(unless you are a graduating senior), there is no
advertisement
, there is no")
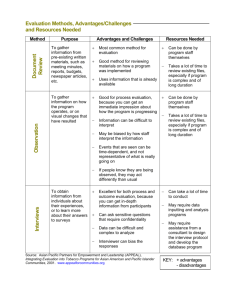
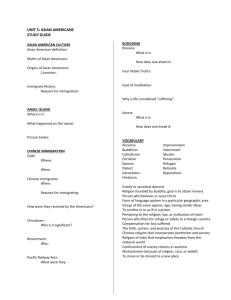
HPRF 135 Jerry M. Kaiser jkaiser@casa.sjsu.edu www.schoolrack.com/jkaiser/files 924-7480 1. Check and sign the roster: Name, preferred name, e-mail 2. Adding the class: Graduating seniors first (with letter from advisor); seniors next (first, if you were here last week, and then by lottery). There are not enough spaces for all seniors and none available for juniors. If you were not here last week (unless you are a graduating senior), there is no space available. 3. Required: 3x5 cards at beginning and end of class. Put them in the box on the desk. 1. Beginning: 3 comments and/or questions about the assignment 2. End: 1 comment and/or question about the class 4. If you are miss class or arrive late, you are responsible for work and assignments. See Greensheet for late policies. 5. Course reader is in the bookstore - not print shop. Ignore content which does not relate. Cultural Concepts: • Attitude – State of mind or feeling about some matter of a culture – Attitudes are learned • Belief – Accepted as true – Tenet or body of tenets accepted by people in an ethnocentric group. – Do not have to be proven • Ideology – Thoughts and beliefs which reflect social needs and aspirations of an individual or an ethno-cultural group Activity • In groups of 4, discuss one of your – Attitudes – Beliefs – An ideology that you share Culture • The totality of socially transmitted behavioral patterns, arts, values, customs, lifeways and all other products of human work and thought characteristics of a population of people that guide their worldview and decision-making. • May be explicit or implicit. • Primarily learned and transmitted in family • Shared by most members of the culture • Emergent phenomena that change in response to global phenomena • Largely unconscious and has powerful influences on health and illness. • Discuss: Cultural Climate at SJSU Cultural awareness • Appreciation of signs of diversity Cultural sensitivity • Attitudes, behaviors, possibilities Cultural competence • Developing an awareness of one’s own existence, sensations, thoughts and environment without letting it have an undue influence on those from other backgrounds. • Demonstrating knowledge and understanding of the client’s culture, health-related needs and meanings of health and illness • Accepting and respecting cultural differences • Not assuming that the healthcare provider’s beliefs and values are the same as the client’s • Resisting judgmental attitudes such as “different is not as good.” • Being open to cultural encounters • Adapting care to be congruent with the client’s culture. Cultural competence is a conscious process and not necessarily linear. The progression toward cultural competence • • • • Unconscious incompetence Conscious incompetence Conscious competence Unconscious competence • “To be even minimally effective, culturally competent care must have the assurance of continuation after the original impetus is withdrawn; it must be integrated into, and valued, by, the culture that is to benefit from the intervention.” Ethnocentrism • “The universal tendency of human beings to think that their ways of thinking, acting, and believing are the only right, proper, and natural ways. Values • Principles, and standards that have meaning and worth to an individual, family, group, or community • The extent to which one’s cultural values are internalized influences the tendency toward ethnocentrism. Primary Characteristics of Culture • • • • • • Nationality Race Color Gender Age Religious Affiliation Secondary Characteristics of Culture • • • • • • • • • • • • • • Educational status Socioeconomic status Occupation Military experience Political beliefs Urban v. rural residence Enclave identity Marital status Parental status Physical characteristics Sexual orientation Gender issues Reason for migration Length of time away from country of origin Immigration Status and Worldview • Voluntary immigrants acculturate more willingly • Assimilate more easily 12 domains of culture a. b. c. d. e. f. g. h. i. j. k. l. Overview, inhabited localities, and topography Communication family roles workforce issues biocultural ecology high-risk behaviors nutrition pregnancy and childbearing practices death rituals Spirituality health care practices health care practitioners Overview, inhabited localities, and topography 1. Country of origin 2. Current residence 3. The effects of the topography of country of origin and current residence on health 4. Economics 5. Politics 6. Reasons for migration 7. Education status 8. Occupations Communication • • • • • • • Dominant language Dialects Cultural communication patterns Personal space Body language Touch Temporal relationships • Format for names Family roles and organization • • • • • • • • • • • • The head of the household Gender roles Family goals and priorities Developmental tasks of children and adolescents Roles of the aged Roles of extended family members Individual and social status in the community Acceptance of alternative lifestyles Single parenting Nontraditional sexual orientations Childless marriages Divorce Workforce issues • • • • • • • Autonomy Acculturation Assimilation Gender roles Ethnic communication styles Individualism Health care practices from the country of origin Biocultural ecology • • • • Skin color Body type Diseases that are genetic, hereditary, topographic or endemic How the culture metabolizes drugs High-risk behavior • • • • • • • • Drug use Alcohol use Nicotine use Dangerous behaviors Use of safety equipment (seat belts, helmets) High risk behaviors (sexually or otherwise) Degree of sedentary lifestyle Consumption of unhealthy food Nutrition • • • • Availability of food Rituals and taboos associated with food The meaning of food to the culture How food is used in sickness and in health Pregnancy and childbearing practices • Fertility practices • Labor and delivery practices • Practices that are considered taboo, prescriptive or restrictive during pregnancy • Labor and postpartum Death rituals • • • • • How death is viewed Euthanasia Preparation for death Burial practices Bereavement practices Spirituality • Practices that give strength and meaning of life to a individual • Religious practices • How prayer is used Health care practices • • • • • • Does the culture seek preventative or acute treatment? Magicoreligious healthcare beliefs Traditional practices Individual responsibility for health Self medicating practices Views towards issues such as – Organ donation – Mental illness – Rehabilitation • How pain is expressed • The sick role • Barriers to health care Health care practitioners • Type of practitioners the culture uses – Traditional, or folk – Biomedical • Does gender of the practitioner comes in to play? • What is the status the practitioner has in this culture? Ethnicities • • • • • White African American American Indian and Alaskan Native Asian Native Hawaiian and other Pacific Islander • “some other race”; I.e., unable to identify with other categories. Nation American Indian/Alaska native 1% Other Race 0.17% Two or More Races 2% Asian 4% Hispanic 13% Pacific Islander 0.13% African American 12% White 68% California American Indian/Alaska native 1% Other Race 0.17% Two or More Races 3% Asian 11% White 47% Hispanic 32% African American 6% Pacific Islander 0.13% SJSU Student Body Pacific Islander 1% Filipino 7% Other Hispanic 4% White 25% Not stated 17% African American 4% American Indian/Alaskan 1% Mexican American 10% Asian 31% Comparative Demographics 70 60 50 40 Nation California SJSU** 30 20 10 0 **17% not stated White Hispanic Asian African American Determinants of Health Percent of U.S. Deaths 45 40 35 30 25 20 15 10 5 0 40 30 20 10 Behavioral Patterns Social Circumstances and Environmental Exposures Genetics Inadequacies in medical care Influences on the Health of Individuals QuickTime™ and a TIFF (LZW) decompressor are needed to see this picture. Life Expectancy, in years, at birth American Indian Hispanic Asian/Pacific Islander Black White 60 65 70 75 80 Life expectancy for an African American baby boy born today is about the same as for a white born in 1950 85 Hispanic Health Differences (deaths per 100,000) 32 10 Puerto Rican women 32 Puerto Rican Men Cuban Women 1 217 57 291 11 Diabetes HIV/AIDS Heart disease 92 10 24 Cuban Men Mexican Women 12 13 Mexican Men 10 16 0 170 85 110 100 200 300 400 Percent of men who smoke Laotian Korean Vietnamese Filipino Chinese Japanese Asian and pacific Islander 0 20 40 60 80 Immigration History and Policy 1882 The Chinese Exclusion Act of 1882 suspends immigration of Chinese laborers under penalty of imprisonment and deportation. • 1898 Philippines became American possession, and Filipinos were designated “nationals”. • 1907 The United States and Japan form a “Gentleman’s Agreement” in which Japan ends issuance of passports to laborers and the U.S. agrees not to prohibit Japanese immigration. • 1913 California’s Alien Land Law rules that aliens “ineligible to citizenship” were ineligible to own agricultural property. • 1917 Immigrants required to pass a literacy test, excluded virtually all Asians. • 1922 The Supreme Court rules in Ozawa v. United States that first-generation Japanese are ineligible for citizenship and cannot apply for naturalization. • 1924 Immigration Act of 1924 establishes fixed quotas of national origin and eliminates Far East immigration. • 1934 U.S. Supreme Court ruled the “White persons” meant Caucasian, and excluded Chinese, Japanese, East Asians (Hindus), American Indians, and Filipinos. These groups were excluded from citizenship. Also, quotas were placed on Filipino entries and some were repatriated. Immigration History and Policy • 1942 Bracero program initiated, allowed temporary workers • 1943 Quota system changed to allow a few restricted aliens to enter. For example, 100 Chinese a year were allowed. The Chinese Exclusion Act was repealed • 1950 Aliens required to register • 1952 Immigration of a few additional Asians allowed; also some refugees were allowed. • 1964 End of Bracero program • 1965 Old quotas based on country of origin were dropped; Asians no longer restricted and Europeans no longer favored. Preference categories favored entry of family members and of professionals, effective 1968. Allowed admission of refugees. • 1970’s-80’s Most immigrants have been from Latin America and Asia: Vietnam, S.E. Asia, Cuba, and Haiti. In addition, many illegal immigrants enter every year; especcially from Mexico. • 1986 Amnesty for undocumented workers in U.S. since 1982 • 1990 Increased immigration ceiling from 500,000 to 700,000 annually until 1995 • 2001 Patriot Act creates significant new restrictions on immigration procedure in an effort to combat terrorism. • Discuss: Effects of immigration on U.S. Asssignments: For February 6 • Ch. 2, p. 14-21, 21-23 • 1-2 pages: Who am I, related to 12 domains. • Course adds: – add number by department Worldmapper: Maps of Inequalities Public Health Spending Private Health Spending Early Neonatal Mortality HIV/AIDS Prevalence Malaria Cases Medical Myths: Kurdistan • 1. 2. 3. 4. 5. 6. 7. 8. 9. medical myths common among our local populations, having no sound scientific basis & include: Acidic food as lemon are good for hypertension. Bitter food are good for diabetes. Honey & dates are safe for diabetics. Typhoid & measles patients should not eat yougurt. Typhoid, measles & infleunza patients should not have a bath untill cured. Jaundice clears by looking at moving fish in water. Whooping cough can be cured by passing through tunnels. Inhalers for asthma are addicting. Garlic prevents heart disease & lowers blood pressure.