Handout
advertisement

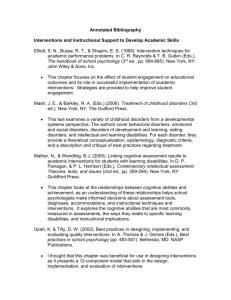
Navigating the New Environment for Addiction Treatment Steve Allen, PhD UC Berkeley Extension What is now The Past • • • • • 1970’s and 80’s: Private insurance often covered 28-day inpatient stays for 12 Step based Minnesota Model treatment. Public, government-funded treatment services also provided 28-day residential treatment, and even longer-term stays. A great many alcohol and drug counselors came into the profession via their own recoveries which began in such residential programs, and many of them have continued to work in these settings. Beginning in the 90’s, both insurance companies and public agencies began to question the need for residential programs, and began to extend more support to day treatment and intensive outpatient services. Many traditional programs then began to expand their services to include these new modalities. Counselors have continued to play large roles in these expanded services, often adapting the same techniques used in residential services. What is now The Past • Addiction treatment has always been segregated from the rest of healthcare, and almost always provided in separate specialty care addiction treatment programs. • Financing for addiction treatment was also separated from other healthcare coverage, typically “carved out” and managed separately from the larger healthcare plan. • Many private insurance plans have not covered addiction treatment at all. Over 80% of addiction treatment financing has come from government sources (Block grants, VA, etc.) • Whether public or private, coverage has always been restricted to only the most advanced and severe form of substance use problem: addiction. Coverage for less severe but far more common forms of substance use disorders has never been included. PPACA Basics • • • • • • • • Requires all Americans to purchase healthcare insurance, with subsidies provided to lower-income people. Requires all health plans and systems to cover ten “essential services”—including “substance use disorders.” (We’ll come back to that term later.) No annual or lifetime dollar limits on coverage of any of these essential services No denial of coverage for pre-existing conditions, and no dropping of those who acquire a chronic condition. Assures portability of of insurance when changing jobs. Family coverage can include all children through age 26. Increases primary prevention services—available to all insured with no co-pays; 100% Federally funded. Greatly expands eligibility for Medicaid. (We’ll come back to that later too.) Substance Use Disorders under PPACA • • • Requires health insurers to cover, and healthcare organizations to provide, prevention, screening and brief interventions for the full spectrum of substance use disorders, not just “addiction.” Care for these disorders must have the same type, duration, range of services and patient financial burden as the care currently available to patients with other physical illnesses. Chronic disease management is incentivized to provide teambased, proactive management through electronic health records, patient registries, improved outcome monitoring systems, and waiver of copays for patients. Substance Use Disorders under PPACA • • • • Integrates insurance coverage for substance use disorders into general medical insurance policies. Expands care delivery into mainstream medical settings such as primary care and team-based chronic disease management programs. By providing treatment of the full spectrum of substance use disorders, some of the stigma of these disorders will be removed. Greatly increases the number of individuals now eligible for some type of substance use disorder treatment, and facilitates their access to such treatment. So what does this mean for “traditional” addiction treatment services? Opportunities & Hazards • There will still be even more people with severe and advanced addictions– at least for a while. And there will be many more of these who are newly insured for addiction treatment, with benefits at parity with rates for other chronic illnesses. • Insurance carriers will be even more interested in the varying levels of care that may be necessary and sufficient. High quality diagnosis and assessment will be increasingly important, both for admission and for timing of “step-downs.” • The traditional addiction treatment programs will have to “medicalize” their care, adopting more of the methods and language of clinical specialties to their care patterns. • There will likely be increased competition from mental health providers, who may lack direct clinical experience with addicted patients, but are much more sophisticated in working with other medical specialties and medical care organizations. Opportunities & Hazards • • • There will also be opportunities for counselors currently employed in traditional programs to become involved with delivery of other levels of care in other settings. Accountable Care Organizations (Medical Homes, Health Maintenance Organizations, and other integrated care networks) will be strongly supported by the ACA, and much of the early intervention work will be carried out in these organizations. Primary Care physicians will play key roles in the provision of this care, and substance use counselors—if properly trained and oriented—could also be involved at this level. Integrated treatment of co-occurring psychiatric and medical disorders will also become increasingly common, and it will be important for counselors to obtain the knowledge and develop the collaborative skills necessary to participate with other providers from a variety of disciplines. In the Supreme Court’s 2012 decision upholding the Affordable Care Act, it gave the states the choice to opt out of Medicaid expansion. It is now rests with governors and state legislatures to decide whether it is in the best interest of the state to implement the Medicaid portion of the law that affords health coverage to those in need. Medicaid Expansion • • • • Medicaid currently requires coverage for certain groups of individuals: low-income children and some of their parents; poor pregnant woman; certain low-income seniors; and some individuals with disabilities who are under the age of 65. Under the Affordable Care Act, Medicaid eligibility would be extended to all individuals with incomes up to 138% of the federal poverty level --$26,347 for a family of three and $15,417 for an individual. As of June 2014, Medicaid expansion in several Western states, as an example, provided new coverage for 175,000 people in Nevada, 345,000 in Oregon, 403,000 in Washington, and 1,743,000 in California. In states that have not expanded Medicaid, many people are caught in a coverage gap: unable to obtain Medicaid benefits, and too poor to qualify for ACA insurance subsidies. Pennsylvania expanded Aug 28 * Previous Versions • Levels of care and lengths of stay originally based on what insurance companies would pay for (eg, Minnesota Model inpatient) • In early ‘90s, ASAM developed a single set of criteria for levels of care • PPC: Patient Placement Criteria • Three editions of PPC: 1991, 1996, 2001 What’s new? • Not just a checklist—a 465 page book • Shifted from “placement” criteria to “treatment criteria” • Shift from program-driven treatment to individualized, clinically-driven treatment • Updated terminology, eg • “Resistant” now “not interested in stopping use” • “Inappropriate use” now ‘High-risk use” • Sections on special populations Efficacy vs Effectiveness • Efficacy = a treatment or intervention produces positive results in a controlled experimental research trial. • Effectiveness = a treatment or intervention produces positive results in a usual or routine care setting (i.e., in the real world). Research-only approach to EBPs • Emphasizes scientific research and contrasts scientific evidence with approaches based on “global subjective judgment,” consensus, preference, and other forms of “nonrigorous” assessment. • Criticism: The true performance of an intervention often remains uncertain even when research evidence is available. • Criticism: Certain types of interventions are more amenable to research than are others and are therefore more likely to be supported by research evidence. • Criticism: Definitions of successful outcomes are not universally shared, especially in behavioral health. • Criticism: Clinical decision-making and health policy involve factors and trade-offs related to patient and community values, culture, and competing priorities that are not generally informed by research. Multiple Streams of Evidence • The Institute of Medicine has argued for an approach that reflects “multiple streams of evidence”: 1. Best research evidence—the support of clinically relevant research, especially that which is patient centered 2. Clinician expertise—the ability to use clinical skills and past experience to identify and treat the individual client 3. Patient values—the integration into treatment planning of the preferences, concerns, and expectations that each client brings to the clinical encounter http://www.nrepp.samhsa.gov DISCLAIMER NREPP rates the quality of the research supporting intervention outcomes and the quality and availability of training and implementation materials. NREPP ratings do not reflect an intervention's effectiveness. Users should carefully read the Key Findings sections in the intervention summary to understand the research results for each outcome. NREPP does not provide an exhaustive list of interventions or endorsements of specific interventions, since NREPP has not reviewed all interventions. Policymakers and funders in particular are discouraged from limiting contracted providers and/or potential grantees to selecting only among NREPP interventions. Review of interventions and their posting on the NREPP Web site do not constitute an endorsement, promotion, or approval of these interventions by NREPP or SAMHSA. http://www.healthquality.va.gov/guidelines/MH/sud/ DISCLAIMER The Department of Veterans Affairs (VA) and The Department of Defense (DoD) guidelines are based on the best information available at the time of publication. They are designed to provide information and assist in decision-making. They are not intended to define a standard of care and should not be construed as one. Also, they should not be interpreted as prescribing an exclusive course of management. Variations in practice will inevitably and appropriately occur when providers take into account the needs of individual patients, available resources, and limitations unique to an institution or type of practice. Every healthcare professional making use of these guidelines is responsible for evaluating the appropriateness of applying them in any particular clinical situation. ! Table&A(4:&Final&Grade&of&Recommendation! ! The&net&benefit&of&the&intervention! Quality(of! Evidence! Good! ! Substantial! A! ! ! Moderate! Small! B! C! Zero&or! Negative! D! Fair! B! B! C! D! Poor! I! I! I! I! ! Evidence&Rating&System! ! A! A!strong!recommendation!that!the!clinicians!provide!the! intervention!to!eligible! patients.! ! B! A!recommendation!that!clinicians!provide!(the!service)!to! Good&evidence&was&found&that&the&intervention&improves& eligible!patients.! important&health&outcomes&and&concludes&that&benefits& !substantially&outweigh&harm.! least&fair&evidence&was&found&that&the&intervention& C! At& No!recommendation!for!or!against!the!routine!provision!of! improves& health&outcomes&and&concludes&that&benefits& the!intervention!is!made.! !outweigh&harm.! At&least&fair&evidence&was&found&that&the&intervention&can& improve&health&outcomes,&but&concludes&that&the&balance&of& benefits&and&harms&is&too&close&to&justify&a&general& recommendation.! D! Recommendation!is!made!against!routinely!providing!the! intervention!to!asymptomatic!patients.! ! At&least&fair&evidence&was&found&that&the&intervention&is& ineffective&or&that&harms&outweigh&benefits.! I! ! ! ! The!conclusion!is!that!the!evidence!is!insufficient!to! recommend!for!or!against! routinely!providing!the!intervention.! ! Evidence&that&the&intervention&is&effective&is&lacking,&or&poor& quality,&or&conflicting,&and&the&balance&of&benefits&and&harms& cannot&be&determined.! VA/DoD Clinical Practice Guideline For Management of Substance Use Disorders Appendix C: Addiction-Focused Psychosocial Interventions Summary of Effectiveness of Psychosocial Interventions during early recovery (first 90 days) on condition specific outcomes of SUD (use or consequences) or general psychosocial functioning First line alternatives at least as effective as other bona fide active interventions or treatment as usual (TAU) Added effectiveness as adjunctive interventions in combination with pharmacotherapy and/or other first line psychosocial interventions Interventions Alcohol Opioids Stimulants Cannabis Alc Ops Stim Cann Comments (alphabetical) /mixed Behavioral Couples Therapy +++ N/A +++ N/A +/- + ? Cognitive +++ Behavioral Coping Skills Training N/A +++ ++ + +++ N/A ++ Contingency N/A Management/ Motivational Incentives N/A N/A N/A + +++ +++ N/A Community +++ Reinforcement Approach N/A + N/A N/A N/A + N/A Complex intervention Motivational +++ Enhancement Therapy (MET) N/A N/A ? +++ ? + May improve treatment engagement as adjunct to TAU for stimulants; Some evidence for those with low readiness or high anger Twelve-Step +++ Facilitation N/A N/A N/A ++ N/A + N/A AA participation is correlated with outcome – appears to mediate TSF effects +/- N/A Effective for male or female patients with SUD and partners; improves marital satisfaction +++ based on meta analysis of comparison with bona fide alternative interventions + or ++ Based on one (+) or more (++) individual trials in comparison with bona fide alternatives N/A: evidence not available; +/- evidence inconsistent across outcomes; ?: benefit questionable Predictions • Evidence Based Practices will increasingly be developed to target more specific problems and levels of severity. • All treatments will be increasingly subject to accountability standards. That is, we must be able to demonstrate that the treatments we are providing are effective, producing measurable positive changes. EBPs will play an important role in these accountability standards * Of particular importance to all providers will be the ability to offer an attractive and evidence-based set of treatment services to the new and more diverse, educated and consumer savvy population of insured patients. Predictions • The well-established failure of the traditional addiction specialty programs to offer evidence based medications, individual therapies and continuing care services has been variously attributed to treatment philosophy,ideology, inadequate economic resources, and/or workforce limitations. • Regardless, the new marketplace is likely to be much more sophisticated, and payers and referral sources are likely to know more about state-of-the-art care methods; and justifiably ask for proof of effectiveness. Again, traditional addiction treatment providers currently have the clear historical and experiential advantage • …but Kodak and Polaroid once held similar technological and experiential precedence in the camera industry