NEUROPSYCHOLOGY
Brain Structure, Function and
Cerebral Dominance
Dr. Malcolm Hughes
Within the areas of study that constitute neuro-psychology, the
understanding of the brain and its constituent parts have led to
substantial contributions to the relationship between brain and
behaviour.
Included among these areas are the physiological mechanisms associated
with the central nervous system.
An overall understanding of the anatomy of the brain structure
reflects the diversity of the individual’s mental processes and
behaviour. Some structures can highlight these effects quite
significantly.
As well as understanding the functions of the brain, it is
important to recognise that the two sides of the brain are not
identical to each other, as research into “lateralisation” of brain
function and the “split-brain” effects will demonstrate
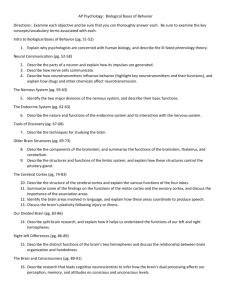
Midline structure of the human brain
Detailed part cross section of the brain stem
Compartmentalisation of the Human Brain
The brain, (as distinct from the spinal cord), consists of three major
divisions:
The Hindbrain – the most posterior part of the brain
The Midbrain – proportionally the smallest part
The Forebrain – the most prominent part of the brain
The Hindbrain:
Consists of three structures – the medulla, the pons and the
cerebellum.
The medulla, pons, midbrain and the central parts of the forebrain
constitute the brain stem.
The Medulla:
Situated just above the spinal cord (almost and extension of that
structure) and controls a number of vital reflexes - notably heart
rate, breathing, vomiting, salivation and sneezing – through the
cranial nerves.
Damage to the medulla can easily be fatal; particularly
susceptible to certain drugs e.g. opiates.
The Pons:
Contains the nucleii for several cranial nerves. Is a section of the
nervous system where axons can cross from one side of the body to
the opposite side.
Both the pons and medulla contain the reticular formation and the
raphe system – these systems send axons throughout the forebrain and
control the overall state of nervous system arousal.
The Cerebellum:
Is a large hindbrain structure – contributes to the control of movement,
including balance and orientation.
In addition, lateral parts of the cerebellum contribute to the speed and
skill of acquiring language and cognition (Leiner & Dow, 1989). Thus,
individuals with cerebellar damage can have problems with their
memory and finding the right word.
The Midbrain:
Although this structure starts in the middle of the brain, it is
eventually dwarfed and surrounded by the forebrain.
The roof of the midbrain is called the tectum. On either side of the
roof are two swellings, the superior colliculus and the inferior
colliculus – both are routes for sensory information.
Under the tectum is the tegmentum – is involved with the pathways
between the forebrain and spinal cord/hindbrain. It also includes
the nucleii for the 3rd and 4th cranial nerves.
Another structure is the substantia nigra, an area whose cells and
axons deteriorate in Parkinson’s disease.
The Forebrain:
This is the most prominent portion of the human brain, comprising
the cerebral cortex, limbic system and other structures including
the thalamus, hypothalamus and hippocampus.
The limbic system and sub-cortical structures
a) The hypothalamus
Has widespread connections with the rest of the fore brain and
midbrain and contains a number of distinct nucleii. Damage to
one of the hypothalmic nucleii can lead to abnormalities of one or
more motivated behaviours,
e.g. feeding, drinking, temperature regulation, level of activity.
The hypothalamus also regulates the secretion of hormones from
the pituitary gland. Is also associated with psychobiological
reactions to stress and onset of psychosomatic illness.
b) Basal ganglia
These are a group of subcortical stuctures left and right of the
thalamus these are the caudate nucleus, the putamen and the
globus pallidus.
The basal ganglia tend to be damaged in Parkinson’s disease,
Huntingdon’s disease and other conditions affecting movement.
Although the basal ganglia do not control movement directly or send
axons to the medulla or spinal cord, they do send messages to the
thalamus and midbrain which relay information to the cerebral
cortex.
The basal ganglia
c) The Hippocampus
This is a large structure between the thalamus and the cerebral
cortex (mostly towards the posterior of the forebrain). Two major
axon tracts, the FORNIX and the FIMBRIA, link the hippocampus with
the hypothalamus.
Evidence implicates this structure with memory. If damaged, learning
about new events (episodic memory) and facts (semantic memory)
become severely impaired.
In humans there are left-right differences in the function of the
hippocampus:
i) Left temporal lobe and hippocampal damaged impairs verbal
memory tasks e.g. word-paired associations.
ii) Right temporal lobe and hippocampal damage affects spatial
response learning.
d) The Thalamus
This structure is the main source of input to the cerebral cortex and
almost the only source of sensory information.
Can be described a a ‘way station’ for information going to the
cerebral cortex. Each nucleus of the thalamus sends its axons to, and
receives axons from, a particular part of the cerebral cortex.
e) The Ventricles
The cerebral ventricles are fluid-filled cavities within the brain and
extend into the central canal of the spinal cord.
The fluid is cerebrospinal fluid (CSF), similar to blood plasma. Its
function is to cushion the brain against mechanical shock when the
head moves. It also provides a reservoir of hormones and nutrition for
the brain and spinal cord.
Sometimes the flow of CSF is obstructed and accumulates within the
ventricles or subarachnoid space, thus increasing the pressure on
the brain – condition known as hydrocephalus, usually associated
with mental retardation.
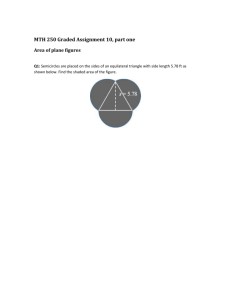
Photo showing part of the hippocampus and
thalamus
The Cerebral Cortex and Corpus Callosum
The surface of the forebrain consists of two cerebral hemispheres (one
left, one right) which cover all the other forebrain structures.
Each hemisphere is organised to receive sensory information from the
contralateral (opposite) side of the body through axons to the spinal
cord and cranial nerve nucleii.
Neurons in each hemisphere communicate with neurones in the
corresponding part of the other hemisphere by two bundles of axons,
the Corpus callosum and the smaller anterior commissure.
The microscopic structure of the cells of the cerebral cortex varies
substantially from one cortical area to another – due to differences in
function. The structures can be subdivided into four major areas:
a)
Frontal lobe – involved with planning of movement, aspects
of memory, inhibition of inappropriate behaviours.
b)
Occipital lobe – involved with vision (visual cortex).
c)
Parietal lobe – body sensations.
d)
Temporal lobe – deals with hearing and advanced visual
processing.
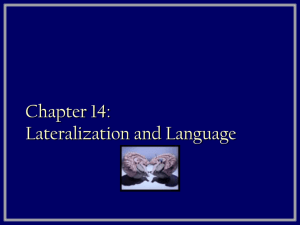
Coronal section though the human brain,
showing the location of the amygdala
The major subdivisions of the human cerebral cortex, with indications of a
few of their primary functions.
Lateralisation of Brain Function
The hemispheres of the cerebral cortex are not mirror images of
each other – have a division of labour known as “lateralisation”.
Via the Corpus callosum, each hemisphere deals with information
from both sides of the body.
It is only through damage to the C. callosum that we come to
recognise the effects of lateralisation.
Damage to the C. callosum is sometimes used to minimise the effects
of epilepsy (in v. severe cases); has the effect of reducing the effects
of epileptic seizures crossing from one hemisphere to the other.
Maturation of the Corpus callossum
Matures over 5 to 10 years – is one of the last brain structures to
attain full maturity; due to this part of the brain developing more
axons in the C. callossum than are actually needed at maturity.
The brain then selects certain axons, then discards the remainder.
Only those axons that connect to similar cells actually survive.
Two views of the corpus
callosum, a large set of
axons conveying
information between the
two hemispheres.
Brain development without the Corpus callosum
Such a condition can be due to:
a) genetic factors
b) toxins during pregnancy
Is a very rare condition; however, a person born without a C.
callossum is very different from a person who looses this structure
as a result of split-brain surgery.
The person born without a C. callossum can perform tasks that the
split-brain person cannot.
e.g. can verbally describe what they feel with either hand or describe
what they see in either visual field.
It is therefore possible that such people develop alternative
connections across the hemispheres by means of the Anterior
commisure or Hippocampal commisure.
- Such individuals can co-ordinate movements but only v. slowly – e.g
their hands may be receiving conflicting information from the two
hemispheres of the brain.
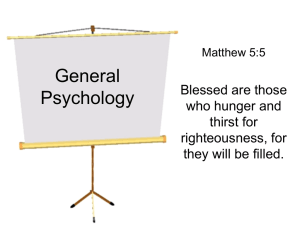
Demonstration of the
effects of damage to the
corpus callosum:
When the word “hatband” is
flashed on a screen, a
person with a split-brain
can report only what their
left hemisphere saw,
“band”.
However, with their left
hand, they can point to a
hat which is what the right
hemisphere saw.
The Split-brain Phenomon
Based primarily on the work of Roger Sperry (1960’s onwards).
The work revealed subtle behavioural effects when stimuli were
limited to one side of the body or another.
The two hemispheres of a split-brain person (SBP) can process
information and answer questions independently of each other.
e.g. Preilowski (1975) described a case where the individual
buttoned his shirt with his right hand, but unbottoned it with his left.
Such neurological conflict appears more common after neurosurgery
(Bogen, Schulz & Vogel, 1988) – important to note that the C. callossum,
once cut, cannot grow back (this applies to all nervous tissue as nerve
cells do not have the capacity to undergo cellular division).
However, the brain can utilise other sub-cortical structures to
compensate.
Function of the Right Hemisphere
Believed to support the left (major) hemisphere, but is subordinate to it;
sometimes dependant on the nature of the functions involved.
e.g. in people with intact, healthy brains, the right hemisphere is less
active than the left during speech; however, the right hemisphere
contributes to the emotional content of speech (Shapiro & Danly, 1985).
Right hemispherical damage results in poor facial expression and
difficulty in the understanding of others facial expressions (of emotion).
In addition:
i) the right hemisphere is also more adept at recognising and dealing
with complex visual patterns – notable in left-handed people;
ii) neurologists have long recognised that right hemispherical
damaged people have difficulty finding their way from one place to
another
iii) The split-brain person arranges puzzle pieces more accurately with
the left hand than with the right;
iv) The left hand does better at drawing items e.g. box, bicycle, etc.
Based upon research evidence (Levy & Sperry, 1968), the right
hemisphere appears to be specialised for the majority of
complex visual and spatial tasks.
Hemispherical Differences and Cognitive Style
There is a doubtful assumption that any given individual relies
consistently on one hemisphere or another, regardless of the task
or situation.
Rather an overstated view as anyone with an intact brain makes
use of both hemispheres for every task – each one may be more
active for certain specific tasks.
Lateralisation and Handedness
Question as to the relationship between handedness and hemispherical
dominance for speech:
Geschwind & Levitsky (1968) reported that one section of the temporal
cortex, the planum temporale, (area for speech and language) is larger:-
a) on the left side for 65% of people;
b) is equal on each side for 24% of people and
c) is larger on the right side for 11% of people.
Location of the hippocampus in relation to the temporal lobes
A study of children who died before 3 month of age revealed that the
planum temporale was larger even before language development occurs
(on average, 2× the size on the left).
Cerebral Dominance and Handedness
10% of people are left-handed (over 90 % of prehistoric drawings
indicate right handedness).
Most left-handers are partly ambidextrous.
The brain of l.h.p. is different from that of a r.h.p. but not simply the
reverse.
For 98% of r.h.p., the left hemisphere is strongly dominant for speech –
the planum temporale is decidedly larger on the left rather than the right
side.
The right hemisphere is dominant for speech in approx. 35 – 40% of lefthanders; the left hemisphere is dominant among the remainder.
The C. callosum is 11% thicker in l.h.p. – believed to be due to facilitating
cross-hemisphere communication and bilateral representation of brain
function.
Reasons for Left-handedness
Possible causes:
Genetics;
Biological factors e.g. hormones which modify
other parts of the body;
Organic brain damage – minimal cerebral
dysfunction.
Geschwind & Garaburda, 1985) – evidence indicated that the hormone
testorsterone contributed to left-handedness.
High levels of testosterone during the formative years may delay
maturation of the left hemisphere and retard growth of the thymus gland
and related structures implicated with the immune system.
Also, high levels of testosterone appear to result in a more highly
developed right hemisphere.
The hormonal theory may also apply to the fact that:
Left handedness is more common in males than in females as also are
allergies, stuttering and certain immune disorders.
In terms of the differences in right and left handedness (left and
right cerebral dominance):
Left-handers are more likely to experience neuronal abnormalities
in their left hemisphere; this may include:
Dyslexia
Childhood allergies
Migraine headaches (in adulthood)
Disorders of the immune system
Increased likelihood of stuttering – debatable issue
However, many left-handed individuals are found to excel in areas such
as:
Mathematics
Aspects of science
Architecture and design, due to their enhanced
visual and spatial orientation.
 0
0