MS PowerPoint (24 pp. 207 kB)
advertisement
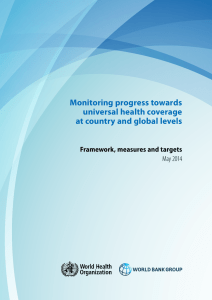
")
Universal Health Coverage: How does your (RBF or not RBF) solution fare? Bruno Meessen, ITM & PBF CoP Expert Talk, Eschborn, December 12th 2012 An assessment of the problem • Health situation in LICs is unacceptable: – Overall status (health / social protection); – Inequity, esp. the poorest. • Yet, we know pretty well the interventions which are needed. • Health system delivery is part of the problem. USE OF BASIC MATERNAL AND HEALTH SERVICES Coverage Rates among Lowest and Highest 20% of the Population in 56 Developing and Transitional Countries (David Gwatkin, 2007) 100 90 80 70 60 50 40 30 20 10 0 Antenatal Care Oral Rehydration Thereapy Full Immunization Med. Treatment of Ac. Res. Inf. Lowest 20% of Population Att. Delivery Med. Treatment of Fever Highest 20% of Population Modern Contra. Use (Women) Contribution to UHC as the bottom line “Everyone should be able to access health services and not be subject to financial hardship in doing so”. (WHA resolution 58.33 2005). Could one structure a bit the contribution of a scheme / initiative / solution to UHC? The 12 desirable traits of any potential solution • Such a solution builds the path to universal coverage, by: Increasing direct benefits to the priority groups. • (1) Increasing resources to health. • (2) Reducing barriers, especially for the most vulnerable groups. • (3) Paying attention to quality of service in public facilities. • (4) Enhancing an efficient use of resources. • (5) Paying attention to quality of care, across the board. • (6) Protecting against impoverishment. Consolidating the system. • (7) Fixing ‘health system problems’. • (8) Being harmonious with other health strategy. • (9) Not undermining control by national health authorities… • (10) But improving their accountability and contribute to overall better governance. • (11) Being scalable, sustainable and appropriate as a stage in a long-term process. • (12) Consolidating the political momentum for UHC and rights to health. (1) Contribute to resource mobilisation • Does the solution increase altruism/solidarity, trust and financial commitment by tax payers, Ministry of Finance, donors and tax payers from the North? • Does it enhance disbursment of the allocated budget? • Ideal features: – – – – – Predictibility. Deliver benefits (in kind or cash) directly to target groups. Traceability. Complete contract. Mismanagement-proofed. • NB: (1) the environment has changed; (2) the future of health care financing in most LICs is national resources (domestic revenue). (2) Remove barriers faced by the users, and the most vulnerable in particular • Quite poor performance of the dominant model (NHS with free preventive services and user fees for curative services). Cf. David Gwatkin analyses. • Can the solution target resources (if needed)? • What is its scale? • Does the solution address remaining barriers on the demand side, at least for the most vulnerable? – – – – Out-of-pocket payment for curative services. Distance. Transport. Knowledge. (3) Improve quality of services • The role of barriers on the supply side is underestimated. Their vulnerability to health facility managers as well. • Will the solution bring about improvements in terms of: – – – – – – – – Availability of qualified staff. Availability of drugs. Cleanliness. Opening hours. Friendliness. Queues. Respect of dignity. … (4) Improve efficiency • Value for Money is not an agenda of donors only. Cf. Kaberuka 2011. • This is a requirement for all resources – including private and public resources. • Does the solution contribute to greater : – Allocative efficiency (promote high impact interventions). – Technical efficiency (get the maximum from the staff, equipment and infrastructure). – ‘Transactional’ efficiency (limited transaction costs) (5) Improve quality of care • Efficiency requires effectiveness of treatment. Quality of care is a huge problem in many LICs, across the board. • How does the solution address quality of care? – Keep in mind that quality of care has many determinants, some can be influenced by health facility managers. Some components are verifiable ex ante, some ex post, some are not. – What about the Private for Profit providers? (6) Reduce risk of impoverishment • How does the solution protect against catastrophic health care expenditure and income loss / iatrogenic poverty? • In the public sector, but also in the private sector. => It is about insurance, but also regulation of providers and shaping health seeking behaviours. Many interventions show some of these 6 traits. But a UHC friendly solution should also fulfill 6 other ‘systemic’ requirements. (7) Address structural health system problems • Does the solution contribute to – Better performance by the public facilities, support services (e.g. drug supply) and administration (e.g. SIS); – Fair treatment of the private not for profit; – Harnessing the private for profit providers? • Some interesting tracks: – Voice and exit mechanisms, separation of functions, clarification of missions, contract, purchaser-provider split, autonomy, neutrality to ownership of the providers, independent verification, measurement, sanction. (8) Harmonization with other interventions • Many ways to respect the first 6 components. • Is your solution in line with other interventions respecting the 6 traits? Does it help to counter / correct solutions which do not respect the 6 first traits? • A particular risk for UHC: multiplication of schemes; vertical approaches; loss of the main objective. (9) Consolidate leadership by the Ministry of Health • The solution should not be forced from outside. Political and technical leadership by national authorities is needed for sustainability, but also as a mechanism to ensure (8). • Is the solution implemented in such a way that it empowers the MoH (esp. in donor dependent countries)? (10) Contribute to overall better governance • Trait 9 should not conflict with accountability to citizens. • Poor performance of the health sector is indeed also the outcome of constraints outside the sector, including lack of accountability. • The solution should combat/shortcut embezzlement and fraud; care for transparency; resist pressure from vested interests by establishing a culture of policy experimentation, monitoring and evaluation. (11) Scalability, sustainability and path dependency • Is the solution scalable, sustainable and putting the health system on a good path? • Scale: can you ensure that all individuals belonging to the target group are covered? • If sustainability is required, can the solution be integrated in public funding and operated by national actors? • Path dependency: how does the solution affect the balance of power for stakeholders such as insurees, providers, private insurance funds, pharmaceutical sector…? (12) Consolidating the UHC momentum • We are technicians, but UHC is about politics. Cf. Thailand, Rwanda, Venezuela! • Does the solution get visibility at voter level? Political pay-off? • Does it consolidate rights to health? Our rough assessment • Many RBF solutions score pretty well on these 12 traits. • Some RBF approaches score better than some others on some traits. => How do others think about this? RBF, strategic purchasing and the agenda of health financing for universal coverage Efficiency (more health for the money) as one of the key pathways to Universal Coverage identified in WHR2010 Strengthening purchasing is a key to building domestic health financing systems – It means using information on provider performance or population health needs to drive resource allocation – Builds capacity; people have to analyze and use this information for decision-making – Changes system culture, shakes up bureaucratic inertia RBF – PBF – P4P etc. are all examples of strategic purchasing 20 | HF for UHC concepts, principles, lessons BTC Brussels, 3 December 2012 Joe Kutzin As with health insurance schemes, think from scheme to system with PBF PBF/RBF should not be run like a "scheme" or "project", but as a step in the process of moving systems towards more strategic purchasing – Long-term capacity building for the purchaser (and investing in understanding by the providers) is much more important than trying to "prove" whether it works or not (because we know that passive budgeting or unmonitored fee-for-service does not work) 21 | HF for UHC concepts, principles, lessons BTC Brussels, 3 December 2012 Joe Kutzin A bad RBF project… …is run by donors (or institutionalizes the idea that the money for these incentives will be managed separately) …overdoes the financial incentives in a way that can't be sustained by the government …is only interested in "proving that it works" in the short run, rather than always acting with the intent to move from scheme to system …overwhelms domestic capacity with too many new things to monitor …does not address the institutional platform that will, in the future, be required to attract and retain the people with the necessary skills to be good purchasers Joe Kutzin Operation: our assessment 1. RBF can be a tool for bilateral aid to contribute to UHC. 2. Bilateral aid can help in trying out new strategies. 3. Coordination will be key. • Thank you.