Measurement for improvement
advertisement

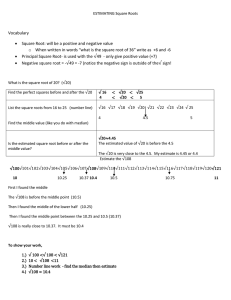
Using Data for Decision Making in Health Care “Plot the dots.” Greg Ogrinc, MD, MS Dartmouth Medical School 27 June 2009 1 Objectives Investigate how healthcare systems are measured and the effect of this measurement Identify how understanding and measuring variation is integral to the model for improvement Apply the rules of analysis for evaluating data over time from a system 2 Agenda Storytime! P4P (10 min) with buzzgroups and discussion (10 min) Evidence, improvement, and measurement (30 min) Data, group work, and discussion Introduction to variation and data over time (time ordered data) (40 min) Data, group work, and discussion 3 Storytime… 4 Percent Normotensive (<140/<90) (Avg=74.39, UCL=83.66, LCL=65.11 for subgroups Jun-07-May-08) 100% 90% 80% UCL Target Avg % patients with normal BP 70% 60% LCL 50% 40% 30% 20% 10% 0% May-05 Jun-05 Jul-05 Aug-05 Nov-05 Jan-06 May-06 Jul-06 Sep-06 Oct-06 Date Jan-07 Mar-07 Jun-07 Jul-07 Sep-07 Nov-07 Jan-08 Mar-08 May-08 5 HTN letter High blood pressure can lead to heart disease and stroke if not well controlled. We review the risks and benefits of changing their blood pressure treatment regimen on a regular basis. Checks of your Blood Pressure show that it is higher than 140/90, so we need to get this under better control to reduce your risk of heart disease and stroke. You can do the following things to help keep your blood pressure under control: - Reach or maintain a normal body weight - Eat a healthy diet without too much salt. - Eat plenty of fruits and vegetables - Limit the amount of caffeine - Include regular physical activity in your schedule - Do not drink more then 2 ounces of liquor or 2 glasses of beer or wine in one day. 6 HTN letter In order to help you get better control of your blood pressure, I recommend the following: (1) Discontinue HYDROCHLOROTHIAZIDE. (2) Start CHLORTHALIDONE 100MG each morning. I have made the changes in the computer and the meds will be mailed to you. (3) Please come to the WHITE MOUNTAIN FIRM for a blood pressure check in 2 weeks. You do not need an appointment. (4) Stop by the laboratory for blood work on the same day you come for the blood pressure check. 7 P4P in NHS Doran et al, NEJM, 2006 Evaluated first year of P4P for >8000 family practices in England Measured proportion of patients eligible for whom the indicator was met Diabetes – % blood pressure <145/<85 Hypothyroid – % blood check within 15 mos Stroke – % cholesterol < 193 Able to request exceptions for some patients 8 9 P4P in NHS Doran et al, NEJM, 2006 Median Level level of achievement was 83% of achievement was affected by Age and socioeconomic of patients Size of practice, # patients per practitioner, age of practitioner, whether practitioner was trained in the UK Exception reporting (1% increase in exception reporting increased achievement by 0.6%) Small number of practices achieved high scores by excluding large number of patients More common in small practices 10 Buzz Groups Turn to the person next to you Use the stories you just heard as well as your knowledge about pay for performance (P4P) – news, articles, journals, internet. 1. What are the benefits of this approach to improving quality? 2. What might be some drawbacks to this approach? 11 Evidence-based Improvement Generalizable Scientific Evidence + Particular Patient Measured Performance Improvement Batalden, 2003 12 Evidence-based Improvement Generalizable Scientific Evidence + Particular Context Measured Performance Improvement Batalden, 2003 13 Evidence-based Improvement executing locally choosing best plan Generalizable Scientific evidence • control for context • generalize across contexts • experimental design • statistics + Particular Context • understand system “particularities” • learn structures, processes, patterns • culture and context of changes Measured Performance Improvement • balanced measures • clinical • functional • satisfaction • costs 142003 Batalden, Individual Patient Care versus Systems of Care Individual patient Initial work-up History, physical exam, chart review Further work- Labs, xrays, up ultrasound, functional tests Therapy Surgery, medications, watchful waiting System Your experience within system, discuss with others Process & causeeffect diagrams, outcomes data model for improvement, PDSA, root cause analysis 15 “quality improvement” The combined and unceasing efforts of everyone – health care professionals, patients and their families, researchers, administrators, payers, planners, educators – to make changes that will lead to better patient outcome, better system performance, and better professional development. Batalden and Davidoff, QSHC, 2007 16 Better patient (population) outcome Better professional development Everyone Better system performance 17 Batalden and Davidoff, QSHC, 2007 Better patient (population) outcome Better professional development Everyone Better system performance 18 Batalden and Davidoff, QSHC, 2007 Competence? Accreditation / certification / licensure? Faculty / curricula development? Professional school admission / selection? Interprofessional cooperation? Joy / creativity / pride? Measures? Patient knowledge? Variation? Causes? Better patient / Hiring / orientation? population outcome Supervision? Accountability? Participation / commitment? Recognition / reward? Better professional development Linking / leadership? Org. development? Governance? Financing? Everyone Better system performance Measures? Options / methods? Reliability / failure? What Standards? Linking / leadership / supervisory development? Leadership performance review? theRecognition / reward? might be foci of inquiry? 20 A Model for Improvement What are we trying to accomplish? How will we know that a change is an improvement? What change can we make that will result in improvement? ACT PLAN STUDY DO Langley et al. , The Improvement Guide, 1996 21 Assumptions about Measurement for QI Measurement has become “popular” and arises in many venues (e.g., P4P, country comparisons, etc) Measurement and measures fit into the model for improvement Part of the cycle Necessary element Understanding the measures means understanding the level of the system to which the measures relate How you display and data can have a significant effect on how it is interpreted and used Know how the measures relate to the system 22 What are the Challenges of Measurement? Time consuming/added work. Threatening, especially when it is used against you. Making sure the data are accurate and consistent. Too many indicators; not the appropriate indicators. Using the data you collect to actually take action. Manual versus automated data collection systems. Results don’t match management’s view of reality. The indicators were given to me by my manager and I had no input. Ownership of the data collection process and the results. Lack of training in data collection methods and analysis. 23 23 What are the Benefits of Measurement? Helps you make decisions; build confidence. Allows you to keep tabs on what is going on. Sets the stage for improvement/identifies problem areas. Provides a common frame of reference for staff and management. Identify patterns and trends in the data. See how well performance matches our goals. Helps us focus on what is important. Helps you “sell” your ideas to management. Understand interrelationships between departments and units. Moves you away from anecdotes and one person’s view. 24 24 The Quality Measurement Journey AIM (Why are you measuring?) Concept Measure Operational Definitions Data Collection Plan Data Collection Analysis ACTION Source: Lloyd, R. Quality Health Care. Jones and Bartlett Publishers, Inc., 2004: 62-64. 25 25 The Quality Measurement Journey AIM – freedom from harm for hospitalized patients Concept – reduce patient falls Measure – falls rate (falls per 1000 patient days) Operational Definitions - # falls/inpatient days Data Collection Plan – monthly; no sampling; all IP units Data Collection – unit submits data to RM; RM assembles and send to QM for analysis Tests of Change Analysis – control chart 26 26 Relating the Three Faces of Performance Measurement to your work Not mutually exclusive silos All three areas must be understood as a system – interdependent. Individuals need to build skills in all three areas. Organizations need translators who are able to speak the language of each approach. Individuals often identify with one of these approaches and dismiss the value of the other two. 27 27 Primer on Heart Attacks Often called “MI” or “AMI” Symptoms include chest pain or pressure, shortness of breath, sweating, nausea and may come on with exertion Individuals often have specific risk factors (genetics, smoking, diabetes, high blood pressure or cholesterol…) Treatment aimed at opening up blocked artery to restore blood flow to part of the heart and reducing the work the heart has to do Treatments may include Catheter with stent to open artery or medication to dissolve clot Meds to thin blood (reduce chance new clot will form) like aspirin and others Meds to reduce the work of the heart like beta-blockers and28 ACE inhibitors What Happens to People Having Heart Attacks? Patient Symptoms Emergency System Emergency Department Cardiac Care Unit Where should we give aspirin? 29 Opportunities To Give Aspirin Aspirin Aspirin Aspirin Aspirin Patient Symptoms Emergency System Emergency Department Cardiac Care Unit •Take when calls •Family education •Before symptoms start •EMT gives •MD orders by radio •MD orders •Nurse protocol •Pre-print admit orders 30 31 Dartmouth Atlas CMS Technical Process Quality Measures Scores (0-100; low–hi) Hospital Composite AMI CHF Pneumonia California Pacific Med Ctr 85.5 92.8 93.5 72.3 Hartford Hospital 80.1 90.2 84.0 60.7 BIDMC 92.5 96.4 94.5 86.5 Catholic Med Ctr 93.2 98.8 93.0 86.3 DHMC 88.3 96.0 88.5 78.5 Fletcher Allen 85.7 92.0 84.5 78.5 Medicare claims data, 2005 32 Dartmouth Atlas CMS Technical Process Quality Measures Scores (0-100; low–hi) State Composite AMI CHF Pneumonia California 85.4 92.3 88.1 73.5 Connecticut 88.6 92.7 88.6 81.6 Massachusetts 89.2 94.7 89.2 80.0 New Hampshire 90.7 95.3 90.8 83.1 Vermont 87.9 91.3 84.3 84.5 Medicare claims data, 2005 33 Group Work, Part 1 Review the data table from the first hand-out Discuss the questions in your group Be prepared to discuss in the large group setting 34 “If I had to reduce my message for management to just a few words, I’d say it all had to do with reducing variation.” W. Edwards Deming 35 35 If you don’t understand the variation that lives in your data, you will be tempted to ... Deny the data (It doesn’t fit my view of reality!) See trends where there are no trends Try to explain natural variation as special events Blame and give credit to people for things over which they have no control Distort the process that produced the data Kill the messenger! 36 Demonstrating Variation: Example #1 The figure below shows how two individuals, Mary and Bill, placed ten shots on a target. Which individual is the better shot? Mary 37 Bill 37 Demonstrating Variation: Example #1 • Mary shots are clustered • Bill hit the bulls eye, but his pattern is erratic • Mary merely has to adjust her sights down and to the left. Then, her shots should all cluster near the center of the target. • People take the most current data point and assume that this represents the process's performance • If you are really sincere about understanding where your processes have been, where they are now, and where they can be in the future, you must become knowledgeable about the types of variation and how to depict them. 38 Mary Bill 38 Demonstrating Variation: Example #2 Using whatever method you have for telling time (watch, phone, Blackberry, PC, position of the sun, etc.) record the exact time right now and decide what time it is at your table! 39 39 The Problem Aggregated data presented in tabular formats or with summary statistics will not help you measure the impact of process improvement/redesign efforts. Aggregated data leads to judgment, not to improvement. 40 40 Types of Variation Common Cause Variation Is inherent in the design of the process Is due to regular, natural or ordinary causes Affects all the outcomes of a process Results in a “stable” process that is predictable Also known as random or unassignable variation Special Cause Variation Is due to irregular or unnatural causes that are not inherent in the design of the process Affect some, but not necessarily all aspects of the process Results in an “unstable” process that is not predictable Also known as non-random or assignable variation 41 Key Point … Common Cause does NOT mean “Good Variation.” • It only means that the process is stable and predictable. • If a patient’s systolic blood pressure averaged around 165 and was usually between 160 and 170 mmHg, this might be stable and predictable but completely unacceptable. Special Cause variation does NOT mean “Bad Variation” • A special cause may represent a very good result (e.g., a low turnaround time), which you would want to emulate. •Special Cause merely means that the process is unstable and unpredictable. 42 Balancing under and over acting to minimize net loss Action taken Action not taken Action needed X loss Action not needed loss X 43 Measure Elements of a Run Chart Time ordered observations The centerline (CL) on a Run Chart is the Median X (CL) Four simple tests are used to determine if special cause variation is present 44 Elements of a statistical process control (SPC) chart Natural Process Limits Mean Measured value (“x”) Time-ordered observations (1 n) 45 Tests to Identify Special Causes on a Run Chart Test #1: Too few or too many runs Test #2: A shift in the process 7 data points on one side of the median Test #3: A trend 7 data points constantly going up or down depending on how many data points you have on the chart) Test #4: A saw toothed pattern 46 Total data points = 29 Run Chart: Medical Waste Data points on the Median = 2 Number of “useful observations” = 27 6.00 The number of runs = 14 5.75 5.50 Pounds of Red Bag Waste 5.25 5.00 4.75 Median=4.610 4.50 4.25 4.00 Points on the Median (don’t count these as “useful observations”) 3.75 3.50 3.25 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 Point Number 47 Does this chart allow us to understand variation? 48 How about this one? 49 Is this one any better? Isn’t this a downward trend? 50 This must surely be an upward trend! 51 Maybe this one is a better chart? If so, why? Is this the Median? 52 Chronic Obstructive Pulmonary Disease Run Chart COPD Length of Stay 1. Find the Median 2. Determine the “useful observations” 3. Apply the run test rules spell los 14.0 12.0 8.0 6.0 4.0 33 data points with 2 on the median 2.0 We have 31 useful observations de c oc t au g ju n 04 Ap r- fe b de c oc t au g ju n 03 Ap r- fe b de c oc t au g ju n 02 0.0 Ap r- Days 10.0 Month 53 Chronic Obstructive Pulmonary Disease Run Chart COPD Length of Stay 1. Find the Median 2. Determine the “useful observations” 3. Apply the run test rules spell los 14.0 12.0 8.0 6.0 4.0 12 runs (should be between 11 and 21 runs) 2.0 de c oc t au g 04 Ap r- fe b de c oc t au g ju n 03 Ap r- fe b de c oc t au g ju n 02 Are there 7 data points constantly increasing (trend)? ju n Are there more than 8 points in a run above or below the median (shift) ? 0.0 Ap r- Days 10.0 Month 54 Group Work, Part 2 Review the run charts on the hand-out Discuss the questions in your group Be prepared to discuss in the large group setting 55 56 57 58 Summary How measures are used have a strong influence on the care that is delivered (P4P) To be most effective, the measures must be clearly connected to an aim/goal, the process, and changes that are tried Measuring data over time (and using run charts or statistical process control charts) creates useful measurement that provides insight into the process Measurement for improvement and decision-making, not just for judgment and research 59