Integumentary System - Practicum-Health-Science-II-2010-2011
advertisement

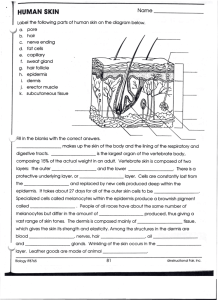
Integumentary System HST III 2009-2010 Objectives: After completing this unit each student should be able to: • Compare the composition and function of the epidermis with those of the dermis • Describe the functions of the skin. • Describe normal hair, nails, sebaceous glands, and sudoriferous glands and their primary functions. Objectives: 4. Give examples of the appropriate health history questions for assessment of the skin, hair, and nails. 5. Describe how to assess thee client’s skin by inspection and palpation. 6. Differentiate between normal and abnormal skin conditions. 7. Describe the characteristics of common skin lesions using appropriate terminology. Objectives: 8. Identify life-threatening drug induced skin eruptions. 9. Describe the general dermatologic preparations and their indications. 10. Discuss ectoparasitic diseases and the use of topical ectoparasiticidal drugs in their treatment. Anatomy and Physiology Considered to be both: • (a) Membrane – covers the body • (b) Organ – contains several types of tissue – Largest organ in body covering (c) 3,000 square inches – About (d) 15% total body weight Tissue: • 3 layers of tissue 1. (e) Epidermis – outermost layer of skin • (f) NO blood vessels or nerve cells (avascular) 2. (g) Dermis – corium or “true skin” • Includes: –Elastic connective tissue –Blood vessels –Lymph vessels –Nerves –Involuntary muscle –Sweat and oil glands –Hair follicles Tissue: Subcutaneous layer (hypodermis) – the innermost layer 3. (h) • Made of: • • • Elastic and fibrous connective tissue Adipose (fatty) tissue Connects the skin to underlying muscles Fingerprints? • The top layer of the dermis has ridges which form lines or striations on the skin which give us our unique fingerprints Major Organs/Structures • • • • Skin Sweat and oil glands Nails Hair Two Main Types of Glands Sudoriferous (sweat) glands 1. (i) • • • Sweat eliminated by these glands contains water, salts, and some body wastes Sweat is odorless until it interacts with bacteria on the skin Perspiration (sweating) removes excess water from the body and cools the body Two Main Types of Glands 2. (j) • • • • Sebaceous (oil) glands Usually open onto hair follicles Produce sebum (oil) which keeps skin and hair from becoming dry and brittle Slightly acidic nature helps prevent infection Oil glands plugged with dirt and oil result in blackheads or pimples. Hair • Consists of a root (which grows in a hollow tube called a (k) follicle) • A (l) hair shaft – Helps protect the body – Covers all body surfaces except the palms of the hands and the soles of the foot (m) Alopecia (baldness) • Genetically inherited • Males (and some females) • Permanent loss of hair of the scalp • • • • Nails Protect the fingers and toes from injury Made of (n) dead, keratinized epithelial cells Formed in the nail bed If lost, nails will regrow if the nail bed is not damaged Functions of Skin Protection –barrier against UV rays and infection, and helps prevent dehydration (p) Sensory perception – nerves help the body respond to pain, pressure, temperature, and touch sensations (q) Body temperature regulation 1. (o) 2. 3. • when blood vessels in the skin (r) dilate (get larger) – excess heat can escape • when blood vessels (s) constrict (get smaller) – heat is retained 4. 5. 6. 7. Storage – tissue temporarily stores fat, glucose, water, vitamins, and salts; adipose (fatty) tissue is a source of energy (u) Absorption – certain substances are absorbed through the skin, such as medicine and nicotine patches; medication patches are (v) transdermal (w) Excretion – eliminates salt, waste, excess water and heat through perspiration (x) Production – skin helps produce vitamin D using UV rays (t) Skin Pigmentation • Basic skin color is inherited – (y)Melanin – brownish-black pigment produced in the epidermis • Everyone has the same number of (z) melanocytes but genes determine the amount of melanin produced • Freckles are small concentrated areas of melanin – (aa)Albino – absence of color pigments in the skin • Skin has pinkish tint • Hair is pale yellow or white • Eyes lack pigment; are red; very sensitive to light Abnormal Pigmentation: • (bb)Erythema – reddish color that can be caused by burns or a congestion of blood in the vessels • (cc)Jaundice – yellow discoloration; indicates bile in the blood resulting from liver and gallbladder disease; also seen in diseases that involve destruction of RBC • (dd)Cyanosis – bluish discoloration caused by insufficient oxygen; associated with heart, lung, and circulatory diseases or disorders • (ee)Chronic poisoning – may cause gray or brown skin discoloration Primary Skin Lesions: Appear on previously healthy skin in response to disease or external irritation. • Macules – flat spots on the skin, such as freckles • Papules – firm, raised areas such as pimples and the eruptions seen in some stages of chickenpox and syphilis; up to 0.5cm in diameter • Vesicles – blisters, or fluid-filled sacs, such as those seen in chickenpox • Pustules – pusfilled sacs such as those seen in acne, or pimples • Bulla – fluid filled lesion greater than 2cm in diameter; caused by severe poison oak or ivy dermatitis • Comedo – plugged pilosebaceous duct, formed from sebum and keratin; blackhead (open comedo); whitehead (closed comedo) • Cyst – Semi-solid or fluid-filled encapsulated mass extending deep into the dermis; example is lacrimal cyst • Nodule – Firm, raised lesion; extending into dermal layer; deeper than a papule, 0.5 – 2cm in diameter; example intradermal nevus • Patch – Flat, pigmented, circumscribed area greater than 1cm in diameter • Plaque – Circumscribed, solid, elevated lesion greater than 1cm in diameter; elevation above skin surface occupies larger surface area in comparison with height • Wheals – itchy, elevated areas with an irregular shape; hives and insect bites are examples • Tumor – Elevated, solid lesion larger than 2cm in diameter, extending into dermal and subcutaneous layers Secondary Skin Lesions: Result from changes in the primary lesion, usually related to the disease process. • Crusts – areas of dried pus and blood, commonly called scabs • Ulcer – a deep loss of skin surface that may extend into the dermis; may cause periodic bleeding and the formation of scars • Atrophy – Thinning of skin surface at site of disorder; aging skin • Erosion – Circumscribed lesion involving loss of superficial epidermis; rug burn, abrasion • Excoriation – Linear scratched or abraded areas, often self-induced; for example, abraded (scratched) acne lesions, eczema • Fissure – Linear cracking of the skin, extending into the dermal layer; for example hand dermatitis (chapped skin) • Keloid – Thick, red, or dark firm scar formed by hyperplasia of fibrous tissue; more frequent in African Americans and Asians. • Lichenification – Thickened, prominent skin markings caused by constant rubbing; • Scale – Thin, dry flakes of shedding skin; for example psoriasis, dry skin • Scar – Fibrous tissue caused by trauma, deep inflammation, or surgical incision; red and raised (recent); pink and flat (6 weeks), or pale and depressed (old) Diseases and Abnormal Conditions • Skin cancer – most common type of cancer – 3 types: • Squamous cell carcinoma – affects the thin cells of the epithelium – spreads quickly • Melanoma – develops in the melanocytes – Most dangerous type of skin cancer • Basal cell carcinoma – cancer of the basal cells in the epidermis – slow growing • Acne – inflammation of the sebaceous glands • Athlete’s foot – contagious fungal infection that usually affects the feet • Eczema – noncontagious, inflammatory skin disorder caused by allergens or irritants • Psoriasis – chronic, noncontagious skin disease with periods of exacerbations (symptoms present) and remission (decrease or disappearance of symptoms) • Ringworm – highly contagious fungal infection of the skin or scalp • Impetigo – Highly contagious condition resulting from staphylococcus or streptococcal infection, and occurs most often in young children; starts as erythema but soon develops into vesicles and yellowish crusts. • Tinea – general name for many different types of mycoses (fungal infections); signs include erythema, scaling, and crusting. • Warts – caused by papilloma virus; type of benign neoplasm of the skin; some transform and become malignant; transmission generally occurs through direct contact with lesions on the skin of an infected person. • Boils – also called furuncles are most often local staphylococci infections of hair follicles characterized by large, inflamed pustules; A group of untreated boils may fuse into even larger pus filled lesions called carbuncles. • Scabies – contagious skin condition caused by the itch mite (Sarcoptes scabiei); transmitted by skin to skin contact; causes intense itching, and excoriation occurs as a result • Uticaria – (hives); characterized by raised, red lesions called wheals caused by leakage of fluid from the skin’s blood vessels; often associated with severe itching; hypersensitivity or allergic reactions, physical irritants, and systemic diseases are common causes. • Scleroderma – an autoimmune disease that affects the blood vessels and connective tissue of the skin; comes from the word sclera (hard) and derma (skin), means hard skin; begins with an area of mild inflammation that later develops into a patch of yellowish, hardened skin. • Decubitus ulcer – (pressure sore); the word decubitus means laying down; these lesions appear after blood flow to a local area of skin slows or is obstructed because of pressure on skin covering body prominences such as the heel; frequent changes in body position and soft support cushions help prevent these lesions from forming. Have different degrees in severity. Stage 1 • Nonblanchable erythema of the intact skin; discoloration of skin, warmth, or hardness may also be indicators. Stage 2 • Partial thickness skin loss involving epidermis and or dermis; the ulcer is superficial and presents clinically as an abrasion, blister, or shallow crater. Stage 3 • Full-thickness skin loss involving damage or necrosis of subcutaneous tissue that may extend down to, but not through, underlying fascia; presents as a deep crater with or without undermining of adjacent tissue. Stage 4 • Full-thickness skin loss with extensive destruction; tissue necrosis; or damage to muscle, bone, or supporting structures. • Burns – constitute one of the most serious and frequent problems that affect the skin. Typically you think of a burn as an injury caused by fire or by contact of the skin with a hot surface; however over exposure to ultraviolet light or contact of the skin with an electrical current or a harmful chemical such as an acid can also cause a burn. Classification of Burns • The classification system used to describe the severity of burns is based on the number of tissue layers involved; the most severe burns destroy not only the layers of the skin and subcutaneous tissue but underlying tissues as well. First Degree Burns • causes minor discomfort and some reddening of the skin; surface layers of thee epidermis may peel in 1-3 days; no blistering occurs, and actual tissue destrucction is minimal; Example is typical sunburn, Second Degree Burn • Involves the deep epidermal layers and always causes injury to the upper layers of the dermis; blisters, severe pain, generalized swelling, and fluid loss characterize this type of burn, scarring is common. • Characterized by Third complete destruction of the epidermis and dermis; tissue death extends below the primary skin layers into the subcutaneous tissue; often involve underlying muscle; insensitive to pain immediately afterwards, requires skin grafts for treatment Degree Burn • Characterized by Fourth Degree Burn complete destruction of the epidermis and dermis; tissue death extends below the primary skin layers into the subcutaneous tissue; often involve underlying muscle and bone; insensitive to pain immediately afterwards; Inhalation Burn • Caused by directly breathing in hot air/flame source; usually occur in the upper airways (trachea, esophagus, and mucous membranes) Nail Infection: Onychomycosis • Caused by yeast or fungus; most common form of nail infection; fungus grows on the growing portion of the nail and spreads proximally • Onychomycosis Wikipedia, the free encyclopedia Nail Ridging: • Fingernail Ridging: What Does It Indicate? Nail Clubbing • Clubbing of the Nails: eMedicine Dermatology Onycholysis • Onycholysis is a common nail disorder. It is the loosening or separation of a fingernail or toenail from its nail bed. It usually starts at the tip of the nail and progresses back. • Onycholysis: eMedicine Dermatology Physical Assessment Nails Assessment Techniques: • Inspection • Palpation Inspection • • • • • • • Color Consistency Symmetry Freedom from ridges and cracks Length Jagged or bitten edges Cleanliness Inspection • Assess the angle between the fingernail and the nail base, usually about 160 degrees; Palpation • Smoothness • Temperature • Capillary Refill Temperature • HOT • COLD Capillary Refill • The capillary nail refill test is a quick test performed on the nail beds to monitor and the amount of blood flow to tissue. • Capillary refill time, increased (Professional Guide to Signs & Symptoms (Fifth Edition)) WrongDiagnosis.com Skin Assessment Techniques: • Inspection • Palpation Skin • • • • Observe overall appearance Note any body odor Note disturbances in pigmentation Note skin color (Be aware that skin color varies from person to person depending on race and ethnic origin) • Note skin lesions Skin Lesion Assessment • Morphology – clinical description of the lesion; Note size, shape, configuration, color, elevation or depression, and texture. • Distribution – Pattern; includes extent of involvement and characteristic locations. • Location – related to total skin area; Note whether the pattern of lesions are local ( small area), regional (one large area), or general (over entire body). Skin Lesion Assessment • Configuration – arrangement of lesions in relation to each other; Skin Turgor • Assess skin elasticity by gently grasping and pulling up a fold of skin, releasing it, and observing how quickly it returns to normal shape. • Normal skin usually resumes its flat shape immediately • This technique also assesses skin mobility, which may be diminished in connective tissue disorders. Case Study: • Ms. Julie Roman, age 21, is a single Caucasian female law student. She has noted changes in her skin over the past 4 months. • Ms. Roman states that she has been under a lot of stress since she started law school 6 months ago, and noticed some faint redness and inflammation over her elbows and knees, with itching about 4 months ago. She stated that the redness progressed to large raised patches with scales that now involve the skin over her arms and back. She states that the lesions get better intermittently, but they always come back. Ms. Roman reports that the itching is an 8/10 and gets worse on humid days. • Ms. Roman states that she has tried numerous lotions and creams, even aloe vera, but it does not help, and it is embarrassing because her skin looks dirty and ugly. • On assessment Ms. Roman’s skin appears dry, oral mucosa is pink and moist. Large erythematous plaques with scales noted over her knees elbow, and back. Multiple scratch marks noted; some in a linear pattern with some thickened skin in areas caused by rubbing. • Ms. Roman’s nails are noted to have striations and their appears to be a fungal infection to the right index and ring fingers. Her skin elasticity is noted to be poor, and her hair is dry and brittle. Part I • Using the information provided, write a SOAPIE note documenting this patients condition. Part II Answer the following questions: 1. What is a probable diagnosis for the patient’s condition? 2. Review the Objective Data, what is the name for the fungal infection Ms. Roman suffers from? 3. What is the correct name for the linear scratch marks noted on the patients skin? Part II 4. What could be some possible causes of the Ms. Roman’s nails having the striations. What is another name for the striations? 5. What is this patient at risk for as a result of her current signs and symptoms? Part III Answer the following questions: 1. What effects do each of the following conditions have on the skin? -Anemia -Decreased oxygenation -Fever -Liver Disease Part III 2. What harmful effects on the skin, hair, and nails can the following behaviors produce? -Taking excessively long showers -Sunbathing or using a tanning booth -Exposing unprotected skin to cleaning solvents -Long-term braiding or corn-rowing of hair Pharmacology General Dermatologic Preparations Baths Oatmeal Bath • Click on the link below to get information regarding the use of this preparation. • Oatmeal Bath Soaps Antifungal Soap • Click on the link below to get information about Antifungal soap • What Is Antifungal Soap? | eHow.com Solutions and Lotions Calamine Lotion • Click on the link below to get information about calamine lotion • CALAMINE LOTION - TOPICAL side effects, medical uses, and drug interactions. Cleansers Hebiclens • Click on the link below to get information about hebiclens cleanser. • chlorhexidine-1 : Information on Uses, Dosage & Side Effects on Yahoo! Health.com Emollients Panthoderm • Click on the link below to get information about this emollient. • Panthoderm Cream Facts and Comparisons at Drugs.com Skin Protectants Benzoin Compound • Click on the link below to get information about this benzoin compound. • benzoin compound Wet Dressings & Soaks Aluminum Acetate Solution • Click on the link below to get information about this aluminum acetate topical solution. • Aluminum Acetate Topical Solution Rubs and Liniments Benzocaine • Click on the link below to get information about this benzocaine. • Benzocaine Topical Anti-Infectives Antibiotics • Neomycin Sulfate • BACITRACIN Antivirals • Acyclovir Antifungals • Lotrimin Corticosteroids • Corticosteroids • Eczema • Psoriasis Keratolytics • • • • • Keratolytic Medications Keratin dissolvers Salicylic acid Warts Plaque Acne Products • • • • Benzoyl-peroxide Clindamycin Erythromycin Tetracycline Burn Products • Silver-sulfadiazine Topical Ectoparasite Drugs • Kwell Drug Information, Professional Medical Terminology Instructions: • Look through the power point and identify the key terms that are important for you to know. • Write them down in your notebook. Medical Abbreviations • • • • • • • • • • dil – dilute dist – distilled dr – dram DC – discontinue DX – diagnosis elix. – elixer et – and ext. – external F – fahrenheit fl - fluid VIP of the Week Dr. Norman Orentreich Instructions: Research this person and write the following in your notebook. • Who is he? Describe him as a person. • What significance did he have to medicine, science, or health care? • How can you utilize his contribution in your profession? • How did his contribution affect the world?