Digestion Physiology Chapter 26
advertisement

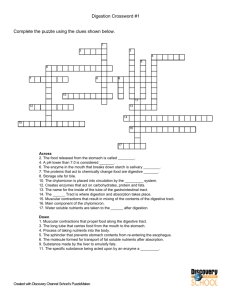
Digestion Physiology Chapter 26 Test (Chapters 25 & 26) April 6th and 7th (next block day) March 28, 2011 Announcements: • • • • Turn in last week’s warm ups to the box Pick up new warm up sheet Practical grades in gradebook Practical make up: – Today after school @ 3:15 – Tuesday morning 6:45 Warm Ups: 1. 2. 3. 4. 5. In the large intestine longitudinal muscles are grouped into strips called _______; circular muscles are grouped into rings are form _______. What is produced in the appendix? The two lobes of the liver are connected by the: What are gallstones? Through what two pathways does blood enter the hepatic lobules? Primary Mechanisms of Digestive System (Table 26-1) • Ingestion – take food in • Digestion – break down complex nutrients into simpler nutrients • Motility – movement of GI tract; aids in digestion • Secretion – enzymes are required for digestion to take place • Absorption – movement across GI mucosa into the internal environment • Elimination – process of eliminating unabsorbed material Mechanical Digestion • All motility of the digestive tract that cause the following changes: – Change in physical state of the food for large particles to smaller particles – Churning of the GI lumen to mix particles with digestive juices – Propelling food forward ending with elimination Mastication • • • • Mastication = chewing Requires tongue, cheek and lips Reduces particle size Mix food with saliva Deglutition • Deglutition = swallowing 1. Oral stage • • • Bolus is formed voluntarily Tongue pushes bolus against the palate and into the oropharynx Soft palate acts as a valve to prevent food from entering the nasopharynx 2. Pharyngeal stage • • Involuntary reflexes push bolus toward esophagus Epiglottis prevents food from entering trachea • Involuntary reflexes move bolus towards stomach 3. Esophageal stage Motility • Smooth muscle contractions take over in the lower portion of the esophagus • Peristalsis – progressive wavelike ripple of the muscle layer of a hollow organ – Bolus stretches the GI tract wall triggers contraction of circular smooth muscle bolus moves forward Motility • Segmentation – mixing movement; back and forward movement within a single region – Mechanically breakdown food particles – Mix food and digestive juices together – Facilitate absorption • Peristalsis and segmentation can occur in alternating sequence to churn/mix and progress food Peristalsis & Segmentation Regulation of Motility • Gastric Motility – Emptying the stomach takes approx 2-6 hours after a meal – Food is churned with digestive juices to form chyme • Ejection every 20 seconds into the duodenum • Controlled by hormonal and nervous mechanisms Regulation of Motility • Hormonal Control – Fats and nutrients in duodenum cause secretion of gastric inhibitory peptide (GIP) from the intestinal mucosa into the bloodstream • Slows peristalsis in stomach; decreasing passage of food into the duodenum Regulation of Motility • Nervous Control – Nerve receptors in duodenum are sensitive to acid and distention • Sensory and motor fibers within the vagus nerve (CN X) cause a reflex inhibition of gastric peristalsis (enterogastric reflex) Regulation of Motility • Intestinal Motility • Takes approx 5 hours for food to pass through the small intestine – Segmentation • Mixes chyme and digestive juices from liver, pancreas and intestinal mucosa • causes contact with intestinal mucosa to increase absorption – Peristalsis • Continues in the jejunum to move food into the large intestine • Stimulated by the hormone cholecystokinin-pancreozymin (CCK) – Secreted by intestinal endocrine cells in the presence of chyme Mechanical Digestion • Summarized in Table 26-2; page 775 Chemical Digestion • Consists of all the changes in the chemical composition of food • Result of hydrolysis – Compounds combine with water then split into simpler compounds – Enzymes catalyze the hydrolysis of foods Chemical Digestion • Six main types of chemical substances: – Carbohydrates, proteins, fats, vitamins, mineral salts, water – Only carbohydrates, proteins and fats must undergo chemical digestion to be absorbed Digestive Enzymes Properties • Extracellular enzymes • Classified as hydrolases • Function optimally at a specific pH – Ex: amylase vs pepsin • Continually destroyed or eliminated • Most digestive enzymes are synthesized and secreted as proenzymes – Kinases convert proenzymes to active enzymes Carbohydrate Digestion • Carbohydrates are saccharide compounds – Contain one or more saccharide groups • Polysaccharides – starches & glycogen • Disaccharides – sucrose, lactose and maltose • Monosaccharides – glucose, fructose & galactose Carbohydrate Digestion • Polysaccharides are hydrolyzed by amylases – Present in saliva and pancreatic juice • Sucrose, lactose and maltose are hydrolyzed by sucrase, lactase, and maltase – Located on epithelial cells lining villi in small intestine – End result (usually glucose) is located at site of absorption (“contact digestion”) Protein Digestion • Proteins are large molecules composed of twisted chains of amino acids • Proteases catalyze the hydrolysis of proteins into smaller compounds – Proteoses peptides amino acids • Proteins have varying peptide bonds holding amino acids together = increased need for varying proteases Protein Digestion - Proteases • Pepsin – gastric juice • Trypsin and chymotrypsin – pancreatic juice • Peptidases – intestinal brush border Proteoses Fat Digestion • Fats are insoluble in water – must be emulsified prior to digestion – Emulsify = dispersed as small droplets – Lecithin and bile salts emulsify oils and fats in the small intestine by forming micelles (fig 26-8, page 778) – Lecithin mixes with fat to form micelles • Fats broken down by mechanical digestion are further broken down by lipase • Action of lipase is enhanced by colipase (released from the pancreas) Residuals of Digestion • Certain compounds cannot be digested in humans b/c we lack the enzyme required for hydrolysis • These compounds are excreted in the feces • Cellulose (dietary fiber), connective tissue from meat (collagen), undigested fats combined with calcium and magnesium, bacteria, pigments, water, mucous Chemical Digestion • Summarized in Table 26-3, page 779 Secretion • Release of substances from exocrine glands in the GI tract – Saliva, gastric juice, bile, pancreatic juice, intestinal juice Saliva • Secreted from salivary glands • Water component helps liquefies food chyme – Allows enzymes to mix with food particles • Mucus lubricates food to protect mucosa lining • Amylase – chemically digest starch and glycogen • Lipase (small amounts) – digest lipids – Decreased function when fat are not emulsified • Sodium bicarbonate (NaHCO3) – Dissociated in water – Bicarbonate ions bind with H+ to increase pH Control of Salivary Secretion • Controlled by reflex mechanisms: – Olfactory & visual stimuli send impulses to centers in the brainstem efferent impulses to salivary glands – Chemical and mechanical stimuli comes from the presence of food in the mouth Gastric Juice • Secreted by gastric glands surrounds by gastric pits • Chief cells – secrete enzymes of digestive juices – Pepsin (proenzyme = pepsinogen) • Pepsinogen is activated by hydrochloric acid (HCl) • Parietal cells – Secrete HCl • Decreases stomach pH; increases blood pH – Secrete intrinsic factor • Binds to molecules of vitamin B12 to facilitate absorption in the small intestine Control of Gastric Secretion • Gastric secretion is controlled by 3 phases: 1. Cephalic phase (“psychic phase”) – – – Sight, smell, taste, thought of food activate control centers in medulla oblongata Parasympathetic fibers of the vagus nerve conduct impulses to gastric glands Vagal impulses stimulate production of gastrin • Gastrin stimulates gastric secretion Control of Gastric Secretion 2. Gastric phase: – Gastrin secretion is further stimulated by the presence of products of protein digestion & distention – Gastrin continue to stimulate the secretion of gastric juices (high pepsinogen and HCl content) Control of Gastric Secretion 3. Intestinal phase: – Gastric inhibitory peptide (GIP) in secreted in the small intestine in the presence of fats and carbohydrates • Decrease gastric motility and secretion – Secretin secreted in the small intestine in the presence of acid, digested proteins and fats • Inhibit gastric secretion • Simulate secretion of pancreatic enzymes • Stimulate ejection of bile into small intestine – CCK • • • • Secreted in the small intestine in the presence of chyme Stimulates ejection of bile from gallbladder Stimulates secretion of pancreatic juices Opposes action of gastrin; raises pH of gastric juice Pancreatic Juice • Secreted by exocrine acinar cells of the pancreas • Mostly water • Enzymes: – – – – Trypsin and chymotrypsin (proteases) Lipases Nucelases (RNA and DNA digesting enzymes) Amylase (starch digesting enzyme) • Secrete bicarbonate into the GI lumen and H+ into the blood to buffer the effects parietal cell secretion (fig 26-10 and fig 26-11) Control of Pancreatic Secretion • Secretin – Stimulates the secretion of pancreatic fluid high in bicarbonate to neutralize acidity of chyme in the small intestine – See notes under “Control of Gastric Section – Intestinal phase” • CCK – see above Bile • Secreted by liver and stored in gallbladder • Lecithin and bile salts – Emulsify fats by creating a hydrophilic “shell” around tiny fats droplets • Sodium Bicarbonate – increase pH of chyme in small intestine • Excretions: – Cholesterol, products of detoxification, bilirubin (product of hemolysis) Control of Bile Secretion • Controlled by CCK and secretin • See Table 26-5, page 782 Intestinal Juice • Mucus – provides lubrication • Sodium bicarbonate – increases pH to allow intestinal enzymes to function at optimal level • Water – carries mucus and NaHCO3 **Study These Tables** Table 26-4: Digestive Secretions Table 26-5: Actions of Digestive Hormones Both on page 782 Wednesday/Thursday 3/30-3/31 Warm Up: 1. Name the 5 components of saliva. 2. What is the proenzyme of pepsin? What is needed to activate this proenzyme? 3. Explain the role of bicarbonate in the GI tract. 4. The control of gastric secretion can be broken up into 3 phases. Name these phase and briefly describe each one. 5. Name and give the function of the 5 enzymes found in pancreatic juice. Absorption • Passage of substances (digested foods, vitamins, salts, water) across the mucosa into the blood • Majority of absorption takes place in small intestine where surface area is increased Mechanisms of Absorption • Some substances (water) are absorbed via diffusion • Secondary Active Transport (ex: Sodium) – Na+ is actively transported from the basal (backside) of epithelial cells lining the lumen of the small intestine into blood capillaries – Creates a low intracellular sodium concentration – Na+ ions diffuse passively from the lumen into epithelial cells – Fig 26-14, page 785 Mechanisms of Absorption • Sodium cotransport – Glucose is very large and hydrophilic – Requires carrier to cross intestinal mucosa – Carriers bind sodium and glucose together to passively transport out of lumen • Amino Acid absorption – Transported by passive carriers on luminal and basal surfaces of absorptive cells – Brush border enzymes can also act as carriers – Polypeptides can diffuse into absorptive cells, hydrolyze into amino acids, diffuse into blood Mechanisms of Absorption • Fatty acid/monoglyceride absorption – Bile salts and lecithin form micelles – Fat digestion takes place within these tiny spheres – At the intestinal brush border, micelle contents can diffuse into absorptive cells – Inside triglycerides reform within chylomicrons – Water soluble chylomicrons allow fats to be transported through lymph and into bloodstream Mechanisms of Absorption • Absorption of vitamins – Vitamins A, D, E, K are fat-soluble • Depend on bile salts for absorption – B Vitamins require carrier-mediated transport • Ex: Vit B12 and intrinsic factor Summary of Absorption • See table 26-6, page 787 Elimination • Expulsion of digestive residuals from the digestive tract in the form of feces – Defecation – Normally rectum is empty – Massive peristalsis of feces into the rectum stimulate receptors and relax the external anal sphincter – Voluntary control Elimination • Constipation – Contents move through large intestine at a slower rate – Increased water absorption occurs resulting in hardened feces • Diarrhea – Result of increased motility of the small intestine – Water absorption does not occur GI Tract Disorders • Common S/S – Gastroenteritis • Gastritis – stomach inflammation • Enteritis – intestinal inflammation – Anorexia: chronic loss of appetite – Nausea: feeling of needing to vomit; may progress to vomiting – Emesis: vomiting – Diarrhea: elimination of liquid feces; abdominal cramps may also be present – Constipation: decreased motility of colon; difficulty in defecating GI Tract Disorders • Ulcers – In stomach or duodenum – Cause pain and may lead to perforation of the wall of the GI tract – Bleeding anemia – Causes: • Hyperacidity • H. phylori bacterium GI Tract Disorders • Stomach cancer – Linked to excessive alcohol use, chewing tobacco, eating heavily preserved foods – Early signs: • Heartburn, belching, nausea – Later signs: • Chronic indigestion, vomiting, anorexia, stomach pain, blood in feces GI Tract Disorders • Diverticulosis – presence of abnormal sac-like projections on the large intestine (diverticula) – When inflamed causes diverticulitis – S/S: pain, tenderness, fever GI Tract Disorders • Colitis – inflammation of the large intestine – s/s: diarrhea, abdominal cramps, constipation, bleeding, intestinal ulcers – Crohn’s Disease: autoimmune colitis – Treatment: surgical removal of affected portions of the intestine GI Tract Disorders • Irritable bowel syndrome (IBS) – “spastic colon” – Noninflammatory condition usually caused by stress – Diarrhea or constipation GI Tract Disorders • Colorectal cancer – Occurs after 50 – Associated with low-fiber, high-fat diet – Early signs: change in bowel habits, fecal blood, rectal bleeding, abdominal pain, unexplained anemia, weight loss, fatigue Liver Disorders • Hepatitis – inflammation of the liver – S/S: jaundice, liver enlargement, anorexia, abdominal discomfort, gray-white feces, dark urine – Causes: alcohol or drug abuse; bacterial or viral infection • Cirrhosis – degenerative liver condition – Tissue can no longer regenerate