disaster management and public health experience in the aftermath
advertisement

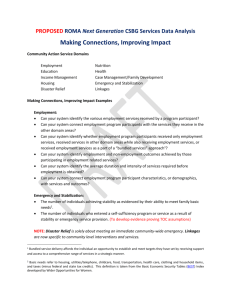
DISASTER MANAGEMENT AND PUBLIC HEALTH EXPERIENCE IN THE AFTERMATH OF THE EARTHQUAKE AT BHUJ IN INDIA Dr HS Ratti, MD India DATE 1819 JUN 16 1869 JAN 10 1885 MAY 30 1897 JUN 12 1905 APR 04 1918 JUL 08 1930 JUL 02 1934JAN 15 1941 JUN 26 1943 OCT 23 1950 AUG 15 1956 JUL 21 1967 DEC 10 1975 JAN 19 1988 AUG 06 1988 AUG 21 LOCATION MAGNITUDE KUTCH,GUJARAT 8.0 NEAR CACHAR, ASSAM 7.5 SOPOR, J&K 7.0 SHILLONGPLATEAU 8.7 KANGRA, H.P 8.0 SRIMANGAL, ASSAM 7.6 DHUBRI, ASSAM 7.1 BIHAR-NEPALBORDER 8.3 ANDAMAN ISLANDS 8.1 ASSAM 7.2 ARUNACHAL PR – CHINA BDR 8.5 ANJAR, GUJARAT 7.0 KOYNA, MAHARASHTRA 6.5 KINNAUR, HP 6.2 MANIPUR-MYANMAR BORDER 6.6 BIHAR-NEPAL BORDER 6.4 SIGNIFICANT EARTHQUAKES IN INDIA AND ITS NEIGHBOURHOOD (1801 - 2000) DATE LOCATION 1991 OCT 20 MAGNITUDE DEATH UTTARKASHI, UP HILLS 1993 SEP 30 LATUR- 1997 MAY 22 JABALPUR,MP 1999 MAR 29 CHAMOLI DIST, UP 6.6 6.3 INJURED 769 7601 6.0 39 6.8 103 16000 ANTICIPATED PUBLIC HEALTH PROBLEMS IN DISASTERS 1 Disruption of Water supply and Sanitation 2 Large scale migration 3 Overcrowding due to emergency housing situations with poor personal hygiene 4 Mass feeding without adequate food handling, storage and sanitary facilities 5 Disposal of Dead Bodies and Caracas 6 Rodent and Stray dog/animal problems 7 Relaxation of sterilization precautions and emergency use of unscreened blood 8 Psycho-social and Mental health problems COMMUNICABLE DISEASES HAVING DISASTER IMPLICATIONS (HAVING POTENTIAL FOR OUTBREAK) 1.Amoebiasis 2.Camplyobacter Enteristis 3.Chicken Pox 4.Cholera 5.Coccidiomycosis 6. Dengue fever 14. Leptospirosis 15. Malaria 16. Measles 17. Meningitis 18. Pertusis 7.Diptheria 19. Plague 8.E. Coli Diarrhoea 20. Pnuemococcal Pneumonias 9.Food Poisoning 21. Rabies 10.Rotavirus Enteritis 22. Relapsing Fever 11.Hepatitis A, B & E 23. Salmonellosis 12.Hanta Virus Disease 24. Scabies 13.Influenzae 25. Typhoid Fever 26 Jan 2001 at 0856 AM (IST), Bhuj in western India and its surrounding areas were struck with severe earthquake, measuring 7.9 on the Richter scale CRATER FORMED AT THE EPICENTRE AT DHORI LINEAR CRACK AT THE EPICENTRE AT DHORI LAVA LIKE MATERIAL SPROUTED AT THE EPICENTRE DESTRUCTION LEFT BEHIND BY THE EARTHQUAKE Mortality and Morbidity • Dead 19727 • Injured 1,66,000 • Homeless 6,00,000 • House Destruction total : 3,48,000 • House Destruction partial : 8,44,000 • Total cattle Killed : 20,000 • Direct Estimated Economic Loss :USD 1.3 bn • Large scale migration of inhabitants • Large scale scale influx of relief workers & material Relief Agencies at work • • • • • • • International NGOs : 55 National /Local NGOs : 26 Government Bodies :8 Donor Governments :18 Inter Governmental Organisations :8 Red Cross and Red Cresent :6 Total Organisations (2 weeks) :125 • Immediate 48-72 hrs Relief and Rescue provided by Indian Army Teams and the Indian Army Hospital • 12000 surgical operations performed in makeshift Military Hospital within first 60 hrs of the Disaster Public Health Measures • Situation Assessment • Public Health Measures – Water Borne disease – Air Borne infections – Vector borne diseases – Biomedical wastes – Disease Surveillance – Dead Bodies and Animal Caracas Disposal – Disinfecting of Rescue Sites and Teams – Mental Health CLIMATIC CONDITIONS PREVAILING IN BHUJ IN FIRST WEEK OF FEB 2001 Day Time Night Time RH Rainfall Max 330 C 190 C 72 Nil Min 220 C 090 C 61 Avg Temp 210C Gujarat State has experienced Drought Conditions since 1998 Water Borne disease • Threat potential – Breakdown of distributed piped water supplies and water requirement being met from alternate sources – Drinking water available only from 4 to 5 deep bore wells scattered over the whole town and nearby villages in the Public Health Engineering Department. – Drinking water is highly salty and at places turbid (due to earthquake). – The water is collected by water truck/water bowsers/tankers and distributed manually Water Borne disease • Intervention – The bore well water is collected in sump. – Flocculation and sedimentation in the sump was carried using Alum for a period of atleast 4 hours – It is followed by super chlorinating at 2 ppm with liquid chlorine and/or bleaching powder with a contact period of minimum 20 minutes – All water bowsers/tankers leaving the water point were checked for free chlorine levels and due records were kept. Water Borne disease • Outcome – 70 to 75 percent of population was getting chlorinated water supply. – A 8000 litre desalination plant received as gift from USAID was installed for exclusive issue of drinking water. –There were no cases of Gastro Intestinal diseases among population in 3 week post disaster period. –A close monitoring has been instituted combined with disease surveillance Air Borne disease • Threat potential – All pers and families living in tentage and makeshift arrangements – Inadequate supplies of tentage resulting in overcrowding by a factor of 80 to 100 percent. – Sharp and high difference in max and min temp (max daytime temp of 34 to 36 degrees centrigade while min night temp was 8 degrees centigrade) – Season ideal for Chicken pox, measles and meningitis outbreaks – Potential of outbreak of Bubonic plague was kept in mind in view of earthquake disaster • Intervention Air Borne disease – Health education campaign was undertaken to ensure that there was minimal over crowding in tentage accommodation. A minimum distance of 3 feet was advocated – To adopt a head-foot alternate bed positions – Adequate ventilation of tentage and exposure to sun during daytime was adovacated – Provision of adequate warm clothing – Field and Hospital based Passive Disease surveillance – Active surveillance by random interviews was carried out in select areas of high density. Every day, a new area was visited. Health advice was given. Air Borne disease • Outcome – There were 4 cases (all adult males) of chicken pox reported between 7 to 8 Feb in military areas and 31 cases among civil population in samkhayali village near Bachao. Of these, 28 were children under 12 years of age and 3 adults – Outbreak control measures included segregation and symptomatic treatment of the affected individuals – All cases recovered and no secondary outbreak of communicable diseases was reported in military and civil areas till 3 weeks after last case Vector Borne disease • Threat perception – No piped distribution of water supply leading to places with water point collection – Inadequate disposal of liquid and solid wastes leading to fly nuisance – Inadequate disposal of Bio Medical waste Vector Borne disease Intervention – Spraying operations using 0.1 % NUVAN (Dicholorvos) solution in the areas where solid waste were disposed – Daily sprinkle of Lime Slaked powder over and around the Deep Trench/Shallow Trench latrines used for excreta disposal in temperory shelters put up for living – ‘Smoking’ of the Deep trench latrines to prevent and fly breeding – Spray water collection pockets with anti larval measures - Baytex 1000 Conc and/or Baytex granules or Abate (Temephos 0.5%) – Space spraying of tentage accommodation with Baygon and /or Malathion 50 % EC (in 0.5 % solution) Bio Medical Waste • Large quantity of Biomedical waste was generated in the areas in military hospital and other places in whole of district of Bhuj following disaster. • No incineration facilities are available except in the military hospital where rudimentary and sufficient facilities are available only for routine workload • The waste was segregated into open pits at a distance from the hospital and burnt in the beehive incinerator over a period of 7days • Other non biodegradable waste like plastics, IV Sets, were disposed by deep burial in open ground • Biological medical waste generated in other areas including animal dead was strewn all around in Bhuj district and posed a potential public health problem Disease Surveillance • Active Disease surveillance in 10 relief centres were established in and around Talukas of Bhuj district - Khavda, Anjar, Baccaho (2 centers), Samkhyali, Ratanpol, Modvadar, Dhori, Dharan and Mandvi. • Passive Disease surveillance launched in consultation with WHO Teams and the State Health authorities •Each relief centre had a team of one Medical Officer and Two Nursing Assistant. Besides, additional Mobile Teams from each centre were sent out daily to cover different villages. •No mass immunisation was recommended. However, UNICEF promoted mass vaccination against measles for all children 9 mths - 5 yrs was undertaken in the the Kutch areas by the state health authorities Disinfection of Rescue Sites and Teams • Personal Protective Measures – Gloves, Face Masks and Head Protection • Disinfecting The Dead Bodies with 40% Formalisn and 10 % Creosol Solution • Deodourisation of the work are at the relief site MENTAL HEALTH •Acute Post Stress Disorder •In need of Post Traumatic Counseling A much relieved lady rescued after 96 hours. REHABLITAION & RECONSTRUCTION First steps towards future ?