Fig. 18.5 - Plain Local Schools
advertisement

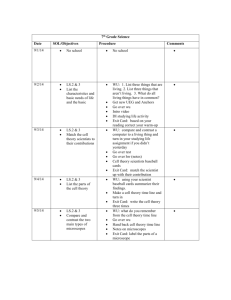
Chapter 18 Major Mental Disorders Table of Contents Exit Key Questions What are the general characteristics of psychosis? How do delusional disorders differ from other forms of psychosis? What forms does schizophrenia take? What causes schizophrenia? What are mood disorders? What causes depression? How are major mental disorders treated? Who do people commit suicide? Can suicide be prevented? What does it mean to be “crazy”? What should be done about it? Table of Contents Exit Psychosis- “Losing It” Page 584 Table of Contents Exit Psychosis: Loss of contact with shared views of reality Hallucinations: Imaginary sensations, such as seeing, hearing, or smelling things that do not exist in the real world Most common psychotic hallucination is hearing voices Note that olfactory hallucinations sometimes occur with seizure disorder (epilepsy) Table of Contents Exit Delusions: False beliefs that individuals insist are true, regardless of overwhelming evidence against them 1. Depressive 2. Somatic 3. Grandeur 4. Influence 5. Persecution 6. Reference Table of Contents Exit Some More Psychotic Symptoms Flat Affect: Lack of emotional responsiveness; face is frozen in blank expression Disturbed Verbal Communication: Garbled and chaotic speech; word salad Personality Disintegration: When an individual’s thoughts, actions, and emotions are uncoordinated Brief Reactive Psychosis: Psychotic symptoms typically appear after an extremely stressful event Table of Contents Exit Table 18-1 Common Warning Signs of Psychosis and Major Mood Disorders Expresses bizarre thoughts or beliefs that defy reality Has withdrawn from family members and other relationships Hears unreal voices, sees things others don’t Is extremely sad, persistently despondent, or suicidal Is excessively energetic, has little need for sleep Loses appetite, sleeps excessively, has no energy Exhibits extreme mood swings Believes someone is trying to harm her or him Has engaged in anti-social, destructive, or self-destructive behavior Table of Contents Exit Other Psychotic Disorders Organic Psychosis: Psychosis caused by brain injury (gunshot wound) or disease Functional psychosis Based on unknown causes or psychological factors Table of Contents Exit Organic Psychosis Dementia: Most common organic psychosis; serious mental impairment in old age caused by brain deterioration Archaically known as senility (senile dementia) Alzheimer’s Disease: Symptoms include impaired memory, confusion, and progressive loss of mental abilities Ronald Reagan most famous Alzheimer’s victim (Page 587) Table of Contents Exit Organic Psychosis Cinema Education The Notebook A Moment to Remember (Subtitled) Table of Contents Exit Delusional Disorders Delusional Disorders: Marked by presence of deeply held false beliefs (delusions) May involve delusions of grandeur, persecution, jealousy, or somatic delusions Experiences could really occur! Paranoid Psychosis: Most common delusional disorder Centers on delusions of persecution Table of Contents Exit Schizophrenia: The Most Severe Mental Illness Schizophrenia: Psychotic disorder characterized by hallucinations, delusions, apathy, thinking abnormalities, and “split” between thoughts and emotions Does NOT refer to having split or multiple personalities Table of Contents Exit The Four Subtypes of Schizophrenia Disorganized (Hebephrenic) Type: Incoherence, grossly disorganized behavior, bizarre thinking, and flat or inappropriate emotions Catatonic Type: Marked by stupor, unresponsiveness, posturing, and mutism Paranoid Type: Preoccupation with delusions; also involves auditory hallucinations that are related to a single theme, especially grandeur or persecution Undifferentiated Type: Any type of schizophrenia that does not have specific paranoid, catatonic, or disorganized features or symptoms Table of Contents Exit © Bruce Ely/Getty Images Fig. 16.6 Over a period of years, Theodore Kaczynski mailed bombs to unsuspecting victims, many of whom were maimed or killed. As a young adult, Kaczynski was a brilliant mathematician. At the time of his arrest, he had become the Unabomber—a reclusive “loner” who deeply mistrusted other people and modern technology. After his arrest, Kaczynski was judged to be suffering from paranoid schizophrenia. Table of Contents Exit Causes of Schizophrenia Environment Psychological Trauma: Psychological injury or shock, often caused by violence, abuse, or neglect Disturbed Family Environment: Stressful or unhealthy family relationships, communication patterns, and emotional atmosphere Deviant Communication Patterns: Cause guilt, anxiety, anger, confusion, and turmoil Double-bind communication: Places the listener in an unsolvable emotional conflict, or “no-win” situation Table of Contents Exit Causes of Schizophrenia Heredity Some individual inherit a potential for developing schizophrenia They are more vulnerable to the disorder than others are EX: If 1 identical twin becomes schizophrenic (identical twins have identical genes) then the other twin has a 48% chance of also becoming schizophrenic Table of Contents Exit Research Classic The Genain Sisters- Trouble times four (page 592) Table of Contents Exit Fig. 16.7 Lifetime risk of developing schizophrenia is associated with how closely a person is genetically related to a schizophrenic person. A shared environment also increases the risk. (Estimates from Lenzenweger & Gottesman, 1994.) Table of Contents Exit Biochemical Causes of Schizophrenia Biochemical Abnormality: Disturbance in brain’s chemical systems or in the brain’s neurotransmitters Dopamine: Neurotransmitter involved with emotions and muscle movement Works in limbic system Dopamine overactivity in brain may be related to schizophrenia Table of Contents Exit Fig. 18.3 Dopamine normally crosses the synapse between two neurons, activating the second cell. Antipsychotic drugs bind to the same receptor sites as dopamine does, blocking its action. In people suffering from schizophrenia, a reduction in dopamine activity can quiet a person’s agitation and psychotic symptoms. Table of Contents Exit Louis Wain This series of paintings by Louis Wain reflects a troubled personality. Wain was a British illustrator who became schizophrenic in middle age. As Wain’s psychosis progressed, his cat paintings became highly abstract and fragmented. In many ways, Wain’s paintings resemble the perceptual changes caused by psychdelic drugs such as LSD. Recent research suggests that psychosis may, in fact, be the result of mind-altering changes in brain chemistry Table of Contents Exit Schizophrenic Brain Computed Tomography (CT) Scan: Computer enhanced X-ray of brain or body Magnetic Resonance Imaging (MRI) Scan: Computer enhanced three-dimensional image of brain or body; based on magnetic field MRIs show schizophrenic brains as having enlarged ventricles Positron Emission Tomography (PET) Scan: Computer-generated color image of brain activity; radioactive sugar solution is injected into a vein, eventually reaching the brain Activity is abnormally low in frontal lobes of schizophrenics Table of Contents Exit © Dennis Brack/Stockphoto.com76 Fig. 18.4 (left) CT scan of would-be presidential assassin John Hinkley, Jr., taken when he was 25. The X-ray image shows widened fissures in the wrinkled surface of Hinkley’s brain. (right) CT scan of a normal 25-year-old’s brain. In most young adults the surface folds of the brain are pressed together too tightly to be seen. As a person ages, surface folds of the brain normally become more visible. Pronounced brain fissuring in young adults may be a sign of schizophrenia, chronic alcoholism, or other problems. Table of Contents Exit Fig. 18.5 Positron emission tomography produces PET scans of the human brain. In the scans shown here, red, pink, and orange indicate lower levels of brain activity; white and blue indicate higher activity levels. Notice that activity in the schizophrenic brain is quite low in the frontal lobes (top area of each scan) (Velakoulis & Pantelis, 1996). Activity in the manic-depressive brain is low in the left brain hemisphere and high in the right brain hemisphere. The reverse is more often true of the schizophrenic brain. Researchers are trying to identify consistent patterns like these to aid diagnosis of mental disorders. Table of Contents Exit Schizophrenia Beautiful Mind Table of Contents Exit Stress-Vulnerability Model Stress-Vulnerability Hypothesis: Combination of environmental stress and inherited susceptibility cause schizophrenic disorders Table of Contents Exit Fig. 18.6 Various combinations of vulnerability and stress may produce psychological problems. The top bar shows low vulnerability and low stress. The result? No problem. The same is true of the next bar down, where low vulnerability is combined with moderate stress. Even high vulnerability (third bar) may not lead to problems if stress levels remain low. However, when high vulnerability combines with moderate or high stress (bottom two bars) the person “crosses the line” and suffers from psychopathology. Table of Contents Exit Mood Disorders Mood disorders: Depressive Disorders: Moderate depression that lasts for at least two years Cyclothymic Disorder: Involve both depression and mania or hypomania Dysthymic Disorder: Sadness or despondency are prolonged, exaggerated, or unreasonable Bipolar Disorders: Major disturbances in emotion, such as depression or mania Moderate manic and depressive behavior that lasts for at least two years Reactive depression: Is an episode of despondency that follows some identifiable event Table of Contents Exit Major Mood Disorders Major mood disorders: Major Depressive Disorder: Lasting extremes of mood or emotion and sometimes with psychotic features (hallucinations, delusions) A mood disorder where the person has suffered one or more intense episodes of depression; one of the more serious mood disorders Bipolar I Disorder: Extreme mania and deep depression; one type of manic-depressive illness Bipolar II Disorder: Mania: Excited, hyperactive, energetic, grandiose behavior Person is mainly sad but has one or more hypomanic episodes (mild mania) Affective psychosis: Combination of mood disorder and a break with reality Table of Contents Exit Major Mood Disorders (cont.) Endogenous Depression: Depression that seems to be produced from inside the body (due to chemical imbalances) and NOT from life events Seasonal Affective Disorder (SAD): Depression that only occurs during fall and winter May be related to reduced exposure to sunlight Phototherapy: Extended exposure to bright light to treat SAD Table of Contents Exit Batman and his Foes Comic Book characters and their problems Table of Contents Exit Feeling Sad? It Could Be SAD Page 598 Table of Contents Exit Fig. 18.7 Seasonal affective disorder appears to be related to reduced exposure to daylight during the winter. SAD affects 1 to 2 percent of Florida’s population, about 6 percent of the people living in Maryland and New York City, and nearly 10 percent of the residents of New Hampshire and Alaska (Booker & Hellekson, 1992). Table of Contents Exit © Dan McCoy/Rainbow Fig. 18.8 An hour or more of bright light a day can dramatically reduce the symptoms of seasonal affective disorder. Treatment is usually necessary from fall through spring. Light therapy typically works best when it is used early in the morning (Lewy et al., 1998). Table of Contents Exit Maternity Blues Maternity Blues: Mild depression that lasts for one to two days after childbirth Marked by crying, fitful sleep, tension, anger, and irritability Brief and not too severe Table of Contents Exit Postpartum Depression Postpartum Depression: Moderately severe depression that begins within three months following childbirth Marked by mood swings, despondency, feelings of inadequacy, and an inability to cope with the new baby May last from two months to one year Part of the problem may be hormonal Table of Contents Exit Fig. 18.9 At least one schizophrenic patient in four had completely recovered 10 years after being diagnosed. Three out of four had improved. New treatments for schizophrenia and other major mental disorders may improve these odds. (Source: FDA Consumer, 1993.) Table of Contents Exit Therapeutic Interventions Psychotherapy: Any psychological treatment for behavioral or emotional problems Typically involves two people talking about one’s personal problems Somatic Therapies: Bodily Drug therapy, hospitalization, or psychosurgery Pharmacotherapy: Use of drugs to alleviate the symptoms of emotional disturbance Table of Contents Exit Pharmacotherapy What type of drugs are used in pharmacotherapy? Tranquilizers Drugs (Valium) that produce relaxation or reduce anxiety Antidepressants Are mood elevating drugs used to combat depression Antipsychotics Drugs that, in addition to having tranquilizing effects, also tend to reduce hallucinations and delusional thinking. Table of Contents Exit Psychiatric “Wonder Drugs” Read page 601 Table of Contents Exit Shock Electroconvulsive Therapy (ECT) A 150-volt electrical current is passed through the brain for slightly less than a second How does shock help? It is the seizure that helps, which is induced by the shock Table of Contents Exit Psychotherapy Psychotherapy Any surgical alteration of the brain Best known psychotherapy Prefrontal lobotomy: The frontal lobes are surgically disconnected from the other areas of the brain Deep lesioning: Small target areas are destroyed in the brain’s interior Table of Contents Exit Suicide: Major Risk Factors Drug or alcohol abuse Prior suicide attempt Depression or other mood disorder Availability of a firearm Severe anxiety or panic attacks Family history of suicidal behavior Shame, humiliation, failure or rejection Table of Contents Exit Fig. 18.10 Adolescent suicide rates vary for different racial and ethnic groups. Higher rates occur among whites than among non-whites. White male adolescents run the highest risk of suicide. Considering gender alone, it is apparent that more male than female adolescents commit suicide. This is the same as the pattern observed for adults. Table of Contents Exit Common Characteristics of Suicidal Thoughts and Feelings (Page 605) Escape Unbearable Psychological Pain: Emotional pain that the person wishes to escape Frustrated Psychological Needs: Such as searching for love, achievement, or security Constriction of Options: Feeling helpless and hopeless and deciding that death is the only option left Table of Contents Exit Fig. 16.16 Suicidal behavior usually progresses from suicidal thoughts, to threats, to attempts. A person is unlikely to make an attempt without first making threats. Thus, suicide threats should be taken seriously (Garland & Zigler, 1993). Table of Contents Exit