Hot Topics in Chronic Pain Management: Questions Every
advertisement

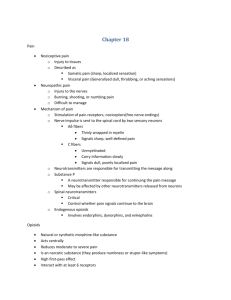
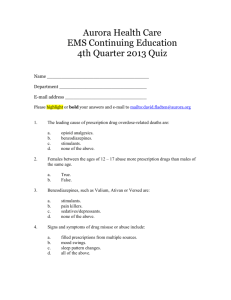
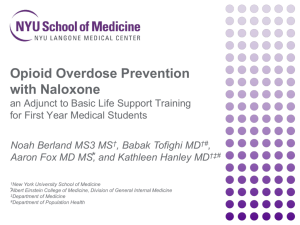
Hot Topics in Chronic Pain Management: Questions Every Pain Pharmacist is Asked William D. Gersch PharmD, BCPS Clinical Pharmacy Specialist – Pain Management Kaiser Permanente Colorado Colorado Pharmacists Society 2016 Winter CE and Ski Seminar January 9th - 13th Conflict of Interest Disclosure I have no conflicts of interest to disclose. Objectives Summarize the role of buprenorphine for chronic pain management Critique the rationale for opioid dose limiting Develop criteria for naloxone prescribing/dispensing Describe an appropriate UDS monitoring program in clinical practice BUPRENORPHINE AND CHRONIC PAIN Buprenorphine is indicated for the management of chronic pain? Green – True Pink – False Background Semisynthetic derivative of thebaine, an opioid alkaloid Mixed partial agonist opioid receptor – Mu receptor partial agonist – Kappa receptor antagonist C-III medication for the management of opioid dependence and chronic pain – Suboxone® (buprenorphine/naloxone) and Subutex® (buprenorphine) are FDA indicated for opioid dependence – Butrans® (buprenorphine) is FDA indicated for the management of chronic pain Heit HA et al. Clin J Pain. 2008; 24:93-97 Advantages Long-acting due to slow dissociation from the opioid receptor Ceiling effect for CNS and respiratory depression – Higher doses result in antagonistic effect Potentially less hyperalgesia due to partial agonist properties No dose adjustments for renal impairment Less constipation Not associated with hypogonadism due to lack of HPA axis impact Potentially less immunosuppression Boas RA et al. Br J Anaesth 1985; 57:192–196 Sporer KA. Ann Emerg Med 2004; 43:580–584 Raisch DW et al. Ann Pharmacother 2002; 36:312–321. Pergolizzi JV et al. Acta Anaesthesiol Taiwan 2015; 53(2):71-6 Sacerdote P. Curr Opin Support Palliat Care 2008; 2:4-18 High Receptor Affinity – Blessing or Curse Lower level of physical dependence Potentially more mild withdrawal symptoms Improves safety profile if non-prescribed opioids are taken Challenge for incident pain management Resistance to opioid antagonist such as naloxone in overdose situations Breen CL et al. Drug Alcohol Depend 2003; 71:49–55. Disadvantages Analgesic effects may not be as powerful as a full opioid agonist Drug interactions – CYP 3A4 inducers – Increases nor-buprenorphine which has more potent respiratory effects – QTc prolonging agents Abuse – Finland 56% of opioid agonist treatment were due to buprenorphine 33% of clients reported buprenorphine as their primary drug of abuse – French survey noted that 54% treatment patients used non-prescribed buprenorphine – Polysubstance abuse with other CNS depressants is common to achieve sedation, intoxication and euphoria UDS monitoring is more challenging/expensive Ohtani M et al. J Pharmacol Exp Ther 1995; 272:505–510 EMCDDA. 2008 National Report (2007 Data) to the EMCDDA by the Finnish National Focal Point, STAKES. Available at: http://www.emcdda.europa.eu/attachements.cfm/att_86775_EN_NR_2008_FI.pdf. Accessed November 16, 2015. EMCDDA. Buprenorphine—Treatment, Misuse and Prescription Practices. Lisbon: EMCDDA; 2005. Accessed November 16, 2015. Prescribing Pearls Use of buprenorphine “off-label” for the management of pain is not prohibited under DEA regulations – Prescribers do not need a waiver from Center for Substance Abuse Treatment (CSAT) – Prescribers should not place an “X” before their DEA number Ideally if used for chronic pain, prescribers should note one or both of the following on the prescription to avoid confusion: – “Chronic Pain Patient” – “Off-labeled Use” Heit HA et al. Pain Med 2004; 5:303–308 Conversions Suboxone® and Subutex® sublingual tablets – 0.4mg SL buprenorphine = 30mg PO morphine – Maximum dose for chronic pain is generally considered to be 32mg daily – Some suggest TID – QID dosing but this is not clearly supported in the literature Butrans® – Ratio estimated to be 1mg TD buprenorphine = 70-115mg PO morphine – Manufacturer’s guideline MED < 30mg daily → Butrans ® 5mcg/hr MED < 30-80mg → Butrans ® 10mcg/hr MED > 80mg → caution advised – Recommended to taper patients to < 30mg MED for up to 7 days prior to switching to Butrans® – Maximum dose is 20mcg/hr due to QTc prolongation Heit HA et al. Clin J Pain 2008; 24:93-97 McPherson ML. (2010). Demystifying Opioid Conversion Calculations: A Guide for Effective Dosing. Bethesda MD: American Society of Health-System Pharmacists OPIOID DOSE LIMITING What is the biggest risk factor for an opioidrelated overdose Green – opioid daily dose greater than 120mg MED Pink – concurrent use of benzodiazepines/hypnotics Purple – aberrant behaviors Yellow – comorbid mental health disorders Morphine Equivalent Dosage (MED) Drug Oral Equianalgesic Dose (mg) Morphine 30 Multiple conversion tables available Buprenorphine 0.4 (SL) Codeine 200 This table is a compilation of multiple different sources Fentanyl 15mcg/hr (TD)** Hydrocodone 30 Hydromophone 7.5 Meperidine 300 Methadone 10** Oxycodone 20 Oxymorphone 10 Tramadol 120 Used to standardize opioid dosing with various agents McPherson ML. (2010). Demystifying Opioid Conversion Calculations: A Guide for Effective Dosing. Bethesda MD: American Society of Health-System Pharmacists Dose Limiting Recommendations Washington State passed legislation requiring all patients prescribed more than 120mg MED daily to be followed/reviewed by a pain specialist – Several other states and organizations have also followed suit The CDC also recommended that patients prescribed more than 120mg MED without substantial improvement should be referred to a pain specialist American Academy of Neurology: “If daily dosing exceeds 80–120mg MED daily, consultation with a pain management specialist is recommended, particularly if pain and function have not substantially improved” Leavitt SB. Do Higher Opioid Doses Increase Overdose Risks?. Accessed 11/171/15. http://updates.paintopics.org/2010/02/do-higher-opioid-doses-increase.html CDC Unintentional Drug Poisoning in the United States. Accessed 11/16/15. www.cdc.gov/injury Franklin GM. Neurology 2014; 83(14):1277-1284 Opioid Concerns Prescription opioids caused 16,651 deaths in 2010 Substance-abuse admissions increased by 400% between 1998 and 2008 Prescription painkillers are the second most prevalent type of abused drug after marijuana Jones CM et al. JAMA 2013; 309:657–659 Okie S. N Engl J Med 2010; 363:1981-1985 CDC Unintentional Drug Poisoning in the United States. Accessed 11/16/15. www.cdc.gov/injury Dunn - Seattle HMO Study Designed to determine the opioid overdose risk in patients (n=9940) who received 3+ opioid prescriptions within 90 days for chronic noncancer pain, 1997-2005 Annual Overdose Rate Percentage 2.00% 1.00% 0.50% 0.00% Dunn K et al. Intern Med 2010; 152:85-92 1.8% 1.50% 0.7% 0.2% <20mg 0.3% 20-49mg 50-99mg* >100mg* Daily Opioid Dose (MED) Dunn - Seattle HMO Study Percentage Breakdown Use without a documented overdose Non-fatal overdoses 99.49% Fatal overdoses 0.51% 0.06% 0.45% Dunn K et al. Intern Med 2010; 152:85-92 Dunn - Seattle HMO Study and 100mg MED Daily Most of the overdoses (78.4%) occurred among patients receiving less than 100mg MED Opioid Dose (MED mg/day) Number of Overdoses Overall Overdose Percentages 0 6 11.8% 1-<20 22 43.1% 20-<50 6 11.8% 50-<100 6 11.8% >100 11 21.6% Dunn K et al. Intern Med 2010; 152:85-92 Aberrant Behaviors Almost half (25 of 51) of overdose patients were expressing some aberrant behavior: – Eight cases involved accidental excess ingestion of opioids – Six were suicide attempts – Three persons obtained additional opioids illicitly – Four patients applied extra fentanyl patches – Four patients noted some type of drug abuse Opioid-related overdoses were elevated in the following patients – History of substance abuse treatment – History of depression Dunn K et al. Intern Med 2010; 152:85-92 Non-opioids Dunn – Seattle HMO Study – Sedative hypnotics prescribed for 74.4% of patients Percentage of patients prescribed at least 45 days of sedative-hypnotics = 31.9% – Benzodiazepines prescribed for 42.7% of patients – Muscle relaxants prescribed for 52.3% of patients Dunn K et al. Intern Med 2010; 152:85-92 Bohnert - VA Study Compared VA patients that died of an opioid overdose to a random 5% sample of patients that were treated with opioids during the same time period, FY2004 and FY2005 – 750 total deaths Risk of fatal overdose = 0.04% Opioid Dose (MED mg/day) Number of Overdoses Overall Overdose Percentages 0 243 40.0% 1-<20 44 7.3% 20-<50 108 17.8% 50-<100 86 14.2% >100 125 20.6% Bohnert et al. JAMA 2011; 305(13):1315-1321 Dose Limiting: Final Thoughts There does appear to be a higher risk of opioid overdose with increased daily doses of opioids More than 75% of the total overdoses examined in both studies were in patients prescribed LESS THAN 100mg MED daily – Bohnert demonstrated that 43.5% of the fatal overdoses in the VA population were not prescribed opioids Focusing on dose alone does not appear to be the complete answer NALOXONE What is the best indicator of an opioid-related overdose Green – altered mental status Pink – decreased heart rate Purple – miotic (constricted) pupils Yellow – decreased respiratory rate Opioid Epidemic Poisoning is the leading cause of injury related death in the US – Opioid deaths accounted for more than 55% of US poisoning deaths in 2013 Opioid analgesics – 16,235 Heroin – 8,257 The United Nations recognized overdose as a global public health issue Hedegaard H et al. NCHS data brief, no 190. Hyattsville, MD: National Center for Health Statistics. 2015. Centers for Disease Control and Prevention (CDC). Morb Mortal Wkly Rep 2012; 61:101-5 Walley AY et al. BMJ 2013; 346:f174 Naloxone Naloxone is an opioid antagonist that reverses the effects of opioid overdose – Competes for the mu, kappa, and sigma opiate receptor sites in the CNS with the highest affinity for the mu receptor – Reverses opioid overdoses only From 1996-2014 an estimated 152,283 lay persons received Overdose Education and Naloxone Distribution (OEND) from 644 sites throughout the US – Resulted in 26,453 opioid overdose rescues Warner M et al. NCHS Data Brief 2011; 81:1-8 Product Information: NARCAN(R). Endo Pharmaceuticals Inc, Chadds Ford, PA, 2003. Wheeler E et al. MMWR Morb Mortal Wkly Rep. 2015 Jun;64(23):631-5. Dosing IV/IM/subQ: 0.4-2mg Intranasal: 2mg – Dispensed with a mucosal atomizer device – Commercially available Narcan nasal spray, approved 11/19/2015 Adapt Pharma will price the medication at $37.50 per dose for all governments and public organizations, available Jan 2016 Evzio® auto-injector: 0.4 mg IM or subQ into thigh – Once activated, provides verbal commands for administration Above doses can be repeated every 2-3 minutes If no response after 10mg, reconsider diagnosis of opioid toxicity Product Information: NALOXONE HCl. Mylan Institutional LLC, Rockford, IL, 2014. Lavonas EJ et al Circulation 2015; 132(18 Suppl 2):S501-S518. Adapt Pharma Press Release. http://www.adaptpharma.com/press-releases. Accessed 11/18/2015. Product Information: EVZIO(TM). Kaleo, Inc., Richmond, VA, 2014. Signs and Symptoms of an Opioid-related Overdose Depressed mental status – Non-responsive to external stimuli (yelling, sternal rub, gentle shaking, pain) Decreased respiratory rate (less than 12 breaths/minute) – Best predictor of an opioid-related overdose – Results in blue/purple cast to fingertips, fingernails or lips Decreased heart rate Decreased bowel sounds Miotic (constricted) pupils – Normal pupils does not exclude opioid intoxication: meperidine or coingestants Stolbach A. Acute opioid intoxication in adults. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. (Accessed on November 16, 2015.) Coffin P. Prevention of lethal opioid overdose in the community. UpToDate, Post TW (Ed), UpToDate, Waltham, MA. (Accessed on November 16, 2015.) Hoffman JR. Ann Emerg Med 1991; 20(3):246 Response to Overdose Attempt to arouse patient with a firm sternal rub If there is shallow or absent breathing administer naloxone Call 911 Perform rescue breathing Re-administer naloxone after 2-3 minutes if still non-responsive Stay with the patient for at least three hours or until help arrives Place person on his/her side to prevent aspiration after vomiting. Coffin P. Prevention of lethal opioid overdose in the community. UpToDate, Post TW (Ed), UpToDate, Waltham, MA. (Accessed on November 16, 2015.) Identifying Patients at Risk No consensus on who should receive naloxone for overdose prevention History of a previous opioid overdose – Strongest predictor History of a substance use disorder Higher the dose, higher the risk – MED >100mg daily results in a 9-fold increase in risk of an overdose Presence of aberrant drug taking behavior Concurrent use of other sedatives or alcohol Recent abstinence Comorbid pulmonary disease and/or sleep apnea Coffin PO et al. Acad Emerg Med 2007 Jul; 14(7):616-23 Dunn K et al. Intern Med 2010; 152:85-92 Bohnert et al. JAMA 2011; 305(13):1315-1321 Darke S et al. J Urban Health. 2003 Jun; 80(2):189-200 Chaparro LE. Spine. 2014 Apr;39(7):556-63 Overview of CO Naloxone Laws SB 13-014 - provides protection from criminal charges for medical professionals who prescribe naloxone to third parties, and for nonmedical people who witness an overdose and administer the drug. It protects healthcare professionals who administer naloxone in an overdose emergency from charges SB 12-020 - encourage witnesses to call for medical help during emergency overdose situations. The law provides limited legal protection from drug charges for those who call 911 for help. It also protects persons suffering an opiate overdose SB 15-053 - allows physicians to write standing orders for naloxone that can be dispensed by designated pharmacists (or harm reduction agencies) Colorado Consortium for Prescription Drug Abuse Prevention. The Problem: Laws and Policies. Accessed 11/16/15. http://takemedsseriously.org/the-problem/laws-policies/ URINE DRUG SCREEN MONITORING Which of the following patients should be selected for a urine drug screen Green – 75yo grandmother prescribed zolpidem 5mg QHS + trazodone 50mg QHS PRN sleep Pink – 21yo college student with a hx of Percocet overdose, but not currently prescribed any controlled medications Purple – 44yo engineer prescribed morphine SR 30mg Q8H Yellow – 55yo psychologist prescribed lorazepam 1mg TID PRN anxiety Benefits Urine drug screening (UDS) is a necessary tool for: – Confirming compliance with prescribed medications – Identifying the use of illicit substances Random testing is more likely to detect surreptitious drug use UDS monitoring demonstrated improvement in identifying aberrant drug taking behaviors versus clinical assessment alone Urine is preferred over blood or saliva for monitoring Chou R et al. J Pain. 2009; 10(2):113 Becker W et al. Prescription drug misuse: Epidemiology, prevention, identification, and management. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. (Accessed on November 16, 2015.) Katz NP et al. Anesth Analg 2003 Oct; 97(4):1097-102 Pesce A et al. Pain Medicine 2012; 13:868–885 Types Immunoassay – The most common method for the initial screening process – Uses antibodies for substance detection – Large scale and fast results – Cost effective – Can result in false positive results Gas chromatography–mass spectrometry (GC-MS) – Criterion standard for confirmatory testing – Can detect small quantities of a substance – Most accurate, reliable and sensitive method of testing – Time consuming – Costly – Generally reserved for confirmatory testing after an immunoassay screen Moeller KE et al. Mayo Clin Proc 2008; 83(1)66-76 Detection Times Moeller KE et al. Mayo Clin Proc 2008; 83(1)66-76 Who to Test All chronic users of controlled substances – Opioids – Benzodiazepines – Hypnotics Patients with a history of chemical dependency – Monitoring for abstinence – Indicator for chemical dependency referral When to Test – Risk Stratification Model Low Medium High No hx substance abuse Family hx substance abuse Hx substance abuse Low opioid dose < 50mg MED Moderate opioid dose 50100mg High opioid dose > 100mg No concurrent sedatives Concurrent sedatives + low opioid dose Concurrent sedatives + moderate dose No aberrant behaviors Expressing aberrant behaviors No hx medication overdose Hx medication overdose When to Test Once yearly Dunn K et al. Intern Med 2010; 152:85-92 Bohnert et al. JAMA 2011; 305(13):1315-1321 Coffin PO et al. Acad Emerg Med 2007 Jul; 14(7):616-23 Darke S et al. J Urban Health. 2003 Jun; 80(2):189-200 Twice yearly Four times yearly Interpretation Pearls PRN medications and negative results – Important to determine average daily dose and most recent use Amphetamine – Multiple false positives, obtain confirmation screen Methadone and fentanyl – Will not return a positive opiate screen, requires a specific screen Oxycodone – Can be +/- on a screen depending on dose, may require confirmation Heroin – 6-MAM metabolite has a short half-life (36min) and is typically only detectable up to 8hrs after use Cocaine – Few false positives via immunoassay, rarely requires confirmation Moeller KE et al. Mayo Clin Proc 2008; 83(1)66-76 Pesce A et al. Pain Medicine 2012; 13:868–885 Questions???