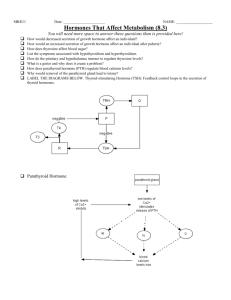
questions - WordPress.com
advertisement

Ⅰ、TERMS 1. Internal environment 3. Negative feedback 2. Homeostasis 4. Positive feedback Ⅱ、QUESTION Describe the ways for the regulation of body functions. Internal environment: The extracellular fluid provides all cells with a constant environment to live in. For this reason, the extracellular fluid is called the internal environment of the body 2. Homeostasis :used by physiologists to mean maintenance of constant conditions in the internal environment. • . Negative feedback: Negative feedback signals always produce an effect opposite to that produced by the initiating stimulus . • For example: the arterial pressure – regulating mechanism. . Positive feedback: In positive feedback control system, deviations from the steady state are actually amplified, rather than diminished, by the feedback loop. That is, a positive feedback circuit intensifies the activity of the control system. • For instance: micturition reflex, parturition, blood coagulation. Describe the ways for the regulation of body functions. 1) Nervous regulation; (2) Humoral regulation; (3) Autoregulation. 1. Channel proteins 2. Voltage gating 3. Ligand gating 4. Primary active transport and secondary active transport 5. Resting potential 6. Action potential 7. Threshold potential 8. All-or-nothing principle 9. Absolute refractory period 10. End plate potential 11. Excitation-contraction coupling 12. Isometric contraction & isotonic contraction QUESTIONS 1. Describe the ways of membrane transport. 2. Describe the physiological role of sodium pump. 3. List the important factors in the establishment of the normal resting potential. 4. Describe the mechanism of the initiation and termination of action potential (AP). 5. Describe the molecular mechanism of muscle contraction. 6. List the important factors that affect contractile performance of skeletal muscle. 1. Channel proteins The protein channels are watery pathways through the interstices of the protein molecules. Substances can diffuse by simple diffusion directly through these channels from one side of the membrane to the other. The protein channels are distinguished by two important characteristics: (1) they are often selectively permeable to certain substances and (2) many of the channels can be opened or closed by gates. 2. Voltage gating Some protein channel gates respond to the electrical potential across the cell membrane, this causes a conformational change in the protein molecule that opens or closes the gate. This is called Voltage gating. 3. Ligand gating Some protein channel gates are opened by the binding of a chemical substance (a “ligand”) with the protein, this causes a conformational change in the protein molecule that opens or closes the gate. This is called chemical gating or ligand gating. 4. Primary active transport and secondary active transport When a cell membrane moves molecules or ions “uphill” against a concentration gradient (or “uphill” against an electrical or pressure gradient), the process is called active transport. Active transport is divided into two types according to the source of the energy used to cause the transport. They are called primary active transport and secondary active transport. In primary active transport, the energy is derived directly from breakdown of adenosine triphosphate (ATP) or of some other highenergy phosphate compound. In secondary active transport, the energy is derived secondarily from energy that has been stored in the form of ionic concentration differences between the two sides of a membrane, created in the first place by primary active transport. 5. Resting potential The resting potential is the transmembrane potential difference across the membrane of a normal cell at rest. Resting potential of cells is typically in the range of -10 to -100 mV, the inside of the cell being negative with respect to the outside. 6. Action potential Some of the cells (excitable cells) are capable to rapidly reverse their resting potential from negative resting values to slightly positive values. This transient and rapid change in membrane potential is called an action potential. 7. Threshold potential A sudden rise in membrane potential of 15 to 30 millivolts usually is required to initiate an action potential. The threshold potential is the membrane potential to which a membrane must be depolarized to initiate an action potential. 8. All-or-nothing principle Once an action potential has been elicited at any point on the membrane of a normal fiber, the depolarization process travels over the entire membrane if conditions are right, or it might not travel at all if conditions are not right. This is called the all-or-nothing principle. 9. Absolute refractory period That period immediately following the discharge of an action potential during which the cell cannot be induced to fire again. 10. End plate potential Upon the arrival of an action potential at the axon terminal, acetylcholine releases and binds to the nicotinic acetycholine receptors that dot the motor end plate. Thus opening of acetylcholine-gated channels is to allow large numbers of sodium ions to pour to the inside of the fiber, carrying with them large numbers of positive charges. This creates a local positive potential change inside the muscle fiber membrane called the end plate potential. In turn, this end plate potential initiates an action potential spreading along the muscle membrane and thus causes muscle contraction. 11. Excitation-contraction coupling To cause muscle contraction, electrical currents must penetrate deeply into the muscle fiber to the vicinity of all the separate myofibrils. This is achieved by transmission of action potentials along transverse tubules (T tubules) that penetrate all the way through the muscle fiber from one side to the other. The T tubule action potentials in turn cause release of calcium ions in the immediate vicinity of all the myofibrils, and these calcium ions then cause contraction. This overall process is called excitation-contraction coupling. 12. Isometric contraction & isotonic contraction Muscle contraction is said to be isometric when the muscle does not shorten during contraction and isotonic when it does shorten with the tension on the muscle remaining constant. QUESTIONS 1. Describe the ways of membrane transport. (1) Simple diffusion; (2) Facilitated diffusion; (3) Active transport; (4) Endocytosis and exocytosis. 2. Describe the physiological role of sodium pump. (Maintain high intracellular K+ concentration gradients across the membrane. Control the volume of cell. Provides energy for secondary active transport. Develop and maintain Na+ and K+ concentration gradients across the membrane which are essential for bioelectricity activity. Electrogenic action influences membrane potential.(ie contribute to negative intracellular charge by 3 Na out and 2K in process) 3. List the important factors in the establishment of the normal resting potential. (1) K+ diffusion potential; (2) Na+ diffusion; (2) Na+-K+ pump. 4. Describe the mechanism of the initiation and termination of action potential (AP). (1) Mechanism of the initiation of AP: a. Local response and Na+ channel activated; b. Regenerative cycle of Na+ influx; c. Threshold potential. (2) Mechanism of the termination of AP: a. Na+ channel inactivated; b. K+ channel activated. 5. Describe the molecular mechanism of muscle contraction. (1) Increase of intracellular calcium level; (2) Combination of calcium ion with troponin C; (3) Conformational change of troponin complex and tropomyosin; (4) “Uncovery” of active sites of the actin; (5) Interaction of myosin and actin filaments; (6) Sliding mechanism, “walk-along” theory. 6. List the important factors that affect contractile performance of skeletal muscle. (1) Preload; (2) Afterload; (3) Contractility. TERMS 1. Hematocrit 2. Colloid osmotic pressure 3. Erythrocyte sedimentation rate 4. Erythropoietin 5. Hemostasis 6. Blood coagulation 7. Antithrombin III 8. Blood typing QUESTIONS 1. Summarize the functions of red blood cells. 2. Describe the physiological properties of platelets. 3. Name the common blood types, and describe how blood is typed and crossmatched. 4. Describe the blood clotting and anti-clotting systems and the clinical importance of each system. TERMS 1. Hematocrit The ratio of the volume of the packed red blood cells to the total blood volume is referred to as the haematocrit. Normal value Male is about 40%-50% Female is 37%-48% Newborn: 55% The haematocrit of anemic patient decreases. 2. Colloid osmotic pressure • Colloid osmotic pressure of plasma is formed by plasma proteins (mainly albumin). • Its normal value is 25 mmHg, a tiny fraction of total osmotic pressure of plasma. Ions diffuse rapidly across the capillary wall but proteins do not, so colloid osmotic pressure of plasma plays an important role in determining the balance of distribution of fluid between extravascular and intravascular spaces and maintaining normal blood volume 3. Erythrocyte sedimentation rate measured as the length of a clear column of plasma after one hour. 4. Erythropoietin Erythropoietin (EPO), a glycoprotein hormone produced primarily by cells of the peritubular capillary endothelium of the kidney, is responsible for the regulation of red blood cell mainly in low oxygen states. 5. Hemostasis In normal condition when a small blood vessel is severed or ruptured, the injury can initiate a series of events that stop the bleeding automatically within a few minutes. This process to arrest the bleeding is called hemostasis. Hemostasis is the result of 3 interacting, overlapping mechanisms: (1) vascular spasm, (2) formation of a platelet plug, (3) blood coagulation, 6. Blood coagulation Blood coagulation means conversion of fluid state into colloid state of blood. It takes place in three essential steps: 1 ) Formation of prothrombin activator. (2) The prothrombin activator catalyzes conversion of prothrombin into thrombin. (3) The thrombin acts as an enzyme to convert fibrinogen into fibrin fibers that enmesh platelets, blood cells, and plasma to form the clot. 7. Antithrombin III Antithrombin, an alpha-globulin, is a potent inhibitor of the coagulation cascade. It is a non–vitamin K-dependent protease that inhibits the action of thrombin as well as other procoagulant factors (eg, factor Xa). 8. Blood typing Before giving a transfusion to a person, it is necessary to determine the blood type of the recipient’s blood and the blood type of the donor blood so that the bloods can be appropriately matched. This is called blood typing, and it is performed in the following way: The red blood cells are first separated from the plasma and diluted with saline. One portion is then mixed with anti-A agglutinin and another portion with anti-B agglutinin. After several minutes, the mixtures are observed under a microscope. If the red blood cells have become clumped - that is, “agglutinated”-one knows that an antibody-antigen reaction has resulted. 1. Summarize the functions of red blood cells. (1) Transport of O2 and CO2; (2) Buffering. 2. Describe the physiological properties of platelets. (1) Adhesion; (2) Aggregation; (3) Release. 4 contraction 5. absorption 3. Name the common blood types, and describe how blood is typed and crossmatched. (1) The common blood types: A, B, AB, O; (2) How is blood typed and cross-matched. Blood typing Sera Red blood cell types Anti-A Anti-B O - - A + - B - + AB + + 4. Describe the blood clotting and anti-clotting systems and the clinical importance of each system. (1) Blood clotting system: Blood coagulation system: • a. Extrinsic pathway- The extrinsic pathway for initiating the formation of prothrombin activator begins with a traumatized vascular wall or traumatized extravascular tissues that come in contact with the blood. This leads to the following steps. • Release of tissue factor. • Activation of Factor X - role of Factor VII and tissue factor. • Effect of activated Factor X (Xa) to form prothrombin activator - role of Factor V. • b. intrinsic pathway- The second mechanism for initiating formation of prothrombin activator, and therefore for initiating clotting, begins with trauma to the blood itself or exposure of the blood to collagen from a traumatized blood vessel wall.Then the process continues through the series of cascading reactions. • Blood trauma causes • (1) activation of Factor XII and (2) release of platelet phospholipids. • Activation of Factor XI. • Activation of Factor IX by activated Factor XI. • Activation of Factor X-role of Factor VIII. • Action of activated Factor X to form prothrombin activator-role of Factor V. Clinical importance: mainly, prevention of bleeding. (2) Anti-clotting system: a. Intravascular anticoagulants: a) Endothelial surface factors; b) Antithrombin III; c) Heparin. b. Fibrinolysis. Clinical importance: Prevention of blood clotting, lysis of blood clots. 1 Premature systole 2. Atrioventricular delay 3. Electrocardiogram 4. Cardiac cycle 5. Stroke volume 6. cardiac output 7. Ejection fraction 8. Cardiac index 9. Cardiac reserve 10. Frank-Starling mechanism 11. Blood pressure 12. Central venous pressure 13. Renin-angiotensin system 14. Nitric oxide synthase 15. Vasomotor center 16. Baroreceptor reflex 1.Cardiac cycle 2.Stroke volume 3.Cardiac output 4.Cardiac reserve 5.cardiac index 6.ejection fraction 7.Blood pressure 8. Central venous pressure 9. Mean circulatory filing pressure 10. Premature systole 11. Process of cardiac cycle 12. Factors affecting cardiac output. 13. Action potential of cardiac working cell, autorhythmic cell and the ionic basis for its genesis 14. Factors affecting artery blood pressure. 15. Factors affecting venous back flow. 16. Factors affecting formation of interstitial fluid pressure. 17. Cardiovascular reflex. QUESTIONS 2. Describe the way the ECG is recorded and the waves of the ECG. 3. Describe in sequence the events that occur in the heart during cardiac cycle. 4. List the factors that affect heart pumping and the effect of each. 5. State the Poiseuille formula for flow in blood vessels, and explain on the basis of this formula why the radius of a vessel is such an important determination of flow. 6. List the factors affecting arterial blood pressure. 7. Describe the local control of blood flow. 8. List the factors affecting formation of interstitial fluid. 9. Outline the neural mechanisms that control arterial blood pressure and heart rate, including the receptors, afferent and efferent pathways, central integrating pathway, and effector mechanisms involved. 10. List the principal vasoregulatory factors secreted by endothelial cells, and describe the function of each. 11. Name the principal hormones that affect arterial blood pressure, and know the physiologic role of each. 12. Summarize the integrated, multifaceted system for arterial pressure regulation. 1. Premature systole A premature contraction of the heart, resulting in momentary cardiac arrhythmia, is called premature systole. 2. Atrioventricular delay The conductive system is organized so that the cardiac impulse does not travel from the atria into the ventricles too rapidly. It is primarily the A-V node and its adjacent conductive fibers that delay this transmission of the cardiac impulse from the atria into the ventricles. This delay allows time for the atria to empty their blood into the ventricles before ventricular contraction begins. 3. Electrocardiogram When the cardiac impulse passes through the heart, electrical current also spreads from the heart into the adjacent tissues surrounding the heart. A small proportion of the current spreads all the way to the surface of the body. If electrodes are placed on the body skin on opposite sides of the heart, electrical potentials generated by the current can be recorded; the recording is known as an electrocardiogram. 4. Cardiac cycle The period of one contraction and one relaxation of the heart. The cardiac cycle consists of a period of relaxation called diastole, during which the heart fills with blood, followed by a period of contraction called systole. 5. Stroke volume Stroke volume is the volume of blood ejected from the left ventricle each beat. In adults, the normal value of stroke volume output for the resting adult is 60~80ml. 6. Cardiac output Cardiac output is the total volume of blood pumped by the ventricle per minute, or simply the product of heart rate (HR) and stroke volume (SV). The average cardiac output for the resting adult is about 5 L/min. 7. Ejection fraction The percentage of blood that is pumped out of a filled ventricle as a result of a heartbeat is called ejection fraction. Ie stroke volume/end diastolic volume *100% 8. Cardiac index There is a correlation between resting cardiac output and body surface area. The output per minute per square meter of body surface area is known as the cardiac index. It averages 3.2L/ min·m2 9. Cardiac reserve The capacity of the heart to increase cardiac output to satisfy human metabolic needs is called cardiac reserve. The maximal cardiac output subtracts the normal value. It reflects the ability of the heart to adapt the change of environment (internal or external) 10. Frank-Starling mechanism The heart has the intrinsic capability of increasing its force of contraction and therefore stroke volume in response to an increase in venous return. This is called the Frank-Starling mechanism. This phenomenon occurs in isolated hearts, and therefore is independent of neural and humoral influences. 11. Blood pressure The lateral pressure that the blood effects on unit area of the vessels wall is called the blood pressure. It varies with the strength of the heartbeat, the elasticity of the arterial walls, the volume and viscosity of the blood, and a person's health, age, and physical condition. In the healthy young adult, the pressure at the height of each pulse, called the systolic pressure, is about 120 mmHg and at its lowest point, called the diastolic pressure, it is about 80 mmHg. The difference between these two pressures, about 40 mmHg, is called the pulse pressure. 12. Central venous pressure The pressure in the thoracic vena cava near the right atrium is called central venous pressure (CVP). CVP is influenced by a number of factors, including cardiac output, respiratory activity, contraction of skeletal muscles and hydrostatic forces (i.e., gravity). Mean circulatory filing pressure (MCFP): when heart beat is stopped, the pressure in any point of cardiovascular system is equal. This pressure is called MCFP. systemic circulation, 7 mmHg; pulmonary circulation, 10 mmHg. 13. Renin-angiotensin system The renin-angiotensin system plays an important role in regulating blood volume, arterial pressure, and cardiac and vascular function. While the pathways for the renin-angiotensin system have been found in a number of tissues, the most important site for renin release is the kidney. Sympathetic stimulation, renal artery hypotension, and decreased sodium delivery to the distal tubules stimulate the release of renin by the kidney. Renin is an enzyme that acts upon a circulating substrate (angiotensinogen) to release a 10-amino acid peptide, angiotension Ⅰ. Vascular endothelium, particularly in the lungs, has an enzyme, angiotensin converting enzyme (ACE), that cleaves off two amino acids to form the octapeptide, angiotensin II (AII). 14. Nitric oxide synthase The enzyme that catalyzes the formation of NO from oxygen and arginine is nitric oxide synthase, a very complex enzyme containing five bound cofactors/prosthetic groups, FAD, FMN, haem, tetrahydrobiopterin (BH4) and Ca2+-calmodulin (CaM), and a heme group which is part of the catalytic site. In mammals, three distinct genes encode NOS isozymes: neuronal (nNOS or NOS1), cytokineinducible (iNOS or NOS2) and endothelial (eNOS or NOS3). 15. Vasomotor center The vasomotor center, located bilaterally mainly in the reticular substance of the medulla and of the lower third of the pons, is responsible for the overall control of blood distribution and pressure throughout the body. This center transmits parasympathetic impulses through the vagus nerves to the heart and transmits sympathetic impulses through the cord and peripheral sympathetic nerves to all or almost all the blood vessels of the body. 16. Baroreceptor reflex The baroreceptor reflex is the body's rapid response system for dealing with changes in blood pressure. This reflex is initiated by stretch receptors, called either baroreceptors or pressoreceptors, which are located in the walls of several of the large systemic arteries. If a rise in arterial pressure stretches the baroreceptors and causes them to transmit signals into the central nervous system. “Feedback” signals are then sent back through the autonomic nervous system to the circulation to reduce arterial pressure downward toward the normal level. QUESTIONS 2. Describe the way the ECG is recorded and the waves of the ECG. (1) The electrocardiogram (ECG) measures changes in skin electrical voltage/potential caused by electrical currents generated by the heart. (2) The waves of the ECG: a. P wave: the sequential depolarization of the right and left atria; b. QRS complex: right and left ventricular depolarization; c. ST-T wave: ventricular repolarization; d. U wave: origin for this wave is not clear, but probably represents "afterdepolarizations" in the ventricles. 3. Describe in sequence the events that occur in the heart during cardiac cycle. (1) Atrial systole; (2) Isovolumic contraction phase; (3) Rapid ejection phase; (4) Reduced ejection phase; (5) Isovolumic relaxation phase; (6) Rapid filling phase; (7) Reduced filling phase. 4. List the factors that affect heart pumping and the effect of each. (1) Preload — Frank-Starling mechanism; (2) Afterload; (3) Myocardial contractility; (4) Heart rate. 5. State the Poiseuille formula for flow in blood vessels, and explain on the basis of this formula why the radius of a vessel is such an important determination of flow. Poiseuille’s formula: Q=pDPr4/8hL 6. List the factors affecting arterial blood pressure. (1) Stroke Volume-stroke volume, the systolic pressure ↑ pulse pressure↑ Heart Rate-heart rate↑ the diastolic pressure ↑ ,pulse pressure ↓ pressure↑, pulse Windkessel effect of aorta and big arteries -windkessel effect ↓ the Resistance-peripheral resistance↑ ,the diastolic pressure ↓ systolic pressure ↑ , the diastolic pressure ↓ Relationship Between volume↑ , pulse pressure↑ Blood Volume and Vascular Volume-Blood the blood pressure ↑ vascular volume↑ the blood pressure ↓ 7. Describe the local control of blood flow. (1) Acute control: a. Tissue metabolism; b. Oxygen available changes: Vasodilator Theory; Oxygen Lack Theory; c. Other nutrients. (2) Long-term control. 8. List the factors affecting formation of interstitial fluid. (1) EFP = (Pc+ Pif) - (Pif+ PP); (2) Rate of lymph flow; (3) Capillary permeability. Factors Influencing Venous Backflow ⑴ Mean Circulatory Filling Pressure ↑---- Backflow ↑ ⑵ Myocardial Contractibility ↑ ----- Backflow ↑ Cardiac contractility ↑– stroke volume ↑ – ventricular pressure in diastole period ↓– blood from atria and large veins to ventricle ↑– venous return ↑ Cardiac contractility ↓– stroke volume ↓ – ventricular pressure in diastole period↑– blood from atria and large veins to ventricle ↓– venous return ↓ ⑶ Muscle Pump -Muscle rhythmic contraction , Promote blood flow significance: At upright position, muscle pump decreases venous pressure of lower limb, and reduces venous blood retention of lower limb. ⑷ respiratory movement ⑸ Stand from lying position ----- Backflow ↓ 9. Outline the neural mechanisms that control arterial blood pressure and heart rate, including the receptors, afferent and efferent pathways, central integrating pathway, and effector mechanisms involved. (1) Autonomic nervous system; (2) Vasomotor center; (3) Higher nervous centers; (4) Cardiovascular reflexes: a. Baroreceptor reflex; b. Chemoreceptor reflex; c. Cardiopulmonary reflex; d. CNS ischemic response. 10. List the principal vasoregulatory factors secreted by endothelial cells, and describe the function of each. (1) Vasodilator factors: a. PGI2; b. NO; c. EDHF. (2) Vasoconstrictor factors: Endothelin. 11. Name the principal hormones that affect arterial blood pressure, and know the physiologic role of each. (1) Angiotensin II: a. Constricts resistance vessels b. Acts upon the adrenal cortex to release aldosterone c. Stimulates the release of vasopressin d. Facilitates norepinephrine release from sympathetic nerve endings e. Stimulates thirst centers within the brain (2) Epinephrine and norepinephrine: Effects Epinephrine Norepinephrine Vessels constriction (skin, visceral) + relaxation (SM, liver) - +++ +++ total peripheral resistance ± +++ Blood pressure systolic +++ +++ diastolic ± ++ MAP ++ (3) Vasopressin: a. Vasoconstriction, increase of arterial pressure; b. Antidiuretic effect. (4) Atrial natriuretic peptide: a. Produces natriuresis and diuresis b. Decreases renin release c. Reduces total peripheral resistance via vasodilatation d. Decreases heart rate, cardiac output (5) Opioid peptide: a. Endorphin, Enkephalin, Dynorphin; + b. Complex cardiovascular effects. (6) Kinin and histamine: a. Causes vasodilatation; b. Increases capillary permeability. (7) Prostaglandins 12. Summarize the integrated, multifaceted system for arterial pressure regulation. (1) Rapidly acting pressure control mechanisms acting within seconds or minutes; (2) Pressure control mechanisms that act after many minutes; (3) Long-term mechanism for arterial pressure regulation. Respiratory system 1. Intrapleural pressure 2. Surfactant 3. Tidal volume 4. Vital capacity 5. Alveolar ventilation 6. Respiratory membrane 7. Ventilation-perfusion ration 8.Oxygen-hemoglobin dissociation curve 9. Hering-Breuer inflation reflex 1. Respiration 2. Pulmonary ventilation 3. Tidal volume 4. Functional residual capacity (FRC) 5. Physiologic dead space 6.forced vital capacity 7. alveolar ventilation 8. ventilation/perfusion ratio 9. Oxygen dissociation curve 1. How is the intrapleual pressure formed and physiological significance ? 2. Forces of pulmonary ventilation and significance of indirect force. 3. Factors affecting oxygen dissociation curve. 4. Origin, component and function of surfactant and its physiological implications Ⅲ、QUESTION Describes the effects of PCO2,[H+] and PO2 on alveolar ventilation and their mechanisms. Respiration: The process of gas exchange between the organism and the environment. 1. Intrapleural pressure (pleural pressure )is the pressure of the fluid in the narrow space between the lung pleura and the chest wall pleura. As noted earlier, this is normally a slight suction,which means a slightly negative pressure. The normal pleural pressure at the beginning of inspiration is about -5 centimeters of water,which is the amount of suction that is required to hold the lungs open to their resting level. Then,during normal inspiration,the expansion of the chest cage pulls outward on the lungs with still greater force and creates a still more negative pressure to an average of about -7.5 centimeters of water. 2. Surfactant is secreted by type Ⅱ alveoli epithelial cells. It is a complex mixture of several phospholipids,proteins,and ions. The most important components are the phospholipids dipalmitoylphosphatidylcholine ,surfactant apoproteins,and calcium ions. The dipalmitoylphosphatidylcholine , along with several less important phospholipids,is responsible for reducing the surface tension. 3. The tidal volume is the volume of air inspired or expired with each normal breath. It amounts to about 500 milliliters. 4. The vital capacity is the maximum amount of air a person can expel from the lungs after first filling the lungs to their maximum extent and them expiring to the maximum extent(about 4600 milliliters). 5. Alveolar Ventilation(VA)is the amount of new air at which reaches functional respiratory units(i.e.,alveoli,alveolar sacs,alveolar ducts,and respiratory bronchioles)per minute.VA=(tidal volume-dead space)×respiratory rate 6. Gas exchange between the alveolar air and the pulmonary blood occurs through the membranes of all the terminal portions of the lungs,not merely in the alveoli themselves. These membranes are collectively known as the respiratory membrane, also called the pulmonary membrane. It includes: (1)A layer of fluid lining he alveolus and containing surfactant that reduces the surface tension of the alveolar fluid; (2)The alveolar epithelium composed of thin epithelial cells; (3)An epithelial basement membrane; (4)A thin interstitial space between the alveolar epithelium and the capillary membrane; (5)A capillary basement membrane that in many places fuses with the alveolar epithelial basement membrane; (6)The capillary endothelial membrane. 7. Ventilation-perfusion ratio:the ratio between the amount of fresh air brought into the alveoli in the lungs and the amount of blood flow past the alveoli in the lungs. Normal Ventilation-perfusion ration=0.8. This ratio in a patient can be higher than normal(indicating “dead space”)in a patient(for a number of clinical reasons)or,of course,it can be lower than normal (“right to left shunt”)in a patient for other clinical reasons. 8. The oxygen-hemoglobin dissociation curve relates oxygen saturation(SO2) and partial pressure of oxygen in the blood(PO2) ,and is determined by what is called“hemoglobin’s affinity for oxygen , ”that is , how readily hemoglobin acquires and releases oxygen molecules from its surrounding tissue. The oxygen dissociation curve is shifted to the right ( oxygen affinity for hemoglobin is reduced)by an increase in hydrogen concentration,PaCO2,temperature and concentration of 2,3-diphosphoglycerate(2,3-DPG)in the red blood cells. 9. When the lungs become overstretched,stretch receptors,which are located in the muscular portions of the walls of the bronchi and bronchi and bronchioles throughout the lungs,transmit signals through the vagi into the dorsal respiratory group of neurons. These signals activate and appropriate feedback response that “switches off” the inspiratory ramp and thus stops further inspiration. This is called the Hering-Breuer inflation reflex. This reflex also increases the rate of respiration, the same as is true for signals from the pneumotaxic center. Ⅲ、QUESTIONS (1)CO2 respiratory activity;Peripheral mechanism and central mechanism, the latter is the main one. (2)[H+] respiratory activity;Peripheral mechanism and central mechanism, the latter is the main one. (3)PO2 respiratory activity;Peripheral mechanism is excitatory. Digestive system 1.Basic electrical rhythm(BER)or slow waves 2. Gastrointestinal(GI)hormones 3. Receptive relaxation (Storage function of the stomach) 4. Mucus-HCO3--barrier 5. Intrinsic factor 1.Digestion 2.Absorption 3.Gastric receptive relaxation 4.Intrinsic factor 5.Enterohepatic circulation of bile salts 6.body temperature 10.Gastric emptying 1. Functions of gastric acid (HCL) 2. Mucous- HCO3- barrier and it’s function 3.Composition and functions of pancreatic juice, and humoral regulation of Pancreatic secretion Ⅲ、QUESTIONS 1. Explain the gastric secretion (including the composition and physiological function of the gastric juice,the regulation of gastric secretion). 2. Describe the pancreatic secretion(including the composition and physiological function of the pancreatic juice,the regulation of pancreatic secretion). 3. Describe the biliary secretion(including the composition and physiological function of the bile). answers Basic electrical rhythm It is a kind of spontaneous ,slow and recurring depolarization and repolarization based on RP. • .Enterohepatic circulation of bile salts- nearly 95% of the bile salts are reabsorbed by the intestinal mucosa in the distal ileum, they enter the portal vein and return to the liver. On reaching the liver, the bile salts are absorbed from the venous sinusoids into the hepatic cells and then resecreted into the hepatic cells and then resecreted into the bile. gastric emptying : A process of gastric contents moving from stomach Food enter stomach –(gastric motility )pyloric sphincter muscle relaxintragastric pressure > pressure in duodenum -Gastic emptying Effective factor of gastic emptying include: 1. character of the food liquid > solid, small granulle > big granulle , isotonic solution > nonisotonic solution Glucose > protein > fat 2. factors in the stomach promote emptying(vagovagal reflex; gastrin) 3. factors in the duodenum inhibit emptying(enterogastric reflex; enterogastrone) • Digestion: It is a process essential for the conversion of food into a form that can be absorbed by the gut. Digestion is the term given to the processes whereby the complex molecules in food are dissolved and broken down into small molecules which can be absorbed from the gut • Absorption: absorption is the process of transporting small molecules produced by digestion from the mucosa lumen of the gut into blood stream and lymph 2. Gastrointestinal ( GI ) hormones are the hormones synthesized by a large number of endocrine cells within the gastrointestinal tract. They are most important in controlling digestive function,releasing other hormones and trophic action. 3. Receptive relaxation -With each swallow of food, the bolus stimulating the stretch receptors in the pharynx and esophagus, smooth muscle relaxation of proximal by a reflex mediated by the vagus nerves.(VIP, NO). significance:with the intaking of food, intragastic pressure retains invariable 4. Mucus-HCO-3-barrier -Mucus is secreted by the stomach epithelial surface cells , mucous neck cells , cardiac gland and pyloric gland . It is strong viscous.The surface mucous cells also secrete HCO3- , It can neutralise with H+ from the lumen of the stomach. this structure and its function are called Mucous-HCO3- barrier Mucus protect mucosa against mechanical injury by acid-pepsin and other agents. 5. Intrinsic factor is a glycoprotein secreted by parietal cells of the gastric mucosa. It is essential for absorption of vitamin B12 in the ileum. Ⅲ、QUESTIONS 1. 1.(1)Major components of gastric juice:①Hydrochloric:i. activates pepsinogen, convert it into pepsin. providing a medium of low pH favoring pepsin action.ii. kills bacteria iii. 4 promotes Fe++ and Ca++ absorption in initial part of small intestine. iv. Degeneration of protein and facilitates digestion v. promotes pancreatic secretion and biliation, intestinal secretion. ②Pepsinogen:Pepsin activated from pepsinogen is an endopeptidase.③Mucusco3 barrier:i.Lubrication of the mucosal surface;ii. Protection of the tissue from mechanical damage by food particles. ④Intrinsic factor:The intrinsic factor binds to Vit B12 and facilitates its absorption. 2.(1)Components of pancreatic juice:①Bicarbonate ions:Neutralizing acid enteringthe duodenum from the stomach. ②Pancreatic digestive enzymes : i. Carbohydrates : Pancreatic amylase ; ii. Fat : Pancreatic lipase , Cholesterol esterase , Phospholipase ; iii. Proteins : Trypsinogen , Chymotrypsinogen , Procarboxypolypeptidase,Proelastase. ③Trypsin inhibitor:Inhibits the activity of trypsin and thus guards against the possible activation of trypsin and the subsequent autodigestion of the pancreas. (2)Regulation of pancreatic secretion:1.Neural regulation ( vagi ):mainly stimulate enzyme secretion. parasympathetic nerve stimulation produces a scanty pancreatic secretion which is enzyme rich. This probably contributes to the cephalic and gastric phases of pancreatic secretion, which precede entry of food to the intestine(intestinal phase). Vagal nerve→Ach and gastrin →pancreatic juice↑(H2O and HCO3- low, enzyme↑) • 2.humoral control: Pancreatic secretion is most strongly stimulated by food entering the small intestine, which triggers release of two intestinal peptide hormones. • (1) secretin produced at S cells in upper end of small intestine. • Acid in the duodenum stimulates S cell release of secretin which causes secretion of a large volume of HCO3- rich fluid. • secretin →H2O and HCO3-↑enzyme low ( HCL > protein digestive products > fatty acid) • (1) CCK(Cholecystokinin) : produced at I cell in upper small intestine.Fat and peptides (not carbohydrates ) as they enter the duodenum evoke CCK release and CCK stimulates acinar cells to produce secretion containing abundant enzymes. • CCK → acinar cells • enzyme↑ H2O and HCO3- low • (protein digestive products > fatty acid > HCL, fat) • Function • secretion of pancreatic juice • Gallbladder contraction • Trophic action to pancreas ①Cephalic Phase;②Gastric Phase;③Intestinal Phase. 3. ( 1 ) Composition of bile : ①HCO-3 ; ②Bile salts ; ③Phospholipids ; ④Cholesterol;⑤Bile pigments. (2)Functions of bile:①Emulsifying or detergent function of bile salts.②Bile salts help in the absorption of:i. Fatty acid;ii.Monoglycerides;iii.Cholesterol; iv.Other lipids. metabolism 、TERMS 1. Specific dynamic action of food 3. Body temperature 2. Basal metabolic rate 4. Set-point Ⅲ、QUESTIONS 1. List the factors that affect energy metabolic rate. 2. Describe the modes of heat-loss from the skin. 3. How dose the body actively maintain a constant body temperature despite changes in ambient temperature? Answers . After a meal is ingested,the metabolic rate increases as a result of the different chemical reactions associated with digestion,absorption,and storage of food in the body. This is called the thermogenic effect of food or specific dynamic action of food. 2. Basal metabolic rate(BMR)is the mimimal caloric requirement needed to sustain life in a resting individual. BMR is usually corrected for differences in body size by expressing it as Calories per hour per square meter of body surface area. 3. Body temperature is usually referred to core temperature. 4. At a critical body core temperature,at a level of almost exactly 37.1℃,drastic changes occur in the rates of both heat loss and heat production. This crucial temperature level is called the “set point”of the temperature control mechanism. Ⅲ、QUESTIONS 1.(1)Physical Activities;(2)Psychic activity;(3)Thermogenic effect of food;(4)Environmental temperature. 2. ( 1 ) Radiation ;( 2 ) Conduction ;( 3 ) Convection ;( 4 ) Evaporation : Insensible evaporation and Evaporation of sweat. 3. When the hypothalamic temperature centers detect that the body temperature is either too high or low due to the changes in ambient temperature,they institute appropriate body temperature-decreasing or body temperature-increasing procedures to maintain a constant body temperature. Body temperature-decreasing procedures:(1)Vasodilatation;(2)Sweating; (3)Decrease in heat production. Body temperature-increasing procedures:(1)Skin vasoconstriction throughout the body;(2)Increase in heat production:Shivering,sympathetic excitation and thyroxin secretion. TERMS 1. Tubuloglomerular feedback 2. Net filtration pressure 3. Glomerular filtration rate 4. Filtration fraction 5. Filtration coefficient 6. Tubuloglomerular balance 7. Renin-angiotensin system 8. Renal threshold for glucose 9. Osmotic diuresis QUESTIONS 1. List the factors affecting glomerular filtration. 2. What are the change of urine and its mechanism when one is injected intravenously 50% glucose 100 milliliter? 3. List the factors that affect the concentration and dilution of the urine. 4. What are the changes of urine and its mechanism when one sweats a great deal and drinks little water? Answers 1. When the change of Na+ content in the renal filtrate is detected by the macula densa,a signal is sent to the renal arterial system,and the renal blood flow and glomerular filtration rate is restored to normal. 2. Net filtration pressure=Hydrostatic pressure in the glomerulus- ( Colloid osmotic pressure of plasma+Bowman’s capsule pressure) 3. The quantity of the glomerular ultrafiltrate formed each minute in all nephrons of the both kidneys. 4. The portion of the plasma that is filtered through the real glomerular membranes. Filtration fraction=GFR/Renal plasma flow 5. The product of the hydraulic conductivity and surface area of the glomerular capillaries. Kf=GFR/Net filtration pressure. 6. The ratio of reabsorption rate and Glomerular filtration rate is relatively constant. 7. The rennin-angiotensin system plays an important in regulating blood volume, arterial pressure,and cardiac and vascular function. While the pathways for the rennin-angiotensin system have been found in a number of tissues,the most important site for rennin release is the kidney. Sympathetic stimulation ,renal artery hypotension,and decreased sodium delivery to the distal tubules stimulate the release of rennin by the kidney. Renin is an enzyme that acts upon a circulating substrate ( angiotensinogen ) to release a 10-amino acid peptide , angiotensin Ⅰ.Vascular endothelium,particularly in the lungs,has an enzyme,angiotensin converting enzyme ( ACE ), that cleaves off two amino acids to form the octapeptide,angiotensinⅡ(AⅡ). 8. The critical value of the plasma glucose concentration when the kidney begins to excrete glucose. Normal value:160~180 mg/dl. 9. An increase in soluter concentration of the tubular fluid decreases the reabsorption of water,and thus increases the amount of the urine. Ⅲ、QUESTIONS 1.(1)Glomerular hydrostatic pressure Increased glomerular hydrostatic pressure increases GFR. (2)Colloid osmotic pressure of plasma Increased colloid osmotic pressure of plasma decreases GFR. (3)Bowman’s capsule pressure Increased Bowman’s capsule pressure decreases GFR. (4)Renal plasma flow Increased renal plasma flow increases GFR. (5)Glomerular capillary filtration coefficient Increased Glomerular capillary filtration coefficient increases GFR. 2. The amount of the urine would increase. After one is injected intravenously 50% glucose 100 milliliter,the amount of glucose filtered from glomerulus exceeds tubular transport maximum for glucose. The osmotic effect of the extra glucose remained in the renal tubules greatly decreases tubular reabsorption of water and solute,and causes much loss of fluid into the urine. 3.(1)Damage of renal medulla Resulting in an impairment of the concentrating ability. (2)Loop diuretics Such as frusemide,inhibiting the Na+/K+/2Cl- cotransport system in the thick ascendinglimb,and reducing the osmotic gradient in the medulla. (3)Lack of urea in the body Such as malnutrition , reducing the osmotic gradient established in the renal medulla. (4)Increased velocity of blood flow in the vasa recta Certain vasodilators can markedly increase the velocity of blood flow in the vasa recta,thereby carrying away amount of NaCl and reducing the osmotic gradient in the medulla. 4.This would cause a small volume of concentrated urine to be excreted. Sweat is fluid of low osmotic pressure. When one sweats a great deal and drinks little water,this would rapidly lead to an increase in plasma osmolarity and decreases in blood pressure and blood volume. The former causes the osmoreceptor cells in the anterior hypothalamus to fire,and the latter causes the arterial baroreceptor reflexes and the cardiopulmonary reflexes. Both stimulate the synthesis and release of antidiuretic hormone(ADH). ADH is transported to the kidneys,where it increases the water permeability of the late distal tubules, cortical collecting tubules and inner medullary collecting ducts. This results in increased water reabsorption and excretion of a small volume of concentrated urine. In addition,water loss in sweat can also increase colloid osmotic pressure of plasma and decrease net filtration pressure , leading to decreased glomerular filtration and decreased amount of urine. CHAPTER 9 SENSE ORGAN 1. All the refractive surfaces of the eye are algebraically added together and considered to be one single lens,so the optics of the normal eye is simplified and represented schematically as a “ reduced eye ” . This is useful in simple calculation. 2. The visual ability to resolve fine detail. 3. It refers to the increase in visual sensitivity with increasing time in the dark following exposure to bright light. 4. The pressure thresholds at which sounds of different frequencies can barely be heard by the ear. 5. Sound transmission mode in the air space between the external ear and the cochlea. 6. The process by which sound waves are transmitted to the inner ear by the cranial bones without traveling through the air in the ear canal. 7. An electrical potential of about +80 millivolts exists all the time between endolymph and perilymph,with positivity inside the scalamedia and negativity outside. Ⅲ、QUESTIONS 1.(1)Accommodation of lens:When an individual looks at a near object,the shape of the lens is changed from that of a moderately convex lens to that of a very convex lens. (2)Accommodation of pupils:The pupil constricts when an individual looks at a near object. This is called “Near reflex of the pupil”. (3)Convergence of eye balls:When the eye fixate on a near object,the eyes must converge. 2.(1)Scotopic vision system:not color sensitive;mainly more sensitive to light;peripheral. (2)Photopic vision system:color sensitive;less sensitive to light;mainly fovea. 3.(1)To provide a subjective sensation of movement and/or displacement in 3dimensional space. (2)To maintain upright body posture(balance). (3)To stabilize the eyes relative to the environment. 4. The motion of the basilar membrane is a traveling wave. The base of the basilar membrane(near the oval window)is three or four times narrower than the apex (the far end of the cochlea). At the base,the basilar membrane is 100 times stiffer than it is at the apex. Different frequencies of sound would lead to a different envelope of vibration on the basilar membrane with a different peak of displacement for each frequency. Therefore,different frequencies of sound would get a peak vibration in different places on the basilar membrane. The point of peak vibration of the basilar membrane would presumably cause the most bending of the cilia and elicit the most response from the hair cells in that part of the cochlea. High frequencies would cause greatest vibration near the base , and low frequencies would cause greatest vibrations near the apex. CHAPTER 10 NERVOUS SYSTEM Ⅱ、TERMS 1. Axoplasmic transport 2.Excitatory postsynaptic potential 3. Inhibitory postsynaptic potential 5. Neurotransmitter 4. Gap junction 6. Conditioned reflex 7. Specific projection system 8. Non-specific projection system 9. Referred pain 10. Spinal shock 11. Stretch reflex 12. Decerebrate rigidity 13. “Stress” response of the sympathetic system 14. Dominant hemisphere 15. EEG 16. Paradoxical sleep Ⅲ、QUESTIONS 1. What is the central inhibition? Please describe postsynaptic inhibition and presynaptic inhibition. 2. Please describe the cholinergic fibers and receptors of the body. 3. What is the sensory area of cerebral cortex? Please describe its details. 4. Describe the regulation of cerebral cortex on somatic movement. 5. What is the decerebrate rigidity? Please describe the main mechanism of it. 6. What are visceral activity regulations by hypothalamus? 7. What are the functions of Wernicke’s area,Broca’s area,the angular gyrus, and the basal ganglia in the production of speech? 8. What methods are used to study learning and memory in humans and experimental animals? 9. How do the brain waves correlate with different stages of sleep? Answer 1. Mitochondria,synaptic vesicles and other cytoplasmic constituents travel to and from the cell body by a process called axonal transport ( also called axoplasmic transport or flow). Movements of materials away from the cell body (in the same direction as signal propagation)is called anterograde transport, while movement of materials toward the cell body is called retrograde transport. 2. An electrical change ( depolarisation ) in the membrane of a postsynaptic neurone caused by the binding of an excitatory neurotransmitter from a presynaptic cell to a postsynaptic receptor;makes it more likely for a postsynaptic neuron to generate an action potential. 3. An electrical change(hyperpolarisation)in the membrane of a postsynaptic neuron caused by the binding of an inhibitory neurotransmitter from a presynaptic cell to a postsynaptic receptor;makes it more difficult for a postsynaptic neuron to generate an action potential. 4. A specialized area of apposed plasma membranes containing connexons , proteins that bridge the extracellular space and that allow the cytoplasm of one cell to communicate with that of the other cell. 5. Small molecules that are liberated by a presynaptic neuron into the synaptic cleft and cause a change in the postsynaptic membrane potential. 6. An acquired response that is under the control of(conditional on the occurrence of)a stimulus. 7. The projecting system of thalamic relay nuclei ( ventral posterior nuclei , medial & lateral geniculate nuclei)receives fibers from ascending somatosensory pathways and projects mostly to a localized(discrete)region of the cortex-focal projection. 8. Non-specific projection system Intralaminar nuclei,dorsomedial nucleus,pulvinar & lateral posterior nucleus are all examples of thalamic nuclei that receive afferent fibres from reticular formation and contain diffuse projections to association cortex ( or to other thalamic areas)and send fibers to very broad regions of cortex-diffuse projection. 9. A person feels pain in a part of his or her body that is considerably remote from the tissue causing the pain. 10. Spinal shock is a state of transient physiological(rather than anatomical) reflex depression of cord function below the level of injury with associated loss of all sensorimotor functions. 11. Reflex contraction of a muscle when an attached tendon is pulled. It is important in maintaining erect posture. 12. Extension of the trunk and the four limbs due to impairment to the mesencephalon. It is accompanied by an irreversible coma and disintegration of vital signs. 13. A mass discharge of the sympathetic system increases in many ways the ability of the body to perform vigorous muscle activity. They increase heart rate and blood pressure,delivering more oxygen and blood sugar to power important muscles, and so on. 14. The side of the brain that controls language function is usually the side opposite to the handedness of the person and is referred to as the dominant hemisphere by definition. The general interpretative function of Wernick’s area and the angular gyrus as well as the functions of the speech and motor control areas are usually much more highly developed in this hemisphere than in the other. 15. A graphical record of electrical activity of the brain ; produced by an electroencephalograph 16. Rapid eye movement sleep(REM sleep),a recurring sleep state during which dreaming occurs;a state of Rapid Eye Movements during slee. Ⅲ、QUESTIONS 1. Central inhibition is also called synaptic inhibition which is the inhibition between neurons. Postsynaptic inhibition:①Involves direct contact between inhibitory synapse and neuron being inhibited ; ② Typically involves hyperpolarization-IPSP ; ③ Involves inhibitory inter-neuron. Types of postsynaptic inhibition : Afferent Collateral Inhibition and recurrent Inhibition. Presynaptic inhibition : ① Inhibitory synapse onto presynaptic terminal of excitatory synapse;②Post-synaptic inhibition momentarily reduces ability of cell to respond to excitatory input ; ③ Presynaptic inhibition reduces amount of neurotransmitter released from an excitatory terminal;④Works by reducing Ca2+ influx into presynaptic terminal,therefore reducing amount of neurotransmitter released. 2.(1)The cholinergic fibers:①Sympathetic and parasympathetic preganglionic fibers ; ② Parasympathetic postganglionic fibers ; ③ Motor nerve fibers ; ④ Sympathetic postganglionic fibers to the sweat glands;⑤Sympathetic vasodilator nerve fibers of the muscles. (2)The cholinergic receptors:M-,N1-,N2-receptor 3. Sensory areas of cerebral cortex (1)Somatosensory cortex Somatosensory area Ⅰ:Brodmann’s areas:3-2-1 Somatosensory area Ⅱ (2)Proprioception sensory area(4) (3)Visual cortex Primary visual cortex(17) Secondary visual areas(18,19) (4)Auditory cortex(41,42) Primary auditory cortex Secondary auditory areas 4. Transmission of signals from the motor cortex to the muscles (1)Pyramidal system(Corticospinal tract) Pathway:Motor cortex(pyramidal cells)→internal capsule→forming the pyramids of the medulla→cross to the opposite side in the lower medulla→spinal cord(motor neurons); Function:It is the direct pathway which concerned more discrete and detailed movements. (2)Extrapyramidal system The accessory pathway that involve the basal ganglia,cerebellum,and nuclei of the brain stem 5.(1)Decerbrate rigidity:Extension of the trunk and the four limbs due to impairment to the mesencephalon. It is accompanied by an irreversible coma and disintegration of vital signs. (2)Mechanism:Blockage of the input to the medullary reticular nuclei from the cerebral cortex,red nuclei and basal ganglia;Medullary reticular inhibitor system becomes nonfunctional;Overactivity of the pontine excitatory system. 6.(1)Cardiovascular Regulation (+)posterior and lateral hypothalamus↑BPA,HR (+)preoptic hypothalamus↓BPA,HR (2)Regulation of body temperature PO/AH(the preoptic area) (3)Regulation of body water Thirst center Supraoptic nucleus:secrete ADH (4)Regulation of uterine contractility and milk ejection Paraventricular nucleus:oxytocin (5)Gastrointestinal and feeding regulation Ventromedial nucleus:satiety center Lateral hypothalamic area:feeding center Mammillary bodies:feeding reflexes (6)Hypothalamic control of endocrine hormone secretion by the anterior pituitary gland (7)Behavioral functions Lateral hypothalamus is involved in controlling rage and fighting Ventromedial nucleus is involed in satiety , decreased eating , and tranquility Thin zone of the periventricular nucleus is involved in fear and punishment, sexual drive (8)Controlling biorhythm Suprachiasmatic nucleus 7. Wernicke’s area:Language comprehension. Broca’s area:Controls facial neurons. Controls speech. Understanding language. The angular gyrus:It is important in the processing of associating a heard name to a seen or felt object,it is probably also important for associations in the reverse direction。 The basal ganglia:The basal ganglia appear function as a “sequencing engine” , allowing humans to speak and to create new patterns of though and to create a potentially limitless number of novel sentences by permuting a finite number of words and syntactic processes. 8. fMRI and PET are usually used for humans for studying learning and memory. As for experimental animals,hippocampus is the most common brain area for research of Synaptic plasticity during learning and memory,and the cerebellum is the area for studying motor memory. The method used for animals is recording the local field potentials in the above two areas with the presynaptic fibers electrically stimulated and to analyze the long-term potentiation ( LTP ) or long-term depression(LTD). 9.(1)Slow-wave sleep EEG:Low-frequency,highly synchronized neural activity Stage 1,2,3,4 (2)Fast-wave sleep EEG:high-frequency,small amplitude,desynchronized wave Endocrine TERMS 1. Hormone 2. Permissive action 3. Hypothalamic regulatory peptide 4. Growth hormone 5. Thyroid Hormones 7. Stress 6. Glucocorticoid 8. Insulin Ⅲ、QUESTIONS 1. Name the hormones secreted by the hypothalamus in humans,and list the main functions of each. 2. What are the mechanisms of action of peptide/protein hormones? 3. List the main physiological actions of thyroid hormones. 4. What are the endocrinologic causes of dwarfism and cretinism,and how does each lead to short stature? 5. Describe the functions of cortisol and the mechanisms that regulate secretion of glucocorticoids. 6. Describe the effects of insulin. 7. What are the disadvantages of long-term , high dose treatment with glucocorticoids in diseases such as rheumatioid arthritis and asthma? What problems occur when steroid treatment is stopped suddenly? Chemicals produced by glands or specialized cells in a small amount that are released into the circulating blood to influence the function of cells at another location in the body and chemicals that have paracrine and autocrine functions. 2. The permissive hormone is an absolute requirement for the actions of another hormone,but may be without noticeable effect of its own. 3. Polypeptide hormones synthesized and secreted by special neurons in the hypothalamus to control secretion of the anterior pituitary hormones 4. Growth hormone,also called somatotropic hormone or somatotropin,is a small protein molecule. It causes growth of almost all tissues of the body that are capable of growing. 5. Thyroid Hormones are thyroxine and triiodothyronine,commonly called T4 and T3,respectively. They have the profound effect of increasing the metabolic rate of the body. 6. Glucocorticoids are secreted by the adrenal cortex. Glucocorticoid is a compound that belongs to the family of compounds called corticosteroids (steroids). Glucocorticoids affect metabolism and have anti-inflammatory and immunosuppressive effects. 7. Trauma,surgery,infection,intense cold or heat,nervousness and anxiety, can cause an immediate and great increase in adrenocorticotropic hormone (ACTH)secretion by the anterior pituitary gland,followed by marked increase of adrenocortical secretion ,mainly cortisol in human. Increased cortisol may cause mobilization of amino acids and fatty acids from their cellar stores,making them rapidly available both for energy and for synthesis of other compounds (i.e.Glucose)which are needed by the vital organs of the body. This is called the stress response. 8. Insulin is a protein hormone secreted by the isles of Langerhans in the pancreas;It regulates storage of glycogen in the liver and accelerates oxidation of sugar in cells. Ⅲ、QUESTIONS 1. Name Target Hormone Secretion Releasing Hormone(or Factor) Thyrotropin releasing hormone(TRH) TSH Gonadotrpin releasing hormone(GnRH,LHRH) LH, FSH Corticotropin releasing hormone(CRH) ACTH Growth hormone releasing hormone(GHRH) GH Melanocyte stimulating hormone releasing factor ( MRF ) MSH Prolactin releasing factor(PRF) PRL Releasing Inhibiting Hormone Growth hormone release inhibiting hormone GH, TSH,insulin (GHRIH,somatostatin) Prolactin release inhibiting factor(PIF) glucagons,gastrin PRL,MSH Melanocyte stimulating hormone release inhibiting factor(MIF) MSH 2.(1)The binding of the hormone to its specific receptor of the target cell. (2)A change in the configuration of the receptor,which becomes activated. (3)The receptor activation leads through a sequence of reactions to the cell’s ultimate response to the hormone. The mechanisms of signal transduction involve three classes key substances in sequence:the G protein,second messengers and protein kinases. The principle second messengers are cAMP,IP3,DG and Ca2+. 3.(1)Effects of thyroid hormone on general metabolism Thyroid hormone exerts numerous effects on metabolic processes in a wide variety of different tissues and cells. a)Calorigenesis or the heat production and BMR in the body; b)Glucose absorption from the intestine and increase the uptake of glucose from the blood into adipose tissue and muscle; c)All aspects of lipids. In general,however,the degradation is affected more than synthesis; d)Protein synthesis when present in physiological concentrations. However, when the thyroid hormone is present in excess,it tends to cause a decrease in protein synthesis and an increase in protein breakdown. ( 2 ) Cardiac output by increasing both the rate and the strength of cardiac contraction. Systolic blood pressure is augmented and diastolic blood pressure is decreased,so that the net result is a widened pulse pressure. (3)Effects of the thyroid hormone on growth and development. The thyroid hormone is required for normal skeletal growth. Development and maturation of the central nervous system are markedly affected by thyroid hormones. 4.(1)Dwarfism can be duo to GRH deficiency,growth hormone deficiency, deficient secretion of IGF-I,or other causes in childhood. (2)Cretinism can be due to deficiency of thyroid hormone during the period of fetal and early neonatal development. (3)Short stature is the result of the disproportionate growth of the skeleton. Growth hormone and thyroid hormones are required for normal skeletal growth. They can regulate the growth of bone. 5.(1)Functions of cortisol: 1)Effect on metabolism Blood glucose concentration by stimulating gluconeogenosis by the liver and the rate of glucose utilization by the cells. Protein store in extrahepatic tissues by protein synthesis and catabolism of protein already in the cells. Mobilization of fatty acids from adipose tissue and oxidation of fatty acids. The patients with excess cortisol secretion develop a peculiar type of obesity with excess deposition of fat in the abdomen,trunk and face,giving a buffalo-like torso and rounded face,a “moon face”. 2)Effect of cortisol in stress Cortisol is resistant to stress. 3)Effect of glucoticoids on some organs and tissues Vascular System : Cortisol permits normal responsiveness of arterioles to the constrictive action of catecholamines by decreasing the degradation of catecholamines. Cortisol is required fore the maintenance of normal blood pressure. Blood cells:The number of red blood cells,platelet,and neutrophils and the number of eosinophils and lymphocytes in the blood. Central Nervous System : The brain possesses receptors for adrenal glucocorticoids. (2)Regulation of glucocorticoids secretion: The glucocorticoid secretion is regulated by feedback mechanisms. CRH:ACTH synthesis and secretion ACTH:Glucocorticoid(cortisol)synthesis and secretion,inhibits the release of CRH through a short-loop feedback Cortisol:inhibits pituitary ACTH synthesis and secretion through negative(longloop ) feedback. Cortisol also has direct negative feedback effects on the hypothalamus to decrease the formation of CRH. All these feedbacks help regulate the plasma concentration of cortisol. 6.(1)Effects of insulin on carbohydrate metabolism The insulin causes rapid uptake,storage,and use of glucose by almost all tissue of the body especially by liver,muscle,and adipose tissue, (2)Effect of insulin on fat metabolism. Insulin rapidly lowers the circulating levels of free fatty acids and ketoacids and may eventually decrease the level of triglycerides. The net effect of insulin on fat metabolism is to increase storage and to block mobilization and oxidation of fatty acids. (3)Effect of insulin on protein metabolism and on growth Insulin increases protein synthesis , especially the enzymes for storage of carbohydrates,fats and proteins. Insulin inhibits the catabolism of proteins. It is equally as essential for growth of an animal as is growth hormone. 7. The disadvantages of long-term,high dose treatment with glucocorticoids: Pituitary inhibition ACTH secretion decrease Adrenal insufficiency, When steroid treatment is stopped suddenly: Lack of glucocorticoids Reproduction 1. Testosterone 2. Estrogen 3. Progesterone 4.Menstrual cycle Ⅲ、QUESTIONS Describe the roles of the pituitary and the hypothalamus in the regulation of ovarian function,and the role of feedback loops in this process. ANSWERS 1. A steroid hormone which is necessary for male sexual reproduction and may also play a role in female sexual response. It is responsible for male secondary sexual characteristics. In males,it is produced in the Leydig cells of the testes;in both sexes,it is produced in smaller quantities by the adrenal glands. 2. A steroid hormone secreted mainly by the ovaries. It affects many aspects of the female body,including menstrual cycles and pregnancy. 3. A steroid hormone which is secreted by the corpus luteum of the ovary and is produced by the placenta during pregnancy ; it can regulate changes in the endometrium of the uterus. 4. Menstrual cycle is the reproductive cycle of female humans. The cycle is characterized by a monthly discharge of blood,mucus,and tissues from the uterus(called menstruation)and involves changes to the endometrium of the uterus during the rest of the month including a few days of fertility after an ovum is released by an ovary. Ⅲ、QUESTIONS (1)The hypothalamic-pituitary-ovarian(HPO)axis GmRH:synthesis and release of FSH and LH FSH:stimulating the ovarian follicles to develop and to secrete estradiol LH:luteotrophic,progesterone production by the corpus luteum ( 2 ) Estrogen and progesterone exert negative feedback effect on the hypothalamus and the anterior pituitary to decrease GnRH and gonadotropin release via long feedback loop. Gonadotropins may inhibit the secretion of GnRH(via short feedback loop) GnRH may exert an inhibitory effect on its own secretion ( via ultra short feedback loop) (3)The preovulatory rise in estrogen may exert positive feedback effect on the hypothalamus to increase GnRH release. The positive feedback effect of the preovulatory rise in estrogens is also augmented by the small increase in progesterone that occurs around the time of the gonadotropin surge ( before ovulation). ( 4 ) Inhibin also plays a significant role in the feedback regulation of gonadotropin secretion.