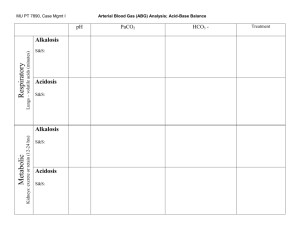
Powerpoint slide
advertisement

Lawrence Martin, M.D. Clinical Professor of Medicine Case Western Reserve University School of Medicine Cleveland, OHIO USA larry.martin@roadrunner.com September 17, 2009 Because your understanding the PaCO2 equation will: Save lives! Improve patient care! Help wean patients off the ventilator! Shorten length of stay! PaCO2 Equation: PaCO2 reflects ratio of metabolic CO2 production (VCO2) to alveolar ventilation (VA) PaCO2 = VCO2 x 0.863 ------------------VA VCO2 = CO2 production VA = VE – VD VE = minute (total) ventilation = f (tidal volume) VD = dead space ventilation = f (dead space volume) 0.863 converts VCO2 and VA units to mm Hg PaCO2 Condition in blood State of alveolar ventilation > 45 mm Hg Hypercapnia Hypoventilation 35 - 45 mm Hg Eucapnia Normal ventilation < 35 mm Hg Hypocapnia Hyperventilation PaCO2 Equation: PaCO2 reflects ratio of metabolic CO2 production (VCO2) to alveolar ventilation (VA) PaCO2 = VCO2 x 0.863 ------------------VA VCO2 = CO2 production VA = VE – VD VE = minute (total) ventilation = f (tidal volume) VD = dead space ventilation = f (dead space volume) 0.863 converts VCO2 and VA units to mm Hg Normal Resting VCO2 = 200 ml/minute f(tidal volume) = 12 (500 ml) = 6 l/min f(dead space vol.) = 12 (150 ml) = 1.80 l/min VA = 6 – 1.80 = 4.2 l/min 200 x 0.863 PaCO2 = ----------------4.2 = 41 mm Hg PaCO2 Equation: PaCO2 reflects ratio of metabolic CO2 production (VCO2) to alveolar ventilation (VA) PaCO2 = VCO2 x 0.863 ------------------VA VCO2 = CO2 production VA = VE – VD VE = minute (total) ventilation = f (tidal volume) VD = dead space ventilation = f (dead space volume) 0.863 converts VCO2 and VA units to mm Hg Rapid Breathing, normal tidal volume VCO2 = 200 ml/minute f(tidal volume) = 24 (500 ml) = 12 l/min f(dead space vol.) = 24 (150 ml) = 3.60 l/min VA = 12 – 3.60 = 8.4 l/min 200 x 0.863 PaCO2 = ----------------8.4 = 20.5 mm Hg PaCO2 Equation: PaCO2 reflects ratio of metabolic CO2 production (VOC2) to alveolar ventilation (VA) PaCO2 = VCO2 x 0.863 ------------------VA VCO2 = CO2 production VA = VE – VD VE = minute (total) ventilation = f (tidal volume) VD = dead space ventilation = f (dead space volume) 0.863 converts VCO2 and VA units to mm Hg Rapid Breathing, Shallow Tidal Volume VCO2 = 200 ml/minute f(tidal volume) = 20 (300 ml) = 6 l/min f(dead space vol.) = 20 (150 ml) = 3.00 l/min VA = 6 – 3 = 3 l/min 200 x 0.863 PaCO2 = ----------------3 = 57.5 mm Hg PaCO2 Equation: PaCO2 reflects ratio of metabolic CO2 production (VCO2) to alveolar ventilation (VA) PaCO2 = VCO2 x 0.863 ------------------VA VCO2 = CO2 production VA = VE – VD VE = minute (total) ventilation = f (tidal volume) VD = dead space ventilation = f (dead space volume) 0.863 converts VCO2 and VA units to mm Hg Rapid breathing, increased dead space (severe COPD) VCO2 = 200 ml/minute f(tidal volume) = 16 (500 ml) = 8 l/min f(dead space vol.) = 16 (300 ml) = 4.80 l/min VA = 8 – 4.8 = 3.2 l/min 200 x 0.863 PaCO2 = ----------------- = 54 mm Hg 3.2 PaCO2 is the center of the blood gas universe; without understanding PaCO2 you can’t understand oxygenation or acid-base balance. Oxygenation Acid-Base PAO2 = FIO2 (BP-47) – 1.2 (PCO2) HCO3 pH ~ -----------PaCO2 PaO2 PaCO2 = VCO2 x .863 -------------------VA where VA = VE - VD Note: PaCO2 is from ABGs. HCO3 is calculated from ABG measurement of pH and PaCO2 or measured in venous blood as part of electrolytes. When measured in venous blood it is variously labeled ‘bicarbonate’, ‘HCO3’ or ‘CO2’ (the latter NOT to be confused with PaCO2). Arterial blood – blood gases Venous blood - BMP PaCO2 is the center of the blood gas universe. . pH PaO2 PaCO2 HCO3 SaO2 You can’t learn this material from a lecture!! Review: www.lakesidepress.com/pulmonary/index-phys.html index to web sites on pulmonary physiology www.lakesidepress.com/ABGQuiz2009-Questions.htm multiple-choice blood gas quiz www.lakesidepress.com/pulmonary/papers/eq/tablecontents.html 4 Most Important Equations in Clinical Practice www.lakesidepress.com/pulmonary/ABG/MixedAB.htm Diagnosing mixed acid-base disorders www.lakesidepress.com/pulmonary/ABG/PO2.htm PaO2, SaO2 & CaO2 – What’s the Difference? Hypercapnia – PaCO2 > 45 mm Hg PaCO2 VCO2 x 0.863 = -----------------VA where VA = VE – VD Hypercapnia is a serious respiratory problem. The PaCO2 equation shows that the only physiologic reason for elevated PaCO2 is inadequate alveolar ventilation (VA) for the amount of metabolic CO2 production (VCO2). Since alveolar ventilation (VA) equals minute ventilation (VE) minus dead space ventilation (VD), hypercapnia can arise from insufficient VE, increased VD, or a combination of both. Hypercapnia (cont) PaCO2 = VCO2 x 0.863 -----------------VA where VA = VE – VD VA = f(tidal vol.) – f(dead space vol.) Examples of inadequate VE leading to decreased VA and hypercapnia: sedative drug overdose; respiratory muscle paralysis; central hypoventilation Examples of increased VD leading to decreased VA and hypercapnia: chronic obstructive pulmonary disease; severe restrictive lung disease (with shallow, rapid breathing) Dangers of Hypercapnia Besides indicating a serious derangement in the respiratory system, elevated PaCO2 poses a threat for three reasons: An elevated PaCO2 will lower the PAO2 (see Alveolar gas equation) and as a result will lower the PaO2. 2) An elevated PaCO2 will lower the pH (see Henderson-Hasselbalch equation) and as result lead to acidosis. 3) The higher the baseline PaCO2, the more it will rise for a given fall in alveolar ventilation, e.g., a given decrease in VA will raise the PaCO2 more when PaCO2 is 50 mm Hg than when it is 40 mm Hg. 1) Dangers of Hypercapnia – lowers PAO2 & PaO2 An elevated PaCO2 will lower the PAO2 and as a result will lower the PaO2 Alveolar Gas Equation determines the alveolar PO2 (PAO2). PAO2 is one of two main factors that determine PaO2. (The other is ventilation-perfusion relationships within in the lungs.) PAO2 = FIO2 (BP-47) – 1.2 (PaCO2) PaO2 Dangers of Hypercapnia – lowers PAO2 & PaO2 An elevated PaCO2 will lower the PAO2 and as a result will lower the PaO2 PAO2 = FIO2 (BP-47) – 1.2 (PaCO2) =.21 (760-47) – 1.2 (40) = 150 – 48 = 102 PAO2 = FIO2 (BP-47) – 1.2 (PaCO2) =.21 (760-47) – 1.2 (60) = 150 – 72 = 78 Assuming 10 mm (A-a) O2 difference, PaO2 = 92 mm Hg Assuming 10 mm (A-a) O2 difference, PaO2 = 68 mm Hg Dangers of Hypercapnia – lowers the pH An elevated PaCO2 will lower the pH, as predicted by the Henderson-Hasselbalch Equation. HCO3 pH ~ -----------PaCO2 Dangers of Hypercapnia – lowers the pH An elevated PaCO2 will lower the pH, as predicted by the Henderson-Hasselbalch Equation. HCO3 pH ~ -----------PaCO2 Normal 24 mEq/l 7.40 ~ -----------40 mm Hg Respiratory Acidosis 24 mEq/l 7.23 ~ -----------60 mm Hg Basic Metabolic Panel from venous blood (BMP) Na+ K+ Cl HCO3 BUN Creatinine 140 4.0 95 35 20 1.1 mEq/L mEq/L mEq/L mEq/L mg% mg% HCO3 and PaCO2 are 2 of 3 components in HCO3 the H-H equation: pH ~ -----------PaCO2 What does HCO3 by itself reveal about PaCO2? Any venous HCO3 can reflect virtually any value of PaCO2. Shown here is venous HCO3 of 35 mEq/L , plotted on graph of H-H equation. The range of possible PaCO2 values is below 20 to above 100. Abbreviated H-H equation: HCO3 pH ~ -----------PaCO2 Knowing just one parameter doesn’t tell you the acid-base state; you need at least two of the three values in H-H equation! Dangers of Hypercapnia – less reserve if there is further hypoventilation Effect of 1 liter decreases in alveolar ventilation on PaCO2, when VCO2 = 200 ml/min VCO2 x 0.863 PaCO2 = --------------VA A one-liter decrease in VA when PaCO2 is 40 mm Hg will increase PaCO2 to 52 mm Hg. The next one-liter decrease in VA will increase PaCO2 to 75 mm Hg… And the next 1 liter decrease in VA will increase PaCO2 to 133 mm Hg! PaCO2 High PaCO2 increases the slope of change for any further decrease in VA High PaCO2 is dangerous! VA (l/min) Dangers of Hypercapnia – summary PaCO2 of 60 mm Hg is not ‘just 50% higher’ than 40mm Hg. A high PaCO2 also: Lowers PaO2 at any given Bar. Press. PAO2 = PIO2 – 1.2(PaCO2) PAO2 > PaO2 Makes patient acidotic pH ~ HCO3 PaCO2 Increases the slope of change for any further decrease in VA. VCO2 x 0.863 PaCO2 = ------------VA For VCO2 of 200 and 300 ml/min PaCO2 Graph of: VA (l/min) You cannot assess PaCO2 clinically – Why not? 50-year-old man with COPD: respiratory rate 35/minute; agitated BP 170/104 mm Hg Pulse 105/minute Good breath sounds Is he hyperventilating? Hypoventilating? No way to tell clinically. At bedside can’t determine if PaCO2 high or low because: VCO2 x 0.863 PaCO2 = -----------------------VA = f(tidal vol. – f(dead space vol.) You don’t know: - VCO2 - tidal volume - dead space volume Trying to assess PaCO2 clinically can lead to fatal or near fatal errors! Case – 73 yo woman in hospital (continued) Intern called to bedside at 11 pm because “she is agitated.” She was previously calm all day. Check of her lab work shows that 2 days earlier, on hospital admission, her venous HCO3 was 35 mEq/L (normal up to 29). Respiratory rate 20 (mild tachypnea). Lungs clear. Intern assess “hypreventilation” and prescribes Valium to “calm her down.” 45 minutes later patient stops breathing, is emergently intubated. (continued) ERROR Intern didn’t think of hypoventilation in setting of agitation. VCO2 PaCO2 =--------VA = f(tidal vol.) – f(dead space vol.) The only parameter known to intern was frequency of breathing (fast). Knowing just ‘f’, it is impossible to reliably gauge if patient is hyperventilating or hypoventilating. High HCO3 (not noted by intern) was certainly consistent with latter. Without check of ABG, Valium should not have been given! Hyperventilating? Hypoventilating? Cannot reliably assess PaCO2 clinically PaCO2 is determined only by factors in the PaCO2 equation: VCO2 x 0.863 PaCO2 = -------------------VA = f(tidal vol. – f(dead space vol.) VCO2 = metabolic CO2 production/min VA = alveolar ventilation f = frequency of breathing 0.863 converts units to mm Hg The ONLY clinical parameter in PaCO2 equation is frequency of breathing!!! There is nothing in PaCO2 equation about respiratory effort, mental status, body habitus, etc. If all you know at bedside is resp. rate, you can’t possibly discern patient’s PaCO2!! You cannot determine at bedside if patient’s PaCO2 is high or low. PaCO2 is key to the blood gas universe; without understanding PaCO2 you can’t understand oxygenation or acid-base. Oxygenation PAO2 = FIO2 (BP-47) – 1.2 (PCO2) Acid-Base HCO3 pH ~ -----------PaCO2 PaO2 PaCO2 = VCO2 x .863 -------------------VA where VA = VE = VD = f(VT) – f(VD) PaCO2 and Alveolar Ventilation: Test Your Understanding 1. What is the PaCO2 of a patient with respiratory rate 24/min, tidal volume 300 ml, dead space volume 150 ml, CO2 production 300 ml/min? The patient shows some evidence of respiratory distress. . PaCO2 and Alveolar Ventilation: Test Your Understanding 1. What is the PaCO2 of a patient with respiratory rate 24/min, tidal volume 300 ml, dead space volume 150 ml, CO2 production 300 ml/min? The patient shows some evidence of respiratory distress. First, you must calculate the alveolar ventilation. . VE = 24 x 300 = 7.2 L/min VD = 24 x 150 = 3.6 L/min VA = 3.6 L/min. Then 300 ml/min x .863 PaCO2 = ----------------------3.6 L/min PaCO2 = 71.9 mm Hg PaCO2 and Alveolar Ventilation: Test Your Understanding 2. What is the PaCO2 of a patient with respiratory rate 10/min, tidal volume 600 ml, dead space volume 150 ml, CO2 production 200 ml/min? The patient shows some evidence of respiratory distress. PaCO2 and Alveolar Ventilation: Test Your Understanding 2. What is the PaCO2 of a patient with respiratory rate 10/min, tidal volume 600 ml, dead space volume 150 ml, CO2 production 200 ml/min? The patient shows some evidence of respiratory distress. VA = VE – VD = 10(600) - 10(150) = 6 - 1.5 = 4.5 L/min 200 ml/min x .863 PaCO2 = ---------------------- = 38.4 mm Hg 4.5 L/min PaCO2 and Alveolar Ventilation: Test Your Understanding 3. A man with severe chronic obstructive pulmonary disease exercises on a treadmill at 3 miles/hr. His rate of CO2 production increases by 50% but he is unable to augment alveolar ventilation. If his resting PaCO2 is 40 mm Hg and resting VCO2 is 200 ml/min, what will be his exercise PaCO2? PaCO2 and Alveolar Ventilation: Test Your Understanding 3. A man with severe chronic obstructive pulmonary disease exercises on a treadmill at 3 miles/hr. His rate of CO2 production increases by 50% but he is unable to augment alveolar ventilation. If his resting PaCO2 is 40 mm Hg and resting VCO2 is 200 ml/min, what will be his exercise PaCO2? Exercise increases metabolic CO2 production. People with a normal respiratory system are always able to augment alveolar ventilation to meet or exceed the amount of VA necessary to excrete any increase in CO2 production. As in this example, patients with severe COPD or other forms of chronic lung disease may not be able to increase their alveolar ventilation, resulting in an increase in PaCO2. This patient’s resting alveolar ventilation is PaCO2 = VCO2 x .863 --------------VA 200 ml/min x .863 VA = 4.32 L/min = ----------------------40 mm Hg Since CO2 production increased by 50% and alveolar ventilation not at all, his exercise PaCO2 is 300 ml/min x .863 -------------------------- = 59.9 mm Hg 4.32 L/min You can’t learn this material from a lecture!! Review: www.lakesidepress.com/pulmonary/index-phys.html index to web sites on pulmonary physiology www.lakesidepress.com/ABGQuiz2009-Questions.htm multiple-choice blood gas quiz www.lakesidepress.com/pulmonary/papers/eq/tablecontents.html 4 Most Important Equations in Clinical Practice www.lakesidepress.com/pulmonary/ABG/MixedAB.htm Diagnosing mixed acid-base disorders www.lakesidepress.com/pulmonary/ABG/PO2.htm PaO2, SaO2 & CaO2 – What’s the Difference?