I am So Confused! A Nursing Guide to Reading and
Interpreting Clinical Research
Sue Jasulaitis RNC, MS
Clinical Research Manager
Fertility Centers of Illinois
Learning Objectives
Review the importance of clinical research and develop
an understanding of basic research terminology.
Understand types of clinical research studies and
describe common approaches to conducting clinical
research.
Understand use of common statistical methods to
interpret clinical research results
Apply information gathered from research findings to
develop evidence-based clinical practices.
Nursing Leaders
They Love What They Do
They Understand What They Do
They Validate What They Do
They Communicate What They Do
Why Clinical Research?
Clinical trials are a vital tool for advancing medical
knowledge and patient care practices.
Enable nurses to direct resources to the strategies
and treatments that work best.
Provide the foundation for evidence-based medicine.
All health care professionals should be research-
literate to support evidence-based practice choices.
Nursing Experience
2008 Nursing study revealed:
64% of nurses read 1/more specialty journal
53% read 1/more general nursing journal
20% did not regularly read any specialty journal
None of the nurses reported reading a journal that related
directly to the stated research question.
Where did they obtain research material?
50% from the hospital library
34% did not know what literature-searching capabilities were
available to them.
(Leasure 2008)
Barriers to Clinical Research
Nursing Barriers to Research
Lack
of time to read research reports
Lack of access to research findings
Difficulty in understanding the jargon
Lack of knowledge to interpret research statistics
Lack of sufficient skills to evaluate research
Lack of knowledge to implement research into practice
Lack of adequate facilities for research implementation
(Richardson, 2002, NHLBI 2012)
Introduction to Research
A clinical trial is a research study involving
human subjects
The purpose of biomedical research is to:
Improve
Develop
Enhance
Conducted to allow safety and
efficacy data to be collected
for specific health interventions
What are Clinical Trials?
Clinical trials explore whether a medical strategy,
treatment, or device is safe and effective for humans.
These studies also may show which medical
therapies work best for specific populations.
A clinical trial may find that a new strategy,
treatment, or device:
Improves patient outcomes
Offers no benefit
Causes unexpected harm
(NHLBI, 2012)
Structure of Clinical Trials
Retrospective
Evaluates past treatment
Systematic Review
Overview of primary studies with similar
data sets
Cochrane Review (www.cochrane.org)
Meta-Analysis
Mathematical analysis of multiple studies
Cochrane Review (www.cochrane.org)
Prospective
Evaluate the effects of healthcare interventions
RTC (Randomized Controlled Trials)
Types of Clinical Trials
Prevention Trials
Screening Trials
Diagnostic Trials
Quality of Life Trials
Treatment Trials
Test experimental treatment, new drug combinations, or
new approaches to therapeutic interventions
Treatment Trials
Developed to determine safety and efficacy of
health interventions
Occurs in 5 phases, each addressing specific questions
Phase 0: Which drug is the best for clinical development?
Phase 1: Is the treatment safe?
Phase 2: Does the treatment work?
(Highleyman, 2005)
Treatment Trials (cont.)
Phase 3:
How does this treatment compare
to existing treatment?
Phase 4:
Are there other potential uses for this
treatment, and/or what are the long-term
adverse effects?
(Highleyman, 2005)
Treatment Trials: Study Design
Randomized
Subjects randomly assigned which study treatment
they will receive
Blind/Double Blind
Done to prevent study bias
Active Controlled (Non-inferiority)
Comparison of new therapy to standard of care
therapy
Placebo-controlled
Isolates the effect of the study treatment
(Highleyman, 2005)
Investigator-Initiated Trials
Developed to determine answers
to clinic-specific issues
Initiated by the clinic’s designated “investigator”
MD, Embryologist, Nurse, Psychologist, etc.
Protocol is designed and developed specifically to
answer the center’s question or concern regarding
their population.
Study Progression
Choose the correct population for the result desired
Select a homogenous population
Specific inclusion/exclusion criteria
Randomly (prospectively) assign the treatment
Randomized controlled trials (RTC’s)
Apply the intervention
Assess the results
Determine if the results are statistically significant
Apply the findings back to the target population
Determine if findings can be generalized
Components of Research Report
Abstract
Statement of the problem
Purpose of the study
Hypothesis
Literature review
Data collection/Statistical analysis
Study results/discussion
Conclusions
Implications for health care practitioners
Recommendations for future studies
References
(Summers, 1991)
Statistical Analysis Plan
Is the data analysis appropriate for the study?
Are the results Reliable and Valid?
Reliability
Results prove consistency over time,
representing the total patient population
Validity
Does the research measure what it is
intended to measure?
(Guilians, 2008)
How do We Measure Study Success?
Is the intervention causing the result?
Statistical Significance: P-value
Provides a single cut-off that for statistical significance.
Indicates the probability that the intervention is working
P-values of <0.05 or <0.01 are deemed statistically significant.
This means the likelihood is less than 5% (or 1%) that the observed
difference in the study treatment was due to chance.
ALSO CAN BE FALSELY AFFECTED BY
SMALL SAMPLE SIZES
(GUILIANS, 2008, HIGHLEYMAN, 2006)
How do We Measure Study Success?
Confidence Interval (CI)
Used as a measure to test the study hypothesis.
Commonly used in Meta Analysis
Used when dealing with a large data set, and provides a range to
determine where your result will fall.
How “confident” are you that the study result falls represents the
intervention?
Expressed in percentages: 95% confidence interval
Or 5% margin of error (5% chance the findings are wrong)
If the intervention produced “perfect results” the CI would be “0”. If
the results “cross 1” then the intervention produced no effect for the
population.
(Guilians, 2008, Highleyman, 2006)
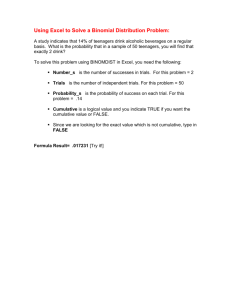
Example
Effect of probiotics on the risk of antibiotic associated diarrhoea.14.
Akobeng A K Arch Dis Child 2005;90:845-848
Copyright © BMJ Publishing Group Ltd & Royal College of Paediatrics and Child Health. All rights reserved.
Critiquing Research Papers
Is the research purpose clear?
Is the research design appropriate?
Is the recruitment strategy appropriate?
Was the data collected to addressed the hypothesis?
Are the results statistically significant?
Has the relationship between the researcher and
sponsors been adequately considered (bias)?
Is there a clear statement of the findings?
How valuable is the research?
(Lee, 2006)
Incorporating Research Into Clinical Practice
Assess the needs in your population.
Review literature for the experience of others.
Retrospectively review your patient outcomes
to determine if intervention are working.
Conduct a pilot study.
Compare your results to the literature.
Determine need for a change in policy an/or practice
standards.
This process allows nurses to better discuss new
findings/technology with patients.
New FCI Monthly Research Newsletter
Share Your Knowledge
Improve
Be
patient education
the resource!
Journal
club
Clinical
meetings (IVF meetings)
Scientific
Publish
conferences
your findings (professional journals)!
Add
research citations to standard operating
procedures
Develop
an REI Library
Barriers to Utilizing Research Findings
Lack of access to research findings
Uncertainty regarding the research results
A lack of confidence in evaluating the quality of the
research design
Difficulty in understanding the jargon
Have insufficient skills to evaluate research
(Richardson, 2002)
Strategies to Enhance Research Use
Identify Barriers
Organizational Issues
Lack of time to read research reports
Implement interventions to minimize barriers
Supportive Leadership
Collaboration between colleagues, staff and physicians
Presentation of research findings
Routine review of protocol outcomes
Provide continued education
Improve workload, increase resources
Establish a quality improvement plan
(Beyea, 2008; Richardson, 2002, Bostrom 2008)
Resources for Learning
KNOWLEDGE IS POWER
Continued Education is the KEY
In-services
CE Direct Courses
Free ASRM e-learn courses
ASRM certification course
Professional Symposia
Research Resources
PubMed access to MEDLINE. National Library of Medicine:
www.ncbi.nlm.nih.gov/entrez/query.fcgi?.
PatientINFORM. Free service providing medical journal access
and patient-friendly interpretation of studies in the fields of heart
disease, diabetes, and cancer: www.patientinform.org.
The Cochrane Library. Includes a comprehensive database of
systematic reviews of medical literature (abstracts and synopses
free; full text access requires subscription):
www3.interscience.wiley.com/cgi-bin/mrwhome/106568753/
home.
A Student's Guide to the Medical Literature, University of
Colorado Health Sciences Center. Includes links to several medical
literature databases, evidence-based medicine Web sites, and
treatment guideline repositories, as well as MEDLINE search tips
and a glossary: http://denison.uchsc.edu/SG/main.html.
(Highleyman, 2006)
Research Resources
On-line resources:
Center for Disease Control (CDC)
Medical societies (ASRM, ESHRE,CFS, etc.)
Pharmaceutical company websites
Clinical trials databases
Clinicaltrials.gov
PhRMA repository of clinical trial results:
www.clinicalstudyresults.org.
Summary
When nurses understand research, they are better able to
apply research.
Clinical trials determine risks and benefits of the intervention,
but the results can only be generalized to the target
population.
The results cannot predict how well a given treatment will
work for a specific person.
Practitioners must still tailor treatment options to meet the
needs of individual patient based on evaluation of the
risk/benefit provided, as well as intuition and clinical
experience.
In the end, the practice of medicine remains an art as well as a
science.
(Highleyman, 2006)
Nursing Leaders
Be a Clinical Leader
Love what you do
Understand and validate
what you do
Communicate what you do
References
Richardson, J (2002) Helping nurses to interpret and evaluate
research. Nursing Times Vol. 98 (5) p. 38
Bostrom, A., Kajermo, K,. Nordstrom, G,. Walline, L. (2008). Barriers
to Research Utilization and Research Use Among Registered Nurses
Working in the Care of Older People. Does the BARRIERS Scale
Discriminate between Research Users and Non-Research Users on
Perceptions of Barriers? Implement Science. 3:24.
NHLBI (2012, August 3): “What are Clinical Trials?”. Retrieved from
http://www.nhlbi.nih.gov/health/health-topics/topics/clinicaltrials/
NHLBI (2012, August 3) “Why are Clinical Trials Important?”
Retrieved from http://www.nhlbi.nih.gov/health/healthtopics/topics/clinicaltrials/important .html
Highleyman, L. (2006) A Guide to Clinical Trials. BETA .Winter 18(2),
41-7.
References (c0nt.)
Summers, S. (1991) Defining Components of the Research Process Needed
to Conduct and Critique Studies. J Post Anesth Nurs.
Feb; 6(1):50-5.
Higleyman (2005) Understanding Clinical Studies. BETA . Summer 17(4),
42-9.
Giuliano, P., Polanowicz, M. (2008). Interpretation and Use of Statistics in
Nursing Research. AACN Advanced Critical Care 19 (2), p. 211-222.
Lee, P. (2006). Understanding and Critiquing Qualitative Research
Papers. Nursing Times. 102 (29), p 30.
Beyea, S., Nicoll, L. (2008). Barriers to and Facilitators of Research
Utilization in Peri-operative Nursing Practice. AORN Journal 65(4), p.
830-831.
Leasure, A., Stirlen, J., Thompson, C. (2008) Barriers and Facilitators to
the Use of Evidence-Based Best Practices. Dimensions of Critical Care 27
(2), pp. 74-82.