MildTBI&Concussion
advertisement

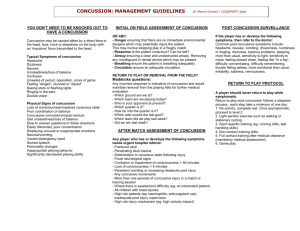
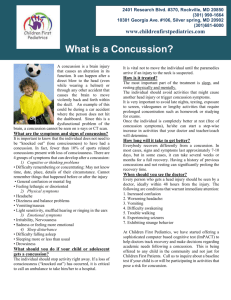
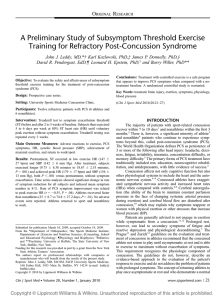
Disclaimer: This PowerPoint is a brief summary of PRELIMINARY RESEARCH. It is intended for educational purposes and not meant to be adopted as treatment protocol. Mild TBI & Concussion Assessment & Treatment Dr. Barry Willer University at Buffalo, Concussion Clinic NHL Buffalo Sabres Foundation Ontario Hockey Hockey Canada Salt Lake City Winter Olympics http://www.youtube.com/watch?v=xXl6LPIoXUg Definitions: o Concussion: - short-term alternation of consciousness due to a trauma - caused by movement of the brain inside the skull - involves metabolic changes - usually recovery within 2 weeks o Post Concussion Syndrome/Mild TBI - symptoms persist beyond 2 weeks - physiologic characteristics include: - ↑ HR - ↑ BP (diastolic during exercise) - ↑ HR variability (parasympathetic response) - ↑ cerebral blood flow during exercise Physiology metabolic chain reaction of brain neurochemical changes after concussion that produces an initial hypermetabolic state followed by a state of metabolic depression may explain why: some symptoms are delayed in onset or worsen over time some patients report symptom resolution before they demonstrate physical and cognitive homeostasis patients who are asymptomatic at rest can become symptomatic during physical or cognitive exertion Regulatory and Autoregulatory Physiological Dysfunction as a Primary Characteristic of Post Concussion Syndrome: Implications for Treatment John J. Leddy, Karl Kozlowski, Michael Fung, David R. Pendergast, and Barry Willer, NeuroRehabilitation 2007 How will our clients present? Headaches Photophobia Poor sleep Dizziness Post Concussion Syndrome (PCS) 5-10% of ppl who experience concussions will have symptoms that persist beyond 6 weeks. There is no known cause for persistent symptoms after a concussion. A prior history of concussions will increase the likelihood of PCS. The most common symptom is headache. Experiencing dizziness is the most definitive predictor of poor outcomes long-term. “Rest is best” theory (no exercise) Prescription of anti-depressants is the most common treatment. Quick Refresher Sympathetic Nervous System Parasympathetic Nervous System ↑ HR ↓ HR Pupils dilate Pupils contract Inhibits digestion Stimulates digestion Inhibits nasal secretions Causes nasal secretions Inhibits saliva production Stimulates liver/kidneys/gall bladder Inhibits liver/kidneys/gall bladder Causes constriction inside the lungs Stimulates sweating Causes piloerection Makes lungs dilate ↑ muscle strength i.e. “fight or flight” vs “rest and digest” Sympathetic Overdrive Imbalance between our sympathetic and parasympathetic nervous systems Parasympathetic system does not “kick in” Poor sleep hygiene Light sensitivity Exercise to Address PCS Rationale: the regulatory system responsible for maintaining cerebral blood flow, which may be dysfunctional in people with a concussion, can be restored to normal by controlled, graded symptom-free exercise. Subsymptom Threshold Exercise Training (SSTET) Dr. Willer advises only aerobic exercise for the treatment of PCS. http://www.medicalnewstoday.com/ releases/53995.php Cerebrovascular & Cardiovascular Benefits of Exercise ↑ PNS activity ↑ Autonomic regulation ↓ Depression EXERCISE Improved sleep Improved mood ↑ cerebral blood flow PCS vs Cervical Strain If a client is able to exercise to the point of exhaustion and their headache IMPROVES, they may have cervical strain. ↑ endorphins ↑ blood flow Muscles relax A heat pack on their neck should reduce their headache. Note: Cervical strain may cause dizziness due to the fact that our neck has both pain sensors and vestibular sensors. So What? Treadmill Test Speed = 3.4 mph Incline = 0% HR monitor Borg RPE Scale Record of symptom onset Ability to exercise to point of voluntary exhaustion w/out symptom exacerbation = “physiologically recovered” Clients respond well to “seeing” improvement Study Results: Symptom Reduction FIGURE 1. Athlete versus nonathlete improvement in mean number of daily symptoms (with 95% confidence intervals) by weeks of exercise treatment. Athletes completed treatment significantly faster than nonathletes. A Preliminary Study of Subsymptom Threshold Exercise Training for Refractory Post-Concussion Syndrome John J. Leddy, Karl Kozlowski, James P. Donnelly, David R. Pendergast, Leonard H. Epstein, and Barry Willer Clin J Sport Med Volume 20, Number 1, January 2010 References http://www.medicalnewstoday.com/releases/53995.php http://journals.lww.com/cjsportsmed/Fulltext/2011/03000/Reliabili ty_of_a_Graded_Exercise_Test_for.3.aspx Regulatory and Autoregulatory Physiological Dysfunction as a Primary Characteristic of Post Concussion Syndrome: Implications for Treatment John J. Leddy, Karl Kozlowski, Michael Fung, David R. Pendergast, and Barry Willer, NeuroRehabilitation 2007 A Preliminary Study of Subsymptom Threshold Exercise Training for Refractory Post-Concussion Syndrome John J. Leddy, Karl Kozlowski, James P. Donnelly, David R. Pendergast, Leonard H. Epstein, and Barry Willer Clin J Sport Med Volume 20, Number 1, January 2010 http://medicine.buffalo.edu/faculty/profile.html?ubit=bswiller http://concussion.buffalo.edu/ bswiller@buffalo.edu Questions?