Integrating Motivational Interviewing, the Stages
advertisement

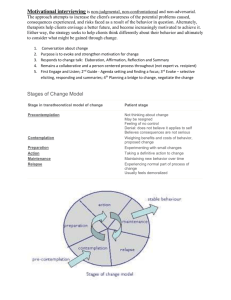
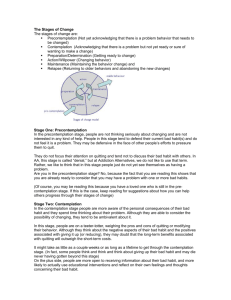
Integrating Motivational Interviewing, the Stages of Change Model, and Treatment Planning Kevin Glavin – Kent State University kglavin@kent.edu Rachel Hoffman – Kent State University rhoffman@kent.edu All-Ohio Counselors Conference November 2-4, 2005 Agenda 1. 2. 3. 4. 5. 6. 7. Background & Introduction to the Stages of Change Model (Transtheoretical Model) The Stages of Change: Key points Practical Applications • Teaching treatment planning and case conceptualization. • Educating clients about the stages of change Motivational Interviewing Techniques Moving through the stages: Techniques and Strategies The Processes of Behavior Change Determining a Client’s Stage of Change using SOCRATES Background Information • During his college years, psychologist James Prochaska, Ph.D., lost his father to alcoholism and depression. Prochaska reported his father’s mistrust in psychotherapy and his refusal to participate in counseling. This served to fuel Prochaskas’ research into substance abuse and the stages of change. • Prochaska and DiClemente started their research by observing individuals who had over come an addiction to nicotine. They discovered change occurred on a continuum and identified common stages and processes individuals appear to progress through. The model is named the Transtheoretical Model — spans so many different theories. • This model provides practitioners with a way in which to understand how clients change, as well as what motivates them to change. It can be used to teach case conceptualization, and build appropriate stage related interventions into treatment plans. The Stages of Change Model: Transtheoretical Model (Prochaska & DiClemente, 1982) • The central organizing construct of the model is the Stages of Change • The Transtheoretical Model views change as a process involving progress through a series of five stages – – – – – Precontemplation Contemplation Preparation Action Maintenance • The goal is to determine which stage of change the client is in and assist the client in progressing through subsequent stages. The Stages of Change Has changed behavior for more than 6 months No intention of changing behavior Has changed behavior for less than 6 months Intends to change in the next 6 months, but may procrastinate Intends to take action soon, for example next month Source: http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat5.section.62561 Change is Dynamic and Cyclical • It is important to note that the change process is cyclical, and individuals typically move back and forth between the stages and cycle through the stages at different rates. In one individual, this movement through the stages can vary in relation to different behaviors or objectives. Individuals can move through stages quickly. Sometimes, they move so rapidly that it is difficult to pinpoint where they are because change is a dynamic process. It is not uncommon, however, for individuals to linger in the early stages. • For most substance-using individuals, progress through the stages of change is circular or spiral in nature, not linear. In this model, recurrence is a normal event because many clients cycle through the different stages several times before achieving stable change. The five stages and the issue of recurrence are described below. Source: http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat5.section.61626 Key Points 1. Prochaska and DiClemente argue that behavior change cannot be thought of as a specific event occurring at a specific point in time. Rather, change should be thought of as a process that may take months or even years. 2. Many ‘behavioral change’ programs are characterized as lasting for a predetermined number of weeks and consisting of structured content. Such programs do not take into account the uniqueness of each client, and the subtle changes that often go unnoticed. Some clients will respond very positively and make significant changes. However, for those who do not, they are said to lack motivation and/or willpower. 3. We tend to acknowledge change has occurred when we see a change in behavior, e.g. a period of abstinence, leaving an unhealthy relationship. These are seen as successes. Key Points 5. The stages of change model suggests that change occurs along a continuum and therefore cannot be measured by one criteria alone, i.e. a change in a specific problem behavior. If we view change as a process then we can report positive changes each time an individual progresses from one stage to the next. Small steps constitute changes and should therefore be recognized and supported. 6. Since clients differ in their readiness to make changes Prochaska and DiClemente suggest matching interventions to the appropriate stage (or readiness). “Success, moreover, is defined not just by changing the behavior but by any movement toward change, such as a shift from one stage of readiness to another.” 7. There is an emphasis on the maintenance of change. Relapse is common and should not be seen as a sign of failure. Clients are encouraged to learn from their relapse. 8. A great deal of importance is placed on the decision making capability of the individual Practical Applications • Teaching case conceptualization and treatment planning in counselor education and supervision – Common concerns of student counselors in supervision: • • • • • • • • • • • “I don’t know what else to do with this client” “I feel like I do not know enough techniques” “I want to be prepared and have a diverse number of tools to draw upon” “The client is stuck, I am stuck, I don’t know where to go” “I am exhausted, she or he, won’t budge.” Counselors need to become aware of when they are working harder than their clients Counselors may get into difficulties if they rely too heavily on theoretical techniques and attempt to draw from their “bag of tricks”. Eventually someone will throw a spanner in the works. Student counselors will benefit from learning about the stages of change because it explains the process of change. More emphasis is placed on the client, which will help alleviate some of the pressure counselors feel. Counselors can use the model to teach clients about the stages of change, and thus set the tone for future counseling sessions. All of the above can then be used to create a collaborative treatment plan based on the clients current position Integration of Major Therapy Systems within the Transtheoretical Framework Levels Contemplation Precontemplation Preparation Action Symptom/ Situational Behavioral Maladaptive cognitions Alderian Rational Emotive Cognitive Behavioral Rational Emotive Cognitive Behavioral Interpersonal Sullivanian Therapy Couples Couples Communication Communication Transactional analysis Transactional analysis Family System Conflicts Strategic Bowenian Bowenian Structural Intrapersonal Conflicts Psychoanalytic Existential Existential Gestalt Gestalt Conflicts Maintenance Structural Motivational Interviewing • A counseling style that is derived from the field of addictions counseling. • Brief intervention format. • Six critical elements necessary for successful brief interventions (the acronym FRAMES) • • • • • • Feedback emphasizing the clients Responsibility for change offering Advice provide a Menu of alternative treatment options demonstrate Empathy reinforce client’s optimism; Self-Efficacy. Miller & Sanchez, 1994 Motivational Interviewing • Motivational interviewing is guided by several principles: • • • • • • • Avoiding argumentation Rolling with resistance Expressing empathy Developing discrepancies Supporting self-efficacy Counselors avoid harsh confrontations MI counselors emphasize the need for change and increase confidence and hope that change can occur. Lewis & Osborn, 2004 Stage 1: Precontemplation Description Techniques Questions to ask Individual’s in the precontemplation stage are often viewed as unmotivated clients who are not ready for change. They may not believe they have a problem and state they do not intend on making any changes in the near future (not within the next 6 months). Their lack of motivation to change may be as a result of failed prior attempts to change their high risk behaviors. It is also possible these individual’s may not fully realize the negative consequences of their behavior. The goal of the precontemplation stage is to move the client into contemplation, i.e. to help client begin to think about negative consequences of their behavior and consider change as a possibility • Validate clients feelings • "What would and thoughts regarding have to happen lack of readiness for you to know that this is a • Make client aware it is problem?“ her/his decision whether or not to change. • "What would you consider as • Encourage re-evaluation of warning signs current behavior that would let • Self exploration, not action, you know that should be the goal this is a • Raise awareness and problem?" doubt • “What things • Explain and personalize have you tried the risk in the past to change?” Adapted from: The National Center for Biotechnology Information: TIP 35: Enhancing Motivation for Change in Substance Abuse Treatment: http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat5.chapter.61302 Precontemplation: Strategies • Use self motivational statements with questions such as: – “How does this concern you?” – “What do you think will happen to you if you do not make any changes?” – “What has your alcohol use prevented you from doing?” • If client is reluctant, try asking – "What would have to happen for you to know that this is a problem?“ – "What would you consider as warning signs that would let you know that this is a problem?“ • • • • • Try not to assume client has a substance abuse problem. Instead, start from the viewpoint ‘there is a possibility substance abuse is a problem for you” If subject seems willing, offer feedback from test results, such as the SOCRATES. (but ask, ‘what do these results say to you?’) Try not to come from the ‘counselor as expert’ point of view. If client is willing, explain the concepts behind the stages of change model. Involve them in the process. Ask subject what they would like the next step to be. Moving from Precontemplation to Contemplation • There is a myth...in dealing with serious health-related addictive...problems, that more is always better. More education, more intense treatment, more confrontation will necessarily produce more change. Nowhere is this less true than with precontemplators. More intensity will often produce fewer results with this group. So it is particularly important to use careful motivational strategies, rather than to mount high-intensity programs...that will be ignored by those uninterested in changing the...problem behavior... We cannot make precontemplators change, but we can help motivate them to move to contemplation. (DiClemente, 1991) • Individual’s in the precontemplation stage rarely show for treatment by choice. Most are required to attend treatment for one reason or another. They may truly believe their substance use is not a problem. One goal is therefore to create doubt within the client, such that they may question their risky behaviors. When you first meet with client: • – – – • Establish rapport and trust Explore events that precipitated treatment entry Commend clients for coming "Why do you think your probation officer believes you have a problem?" This enables the client to express the problem from the perspective of the referring party. It also provides you with an opportunity to encourage the client to acknowledge any truth in the other party's account (Rollnick et al., 1992a). Source: http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat5.section.61822 Moving from Precontemplation to Contemplation Readiness Ruler: (Source: Rollnick) The simplest way to assess the client's willingness to change is to use a Readiness Ruler or a 1 to 10 scale, on which the lower numbers represent no thoughts about change and the higher numbers represent specific plans or attempts to change. Ask the client to indicate a best answer on the ruler to the question, "How important is it for you to change?" or, "How confident are you that you could change if you decided to?" Precontemplators will be at the lower end of the scale, generally between 0 and 3. You can then ask, "What would it take for you to move from an x (lower number) to a y (higher number)?" Moving from Precontemplation to Contemplation • • Description of a typical day Another, less direct, way to assess readiness for change, as well as to build rapport and encourage clients to talk about substance use patterns in a nonpathological framework, is to ask them to describe a typical day. This approach also helps you understand the context of the client's substance use. For example, it may reveal how much of each day is spent trying to earn a living and how little is left to spend with loved ones. By eliciting information about both behaviors and feelings, you can learn much about what substance use means to the client and how difficult--or simple--it may be to give it up. Substance use is the most cohesive element in some clients' lives, literally providing an identity. For others it is powerful biological and chemical changes in the body that drive continued use. Alcohol and drugs mask deep emotional wounds for some, lubricate friendships for others, and offer excitement to still others. Start by telling the client, "Let's spend the next few minutes going through a typical day or session of...use, from beginning to end. Let's start at the beginning." Clinicians experienced in using this strategy suggest avoiding any reference to "problems" or "concerns" as the exercise is introduced. Follow the client through the sequence of events for an entire day, focusing on both behaviors and feelings. Keep asking, "What happens?" Pace your questions carefully, and do not interject your own hypotheses about problems or why certain events transpired. Let clients use their own words and ask for clarification only when you do not understand particular jargon or if something is missing Source: (Rollnick et al., 1992a). Moving from Precontemplation to Contemplation • Provide Information About the Effects and Risks of Substance Use Provide basic information about substance use early in the treatment process if clients have not been exposed to drug and alcohol education before and seem interested. Tell clients directly, "Let me tell you a little bit about the effects of..." or ask them to explain what they know about the effects or risks of the substance of choice. To stay on neutral ground, illustrate what happens to any user of the substance, rather than referring just to the client. Also, state what experts have found, not what you think happens. As you provide information, ask, "What do you make of all this?" • It is sometimes helpful to describe the addiction process in biological terms to persons who are substance dependent and worried that they are crazy. Understanding facts about addiction can increase hope as well as readiness to change. For example, "When you first start using substances, it provides a pleasurable sensation. As you keep using substances, your mind begins to believe that you need these substances in the same way you need life-sustaining things like food--that you need them to survive. You're not stronger than this process, but you can be smarter, and you can regain your independence from substances.“ Source: (Rollnick et al., 1992a). Stage 2: Contemplation Description Techniques Questions to ask During the contemplation stage, individuals are ambivalent about changing. They are aware their behavior is resulting in negative consequences and may be considering making a change. However, no commitment has been made to take action. One could say these individuals are ‘sitting on the fence’. Contemplation is characterized by ambivalence and feelings of being ‘stuck’. • Make client aware it is her/his decision whether or not to change. • Encourage evaluation of pros and cons of behavior change with the goal of helping tip the balance toward change. • Identify and promote new, positive outcome expectations • Have client state their next step • "What are the pros and cons for not changing? • What are the pros and cons (costs/benefits) for changing? • Why do you want to change at this time?" • "What would keep you from changing at this time?" • "What are the barriers today that prevent you from changing?" • "What things (people, programs and behaviors) have helped in the past?" • "What would help you at this time?" Contemplation: Strategies Figure 8-3 Deciding To Change: Use ‘decisional balance’ techniques. Changing Not Changing Benefits •Increased control over my life •Support from family and friends •Decreased job problems •Financial gain •Improved health Benefits •More relaxed •More fun at parties •Don't have to think about my problems Costs •Increased stress/anxiety •Feel more depressed •Increased boredom •Sleeping problems Costs •Disapproval from friends and family •Money problems •Could lose my job •Damage to close relationships •Increased health risks Source: Sobell et al., 1996b. http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat5.table.62797 Contemplation Strategies: Cost Benefit Analysis Scale Source: Davis & Osborn (2000) Costs of Use Benefits of Use Benefits Costs Costs of Sobriety Benefits of Sobriety Costs Benefits Stage 3: Preparation Description Techniques Individuals in the • Identify and assist in preparation stage intend problem solving, e.g. to take action (within the identify barriers and next month) and may brainstorm solutions already have had • Help identify client previous failed attempts resources such as at trying to change. social supports Some may have already • Encourage and ‘tested the waters’ by support small initial engaging in small steps changes, e.g. going without a drink for a night. Client may have an initial plan. Questions to ask • What barriers do see ahead, and how can you minimize or eliminate them? • Who can you turn to for support? • What kind of support do you feel you need the most, and where can you get this support? Preparation: Activities • • • Identify client’s needs/wants/desires Emphasis is on outlining and developing plans in order to break the pattern of substance abuse, and find other ways of meeting clients needs. Goal Setting – Miracle question – Where do you want to be 6 months, 1 year, 5 years from now? What will life look like for you? • • • • • Encourage client to come up with their own plans, and have them state specifically how they will achieve them. Identify alternative ways in which to meet needs. Identify areas of support that can be utilized. Commend client for deciding to change because they always have the option not to. Create an action plan Have client state their next step. Moving Clients From Contemplation to Preparation • Do not rush your clients into decision making. • Emphasize client control: "You are the best judge of what will be best for you." • Acknowledge and normalize ambivalence. • Examine options rather than a single course of action. • Describe what other clients have done in a similar situation. • Present information in a neutral, non personal manner. • Remember that inability to reach a decision to change is not a failed consultation. • Make sure that your clients understand that resolutions to change often break down; clients should not avoid future contact with you if things go wrong. • Expect fluctuations in your client's commitment to change--check commitment regularly and express empathy concerning the client's predicaments. Source: (Rollnick et al., 1992a.) Stage 4: Action Description Techniques Individuals are actively • Focus on restructuring changing their behavior cues and social and/or environment in a support positive manner in order • Bolster self-efficacy for to address their dealing with obstacles problem(s). Client has • Combat feelings of changed behavior for loss and reiterate less than 6 months. long-term benefits Questions to ask •Use strategies listed for Preparation Stage if necessary. •Continue consolidating client’s motivation for change •What actions have you taken? •What has helped/not helped? •What might you do to replace things that have not helped? Action: Strategies • Elicit client’s sources of support • Understand client is trying to fill a void having given up their substance of choice. • How can this void be filled with healthier behaviors so that they client can meet their needs Stage 5: Maintenance Description Techniques Maintenance involves the individual • Conducting a Functional Analysis proactively working to prevent • Developing a Coping Plan relapse. Change is continuous, it • Plan for follow-up support does not end at Maintenance. In addition to handling problems that can Triggers interrupt treatment prematurely, work to stabilize actual change in the problem behavior. This requires considerable interactive planning, including conducting a functional analysis, developing a coping plan, and ensuring family and social support. Start with identifying Triggers and Effects Effects Maintenance Strategies: Functional Analysis Conducting a Functional Analysis: Although a functional analysis can be used at various points in treatment, it can be particularly informative in preparing for maintenance. A functional analysis is an assessment of the common antecedents and consequences of substance use. Through functional analysis, you help clients understand what has "triggered" them to drink or use drugs in the past and the effects they experienced from using alcohol or drugs. With this information, you and your clients can then work on developing coping strategies to maintain abstinence. "Tell me about situations in which you have been most likely to drink or use drugs in the past, or times when you have tended to drink or use more. These might be when you were with specific people, in specific places, or at certain times of day, or perhaps when you were feeling a particular way." Make sure to use the past tense because the present or future tense may unsettle currently abstinent clients. As your client responds, listen reflectively to make sure that you understand. Under the Triggers column, write down each antecedent. Then ask, "When else in the past have you felt like drinking or using drugs?" and record each response After the client seems to have exhausted the antecedents of substance use, ask about what the client liked about drinking or using drugs. Here you are trying to elicit the client's own perceptions or expectations from substance use, not necessarily the actual effects. Miller and Pechacek, 1987 Maintenance Strategies: Functional Analysis • Once the client has finished giving antecedents and consequences, you can point out how a certain trigger can lead to a certain effect. First, pick out one item from the Triggers column and one from the Effects column that clearly seem to go together. Then ask the client to identify pairs, letting the client draw connecting lines on the paper or blackboard. • For trigger items that have not been paired, ask the client to tell you what alcohol or drug use might have done for her in that situation, and draw a line to the appropriate item in the Effects column. Sometimes there is no corresponding item in the Effects column, which suggests that something has to be added. Then do the same thing for the Effects column. It is not necessary, however, to pair all entries. • With this information, you can develop maintenance strategies. Point out that some of the pairs your client identified are common among most users. Next, you can say that if the only way a client can go from the Triggers column to the Effects column is through substance use, then the client is psychologically dependent on it. Then make clear that freedom of choice is about having options-different ways--of moving from the Triggers to the Effects column. You can then review the pairs, beginning with those the client finds most important, and develop a coping plan that will enable the client to achieve the desired effects without using substances Miller and Pechacek, 1987 Maintenance Strategies: Coping Plans Coping Strategies: Coping strategies are not mutually exclusive (i.e., different ones can be used at different times) and not all are equally good (i.e., some more than others involve getting close to trigger situations). The point is to brainstorm, involve the client, reinforce successful application of coping strategies, and consider it as a learning experience if a particular strategy fails. Example #1: Client X typically uses cocaine whenever his cousin, who is a regular user, drops by the house. Coping strategies to consider would include (1) call the cousin and ask him not to come by anymore, (2) call the cousin and ask him not to bring cocaine anymore when he visits, (3) if there is a pattern to when the cousin comes, plan to be out of the house at that time, or (4) if someone else lives in the house, ask them to be present during the cousin's visit. Example #2: Client Y typically uses cocaine when she goes out for the evening with a particular group of friends, one of whom often brings drugs along. She is particularly vulnerable when they all drink alcohol. Coping strategies to consider might include (1) go out with a different set of friends, (2) go along with this group only for activities that do not involve drinking, (3)leave the group as soon as drinking seems imminent, (4) tell the supplier that she is trying to stay off cocaine and would appreciate not being offered any, (5)ask all her friends, or one especially close friend, to help her out by not using when she is around or by telling the supplier to stop offering it to her, or (6)take disulfiram [Antabuse] to prevent drinking. Example #3: Client Z typically uses cocaine when feeling tired or stressed. Coping strategies might include (1) scheduling activities so as to get more sleep at night, (2)scheduling activities so as to have 1 hour per day of relaxation time, (3)learning and practicing specific stress relaxation techniques, or (4)learning problem-solving techniques that can reduce stressful circumstances. The Processes of Behavior Change: How clients can move from one stage to the next The processes of change are the activities clients engage in to progress through the stages of change. (Prochaska, 1997) 1. Consciousness-raising —finding and learning new facts and suggestions supporting the change (e.g., reading a book; watching a TV show; talking with a friend, teacher, or doctor) 2. Dramatic Relief — experiencing and expressing negative feelings about one's problems such as worry or fear (e.g., communicating with a friend, partner, counselor; writing in a journal) 3. Self Re-evaluation — realizing that the behavioral change is part of one's identity (e.g., seeing yourself as a non-smoker or a fit person) 4. Environmental Re-evaluation — assessing how one's problem affects the physical environment (e.g., realizing that second-hand smoke may affect nonsmoking children and partners or even pets) 5. Self Liberation — choosing and committing to act on a belief that change is possible (e.g., making a New Year's resolution); accepting responsibility for changing. The Processes of Behavior Change: How clients can move from one stage to the next (Prochaska, 1997) 6. Counter-conditioning — substituting healthier alternatives for problem behaviors (e.g., using relaxation or meditation techniques instead of eating to deal with stress) 7. Stimulus Control — avoiding triggers and cues (e.g., avoiding bars, friends who still smoke, dessert parties) 8. Contingency Management — increasing the rewards of positive behavioral change and decreasing the rewards of the unhealthy behavior (e.g., buying new clothes after losing weight instead of eating dessert) 9. Social Liberation — societal support for healthier behaviors (e.g., smoke-free workplaces; discussions about safer sex in school and communities) 10. Helping Relationships — seeking and using a strong support system of family, friends, and co-workers.1 Stages of Change in Which Change Processes are Most Emphasized Individual treatment plans can be designed by identifying the stage of change a client is currently experiencing, and making use of the processes of change associated with that stage. (Prochaska, 1997) Determining a Client’s Stage of Change using SOCRATES The Stages of Change Readiness and Treatment Eagerness Scale (Miller & Tonigan) “The Stages of Change Readiness and Treatment Eagerness Scale was originally developed as a parallel measure of the stages of change described by Prochaska and DiClemente with item content specifically focused on problem drinking.” Miller, Tonigan (1996) p. 82 • Contains 19 items • Client responds based on a lickert scale from: (1 - NO! Strongly Disagree) to (5 - YES! Strongly Agree) • 10 minutes to complete • Reports on 3 factors – Recognition – Ambivalence – Taking Steps • SOCRATES in pdf format • SOCRATES in Excel Format Source: http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat5.section.62203#62297 Solution-Focused Goal Setting • When determining goals, a solution-focused frame can create measurable, achievable goals for each stage that the client is in: – – – – – – State the goal POSITIVELY State the goal in PROCESS form (how will it be done) State the goal in the HERE and NOW State the goal as SPECIFICALLY as possible State the goal as the client having CONTROL State the goal in the client’s LANGUAGE From Walter & Peller, 1992 Determine the stage of change: References Davis, T. E. & Osborn, C. J. (2000) The solution focused school counselor: Shaping professional practice. Philadelphia, PA: Accelerated Development. DiClemente, C.C. (1991). Motivational interviewing and the stages of change. In W.R. Miller & S. Rollnick (Eds.) Motivational interviewing: Preparing people to change addictive behavior (pp. 191-202). New York: Guilford Press. Lewis, T.F., & Osborn, C.J. (2004). Solution-focused counseling and motivational interviewing: A consideration of confluence. Journal of Counseling & Development, 82, 38-48. Miller, W.R., & Pechacek, T.F.(1987). New roads: Assessing and treating psychological dependence. Journal of Substance Abuse Treatment,4, 73-77. Miller, W.R., Tonigan, J.S., Montgomery, H.A., et al. (1990). Assessment of client motivation to change: Preliminary validation of the SOCRATES (Rev) instrument. Albuquerque , NM: University of New Mexico Miller, W.R., & Tonigan, J.S. (1996). Assessing drinkers' motivation for change: The Stages of Change Readiness and Treatment Eagerness Scale (SOCRATES). Psychology of Addictive Behaviors 10, 81-89. References continued Miller, W.R., & Sanchez, V.C.(1994). Motivating young adult’s for treatment and lifestyle change. In G.Howard (Ed.), Issues in alcohol use and misuse by young adults (pp. 55-81). Notre Dame, IN: University of Notre Dame Press. Miller, W. R., TIP 35: Enhancing Motivation for Change in Substance Abuse Treatment Retrieved from http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat5.chapter.61302 Prochaska, J.O., & DiClemente, C.C. (1982). Transtheoretical therapy: Toward a more integrative model of change. Psychotherapy: Theory, Research and Practice, 19, 276-287. Prochaska, J.O.,& DiClemente, C.C.(1984).The transtheoretical approach: Crossing traditional boundaries of therapy. Homewood, IL: Dow Jones-Irwin. Prochaska, J.O., & DiClemente, C.C. (1992). The transtheoretical approach. In J.C. Norcross & M.R. Goldfried (Eds.) Handbook of psychotherapy integration. NY: Basic Books. References continued Prochaska, J.O., Redding, C.A., & Evers, K.E.(1997). The transtheoretical model and stages of change. In K. Glanz, F.M. Lewis, & B.K. Rimer (Eds.), Health nd behavior and health education: Theory, research, and practice (2 ed.) San Francisco: Jossey-Bass. Rollnick, S., Heather, N.,& Bell, A.(1992). Negotiating behavior change in medical settings: The development of brief motivational interviewing. J ournal of Mental Health,1, 25-37. Sobell, L.C., Cunningham, J.A., Sobell, M.B., Agrawal, S., Gavin, D.R., Leo, G.I., & Singh, K.N.(1996). Fostering self-change among problem drinkers: A proactive community intervention. Addictive Behaviors 21, 817-833. Walter, J.L. & Peller, J.E. (1992). Becoming solution focused in brief therapy. Levittown, PA: Brunner/Mazel.