiology in the world of science, and how is theoretical and methodological work to be nurtured? The practice of epidemiology in public health Epidemiology is a key science that underpins public health and increasingly clinical practice too. Epidemiological textbooks usually proclaim the applications of epidemiology, as the foundation science of public health, but most focus on design and methods for causal research. A role as an applied science imposes on epidemiology the need for a code of ethics and good conduct. Ethical basis and proper conduct of epidemiology: the need for a code Three issues of interest to me. Manipulation of scientists by the tobacco industry. Manipulation of authorship. Research on ethnicity and race. Tobacco and health Industry has manipulated research into tobacco and health. Fostering controversy. Countering authoritative review articles through an international network of paid scientific ‘consultants’. Concealed or distorted evidence from its own research showing the addictive and harmful nature of smoking. Epidemiologists need to be armed with an ethnical code to guide them in making the right decisions. Authorship Authorship of scientific papers is increasingly important. View that only work that has passed the scrutiny of peers is reliable and trustworthy (a concept itself worthy of scrutiny). Key factor in promotion. Academic appointment. Service appointments, promotion and distinction awards. Winning research grants. Finances coming into Universities. Tempting individuals to accept authorship on papers to which they have not contributed sufficiently. Allocation of authorship is complex and raises ethical issues central to scientific integrity. The International Committee of Medical Journal Editors' criteria for authorship An “author” is generally considered to be someone who has made substantive intellectual contributions to a published study, and biomedical authorship continues to have important academic, social, and financial implications Authorship credit should be based on 1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data; 2) drafting the article or revising it critically for important intellectual content; and 3) final approval of the version to be published. Authors should meet conditions 1, 2, and 3. Ethnicity and race Ethnicity and race are among the top five or so most important variables in epidemiology. Hippocrates contrasted the feebleness of the Asiatic races to the hardiness of the Europeans. Concept of race was of human groups shaped by their ancestry in different environments especially climate. Idea of races as distinct species, which was long and seriously debated, gave way to races as biological subspecies. Differences among races were usually assumed to be biological, interpreted to show superiority of white races and used to justify policies which subordinated “coloured” groups. A perception of inferiority in relation to health can be fostered by research focusing on problems more common in minority ethnic groups, and, by Ethnicity and race When research implies genetic factors rather than environmental ones ethnic minority groups may be perceived as biologically weaker. Science that indicated such weakness helped justify slavery, social inequality, eugenics, immigration control, and racist practice of medicine. Studies of ethnic and racial variations in disease pose a challenge to the maintenance of high ethical standards in epidemiology. Racial prejudice is fuelled by research portraying ethnic minorities as different, usually inferior to the majority. Race and ethnicity are epidemiological variables that show the importance of historical, political and social awareness among epidemiologists. Ethical guidelines In 1998, the International Epidemiology Association’s European Group published a code of practice for epidemiologists which states that epidemiologists should: Seek the truth in good faith without doing harm or jeopardising personal integrity. Judge their own work and ideas and those of colleagues in an impartial manner. Disclose conflicts of interest to ethical review committees. Publicly acknowledge all research sponsorship. Publish all research with scientific merit. Refuse requests to withhold findings, change or tone down the content of reports, or delay publication unreasonably. Critical appraisal in epidemiology: separating fact from error and fallacy Critical appraisal is important because much of what we know as the truth is wrong sometimes dangerously so. Reflect on some medical and public health activities which were widely practised but are now known to be wrong, some dangerously so. Your reflection should include both historical activities, say, before the turn of the twentieth century and more recent ones. Now, reflect on some current policies and practices that may meet the same fate. Critical appraisal: follies and fallacies in medicine Critical appraisal is the use of the ‘scalpel of scepticism’ to extract truth from error in research. Petr Skrabanek and James McCormick’s book Follies and Fallacies in Medicine is a gold mine of examples. The fallacy of association being causal The Weight of Evidence Fallacy The fallacy of repeated citation Fallacy of Authority Fallacy of Simple Explanation The Fallacy of Risk The Fallacy of Inappropriate Extrapolation The Fallacy of Significance Tests The Fallacy of Obfuscation Fallacy of Covert Bias The nature of critical appraisal Critical appraisal is not just about criticism. As in a book, film or theatre review you assess how good the work is in relation to expectations and what has gone before. Austin Bradford Hill posed four simple questions to guide the reading of scientific papers: - Why did the authors start? - What did they do? - What did they find? - What does it mean? Critical appraisal: epidemiological questions The questions below can help to produce a critical appraisal specific to epidemiological research. Is an epidemiological approach appropriate to the problem under study? What alternative methods would also help resolve the problem? What is the study design and is it suitable for the problem addressed? Are the dates on which the sampling frame was compiled given? Is the date or time period over which data were collected given? Critical appraisal: epidemiological questions Have terms/labels used to describe populations or sub-populations been defined and justified? Is the study sample representative of a larger population, and hence, are the results likely to be more widely generalisable? Are the sampling and measurement methods equivalent in the groups to be compared? Are compared populations or subgroups similar on key variables? If not, are the differences sufficiently small to permit adjustment using a weighting technique such as age standardisation, or other statistical techniques such as logistic regression? Continuing education: role of historical landmarks Role of the classics, or in Kuhn’s terminology, exemplars for contemporary work. Lind investigated scurvy and reported his findings in 1753 The story of the prevention of scurvy by eating citrus fruits shows (a) that putting research into practice is a long-term endeavour. (b) mechanistic understanding, though valuable, is not crucial to put epidemiology into public health practice The story of Edward Jenner’s vaccination against smallpox shows the need to (a) listen to the public with an open mind (b) test a hypothesis with experiment (c) those making a discovery need to be champions of its dissemination and implementation. Continuing education: role of historical landmarks-John Snow Classic investigation by John Snow of cholera also illustrates important principles. Miasma theory was favoured. Snow studied what he described as ‘the most terrible outbreak of cholera which ever occurred in this kingdom’- the epidemic of cholera in Broad Street, Soho (1854). Suspected some contamination of the water in the Broad Street pump. The dead lived or worked near the pump. Nearby workhouse and brewery had their own water supply and little cholera. People living far away but drinking Broad Street pump water were afflicted. Continuing education: role of historical landmarks-John Snow Water, not miasma in the air, he concluded, is the source of the morbid matter that causes cholera. He published in 1849 and 1855, and gave evidence to many learned committees. Was unable to convince those in power and died in 1858 before his ideas were accepted. Snow’s book cost him two hundred pounds to publish and he sold 56 copies in three years, making three pounds, 12 shillings. Reflection on the future of epidemiology In industrialised countries the challenges for epidemiology will, increasingly, lie in the prevention and control of the diseases of older people. Solutions to these problems of old age may lie in improving maternal, foetal and infant health. Relative poverty in early life, and wealth in later life, may be the basis of maladaptation, triggering diseases such as coronary heart disease and diabetes. In many developing countries problems of poverty (inadequate sanitation, inadequate nutrition and communicable disease) are combining with those of the post-industrial era (cancer, heart disease, stroke and road traffic accidents). Reflection on the future of epidemiology Economic and health inequalities will hold centre stage in public health The injustice of gross waste in some countries, and horrendous poverty in others will be increasingly unacceptable. Epidemiology and Public Health will face ethical and a technical challenges. One key question facing epidemiology is whether it should be an advocate for eradication of public health problems or a dispassionate contributor of science. Epidemiology will need to provide insights into complex mechanisms e.g. those by which wealth and health interact. Reflection on the future of epidemiology Human genome mapping project will re-ignite the question of the relative importance of genetic and environmental factors even although the environment-gene interaction is all-important Some principles will help to guide epidemiologists in the coming whirlwind of research The genetic pool changes slowly and genetic variations between populations are small The environment changes rapidly, and differs greatly from place to place. Occurrence of most common diseases shows massive geographical and time period variation Changes point to the dominance of environmental causes. Reflection on the future of epidemiology Genetic factors provide the stage in the great drama of disease causation, but the environment is the leading player. advances in genetics will undoubtedly impact on the diagnosis and management of disease in the future epidemiologists will need to be trained in genetics. Reflection on the future of epidemiology Molecular science will deepen understanding. Yet, the public health dividend will come from altering the pattern of risk factors in the whole population. Not simply biochemistry that determines an individual and population’s serum cholesterol level but how food is grown, processed, purchased, cooked and eaten. Behaviours, including dietary ones, are not just personal taste, but affected by, Trade agreements, agricultural policy, marketing, economic subsidy as determinants of costs, availability and consumption. Reflection on the future of epidemiology Epidemiologists will need to work harder to understand how diseases are generated through the interactions that people make when living in groups. How societies work and can be changed to promote health. Development of such understanding will come faster and better in multidisciplinary environments. Epidemiology will become a vital area of knowledge for all clinical and public health researchers and practitioners. Epidemiology will help them envision the causes of ill-health and to develop coherent policies, laws, and health care systems to generate health from the pattern of disease. Summary Theory underpinning epidemiology is seldom made explicit. Epidemiology takes a positivist stance. The basic theory is that systematic variations are a product of differences in the prevalence of, or susceptibility to, the causal factors. Epidemiological methods quantify variations in disease patterns and their causes, to establish associations, and to test resultant hypotheses on causes. A vigorous ongoing debate on the future of epidemiology indicates that major changes are coming. Summary Rise of genetic epidemiology. Social epidemiology. Epidemiology as a prime force in public health. Need for a code of ethics. Critical evaluation of research as a crucial skill. Attention both to technical excellence of epidemiology, and to its value in the historical, political, social, and geographical context. Epidemiologists to have an understanding of the wide determinants of health and disease. Achieved by broad studies of the history and achievement of the key disciplines contributing to epidemiology. Keen interest in contemporary debates and future trends.