in brain & spinal cord
advertisement

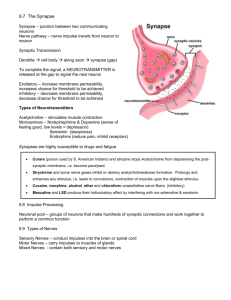
The Nervous System NS and Endocrine System •Transmit info from 1 part of body to another Communication—Integration--Control Nervous System •Rapidly & short duration via nerve impulses Endocrine System •Slowly via hormones (chemicals) secreted by ductless glands into blood stream circulated from glands to other parts of the body (target cells) Homeostasis: Balanced & Controlled internal environment of body essential to fx of all body systems relies on physiological control & integration NS: Monitors & Responds to In/External stimuli Nervous System CNS PNS brain & spinal cord nerves & associated cells not part of CNS Sensory Nerves Motor Nerves Respond to stimuli from Env Somatic NS To skeletal muscles/voluntary Sensory Receptors w/in sense organs Autonomic NS (Eyes, Ears, Taste, Touch, Smell) To cardiac & smooth muscles, glands, involuntary parasympathetic sympathetic Fight/Flight gas ↑ brake ↓ Antagonistic Coverings & Fluid Spaces of Brain & Spinal Cord Meninges: Tough, fluid containing membrane surrounded by bone (skull & vertebrae) 3 Layers of Spinal Meninges Dura Mater (tough outer layer, lines vertebral canal) Pia Mater ( innermost layer covering spinal cord) Arachnoid Layer ( middle layer between Dura & Pia) cob web like w/ fluid (CSF) filling spaces Meninges (protective) extend up & around enclosing brain Fluid fills Arachnoid spaces of brain meninges & spinal cord Cerebral Ventricles: Fluid filled spaces w/in brain 2 lateral ventricles deep w/in brain w/in Lt & Rt cerebrum (lgst part of brain conscious, voluntary, mental processes, emotions) CSF: cerebral spinal fluid forms continuously from fluid filtering out of blood network of brain capillaries (choroid plexus) & into ventricles From lateral ventricles CSF 3rd ventricle & flows ↓ aqueduct of Sylvius 4th ventricle subarachnoid spaces subarachnoid spaces of meninges that surround spinal cord blood via veins in the brain ***CSF forms continuously from blood, circulates & is reabsorbed into blood again **Pressure on Aqueduct of Sylvius (Ex. brain tumor) blocks return path of CSF blood CSF accumulates in ventricles or meninges. Hydrocephalus water on the brain Treatment catheter to drain fluid back to body **** **** **** 3 Types of Neurons Sensory Neurons (Afferent): Carry impulses from sense organs to spinal cord/brain (CNS) Dendrites can be very long Motor Neurons (Efferent): Carry impulses from CNS (brain/sc) (Effecter) to muscles & glands Interneurons (Central or Connecting): Connect sensory & moto neurons in spinal cord Lie w/in gray matter of CNS Cells of the Nervous System Neurons & Neuroglia Basic Neuron Structure sensory, motor, & Soma Many dendrites Cell body interneurons (between sensory & motor Impulse received by dendrites neurons in spinal column) Axon terminals vesicles w/ neurotransmitters Myelinated axon carries impulse from cell body axon terminals Saltatory conduction **vertebrates Mostly outside CNS 80% lipid 20% protein Insulated sheath White Matter Indentations between Schwann cells Axons in brain & sc have no neurilemma no regeneration but those in nerves do regeneration Extend thru axon from cell body Saltatory Conduction: carries impulse node to node (vertebrates) 200 m/s vs few mm/s in unmyelinated (gray matter) Neuroglias (connective tissue) Special connecting & supporting tissues of brain & spinal cord don’t transmit impulses Glia (glue): hold neurons together & protects them Glioma: common type of brain tumor develops from neuroglia cells 3 Types of Neuroglia Astrocytes: Microglia: usually stationary can move & become phagocytic (scavengers) Oligodendroglia: hold nerve fibers together & produce fatty myelin sheath that covers nerve fibers (axons) in brain & spinal cord (not Schwann Cells outside CNS) Myelinated fibers (high fat white matter) Nonmyelinated (gray matter) Myelin Disorder Diseases associated with Oligodendroglia Multiple Sclerosis: Most common 10 of CNS Characterized by myelin loss/ destruction w/ oligodendroglial cell injury/death demyelination of white matter of CNS nerve conduction impaired weakness, in-coordination, visual impairment, speech disturbances Afflicts more women between 20-40 MS ??? Related to autoimmunity & viral type infections Prolonged disease w/ relapses & remissions White Matter in brain & Spinal cord made up of Tracts Tract: bundle of myelinated axons White Matter outside brain & spinal cord = nerves Nerves bundles of myelinated axons single group of nerve fibers surrounded by connective tissue sheath Nerve Trunk group of bundled nerves Nerve prs 8 12 7 cervical vertebrae 12 thoracic vertebrae 5 5 lumbar vertebrae 5 1 Fused vertebrae coccyx Reflex Arcs impulse conduction in 1 Direction 2 neuron arc (sensory motor) 3 neuron arc (sensory interneuron motor neuron) Interneurons w/in gray matter (H-zone) Synapse: (microscopic space between neurons that neurotransmitters released from axon terminals diffuse across) Sensory neuron receptors w/ dendrites pick up stimulus impulse created cell body axon of sensory neuron Synapse interneuron (dendrite cell body axon) synapse motor neuron (dendrite cell body axon) neuromuscular junction Posterior root ganglion Anterior root spinal nerve Patellar Tendon Knee Jerk Reflex Infant Reflexes Rooting Reflex: stroke cheek/ turns head towards touch Gripping Reflex: grasp anything placed in palm Toe Curling Reflex: Inner sole of foot stroked toes curl Outer sole of foot stroked toes spread Stepping Reflex: Held up w/ feet on surface walk/march Sucking Reflex: when something touches roof of mouth Startle/Moro Reflex: sudden sound/mvmt throw arms & legs out & head back then pull limbs back into body Galant Reflex: stroke middle or lower back body curves towards side stroked Tonic Neck Reflex: place on stomach whichever side head is facing limbs on that side straighten, opposite side curl The Nerve Impulse Initiated by a stimulus (pressure, temp, chemical changes, etc) Resting Neuron Outisde +++ Inside (Resting Potential) --- Na+ ions pumped out and K+ ions pumped in Na/K pump run by ATP Active Transport More K+ ions leak out than Na+ ions leak in - - - charge inside c.m +++ charge outside (Also other ions present Ex. Cl-) C.M has gates/channels that allow ions to pass thru normally closed Steps of an Action Potential (Nerve Impulse) Neuron stimulated nerve impulse generated Na+ gates open & flow inside C.M. Inside becomes more + than outside Action Potential Nerve Impulse Depolarization As impulse passes, K+ gates open and K+ ions flow out Inside becomes – and outside + again (Reploarization) Threshold: minimal level of stimulus required to create impulse All or none Impulse moves in 1 direction b/c Na+ gates close after impulse & can’t be reopened for short time (Refractory Period) Link to Action Potential Animation w/ Saltatory Conduction http://www.blackwellpublishing.com/matthews/actionp.html Resting Potential Action Potential Na+ rush in Depolarization Re-polarization – Action Potential – Resting Potential Re-polarization Refractory Period Resting Potential Action Potential reaches Axon Terminal Vesicles w/ neurotransmitters rupture chemicals released diffuse across synaptic cleft (assist, stimulate or inhibit postsynaptic neurons) Neurotransmitters: chemicals used by neuron to transmit impulse across synapse to another neuron or cell (Ex. muscle) *neuromuscular junction • Impulse arrives at axon terminal •Vesicles release neurotransmitters into synaptic cleft/gap •Neurotransmitters diffuse across synapse & attach to receptors on next cell •Stimulus causes rush of Na+ to rush into cell •If threshold met/exceeded new impulse or Rx occurs Ex. muscle contraction Neurotransmitters quickly: broken ↓ by enzymes taken up/recycled by axon terminal diffuse away Certain Illnesses associated w/ abnormal levels of Neurotransmitters Depression: ↓ serotonin & norepinephrine (Exercise releases these) Schizophrenia: associated w/ ↑ levels of dopamine Parkinson’s Disease: progressive NS disease most often after age of 50, associated with the destruction of brain cells that produce dopamine, characterized by muscular tremor, slowing of movement, partial facial paralysis, peculiarity of gait and posture. Endorphins & Enkephalins: Inhibit conduction of pain impulses How do abnormal levels of neurotransmitters affect Fx of NS? Either ↑ or ↓ transmission of nerve impulse Nerve Gas: Class of Lethal Weapons Fx: Inactivate certain enzymes of nerve transmission Normal: neurotransmitters diffuse away, recycled, inactivated Neurotransmitter Acetylcholine is inactivated by cholinesterase enzymes that deactivate acetylcholine quickly efficient, precise synaptic transmission Nerve Gas: binds to & inhibits cholinesterase so acetylcholine remains in synapse continuous stimulation of nerves Uncontrollable convulsions, muscular contractions, death Synaptic Integration: Provides checks & balances in NS At each neuron, Excitatory & Inhibitory receptors compete for membrane control Signals can totally/partially cancel each other out or augment each other’s effect Net outcomes depend on strength, direction & location of each signal. Clostridium tetani Produces toxin that interferes w/ Inhibitory Receptors & Motor Neurons in CNS (brain/sc) Lock jaw unbalanced excitation of muscle cells constant (tetanic) contraction spastic paralysis death Structure of the Spinal Cord • Avg adult spinal cord 17-18” long • Lies inside spinal column in spinal cavity • Extends from occipital bone to 1st lumbar vertebrae • Hands on hips L4 • Spinal meninges extend beyond spinal cord almost to end of spinal column • Allows for spinal tap (lumbar puncture) to extract CSF (test) insert needle just above L4 Spinal Cord • H- shaped gray matter ( dendrites & cell bodies of neurons) • White matter outer part (bundles of myelinated nerve fibers) spinal tracts • Ascending tracts conduct impulses ↑ cord to brain Ex. sensory fx (pain, touch pressure, etc) • Descending tracts conduct impulses ↓ cord from brain Ex. vol. mvmts, skeletal muscle activity Spinal Cord fxs as Switchboard Carries impulses to & from brain To brain via ascending tracts From brain via motor tracts Contains centers for Reflex Arcs Interneurons switch/transfer incoming sensory impulses to outgoing motor impulses Spinal Cord Reflex Arc 2 kinds withdrawal reflex (Ex. from hot/sharp surface) knee jerk reflex Injury cuts spinal cord across impulses can’t pass produces Loss of sensation Anesthesia Loss of ability to move paralysis Spinal Nerves (31 prs) 8 cervical (7 cervial vertebrae) 12 thoracic (12 thoracic vertebrae) 5 lumbar 5 (5 lumbar vertebrae) Sacrospinal (fused vertebrae) 1 coccygeal (coccyx) Conduct impulses between spinal cord & areas not supplied by 12 cranial nerves Contain both sensory & motor fibers sensation mvmt Nerve prs 8 12 7 cervical vertebrae 12 thoracic vertebrae 5 5 lumbar vertebrae 5 1 Fused vertebrae coccyx Dermatome: skin surface area supplied by single nerve Herpes Zoster/Shingles: viral infection of single dermatome caused by varicella zoster virus of chicken pox Virus travel thru cutaneous nerve & remains dormant in dorsal root ganglion long after chicken pox infection ↓ Immune Response (Ex. elderly, stress, radiation, immunosuppresive drugs virus may reactivate Virus travels over sensory nerve to skin of single dermatome painful eruption vesicles, crust & clear 2-3wks PNS Outside CNS Nerves & associated cells not part of CNS (brain & s.c) Consists of: cranial nerves that pass thru skull stimulate head & neck Spinal nerves: 31 prs Ganglia: (nerve cell bodies) Sensory Division of PNS: transmits impulses from sense organs CNS Motor Division of PNS: transmits impulses from CNS muscles/glands (Effectors) Somatic NS voluntary Autonomic NS Involuntary Skeletal muscle contraction Ex. smooth muscles, digestion pupils reflex Some also use reflex arc Sympathetic Parasympathetic ↑ Effect (gas) ↓Effect (brake) Running: Sympathetic NS ↑ heart rate, blood flow to skeletal muscles, stimulates sweat & adrenal glands Parasympathetic NS ↓ smooth muscle contractions in digestive system Stop Running: Parasympathetic NS ↓ heart rate & blood flow to skeletal muscles Sympathetic NS ↑ contractions of smooth muscles in digestive system Important Fx Maintaining Homeostasis Divisions of the Brain Billions of Neurons 1.4kg Must have continuous supply of O2 Part of brain that is damaged determines effects Wavy bumps/folds: gyri (gyrus) Shallow grooves: sulci (sulcus) Folds/Grooves ↑S.A for more neurons (S&F) Gyri: folds Sulci: grooves Cerebrum: Largest part of brain Voluntary, Conscious activities Intelligence, Learning, Judgment Divided into LT & RT hemispheres by deep longitudinal fissure Hemispheres connected by corpus callosum Each hemisphere divided into 4 lobes named after skull bones Frontal (vol muscle mvmt) Parietal (behind frontal) Temporal (sides) Occipital (back) Parkinson’s disease of basal ganglia shaking/tremors Myelinated fibers join LT & RT Hemispheres Fx produces automatic mvmts & posture Each ½ of Cerebrum deals w/ opposite side of body • Sensations from LT body Rt hemisphere • Sensations from RT body Lt hemisphere Commands to move muscles also opposite • LT hemisphere controls RT side of body • RT hemisphere controls LT side of body Studies suggest RT hemisphere associated w/ artistic/creative Lt hemisphere associated w/ analytical/mathematical 2 Layers to Cerebrum Outer Cerebral Cortex gray matter (densely pkd cell bodies & unmyelinated axons) Processes info from sense organs Controls body mvmts Inner Cerebral Medulla white matter (bundles of myelinated axons) Connects Cerebral Cortex & Brain Stem 3 Regions of Cerebral Cortex (Outer layer of Cerebrum)) Spinal Cord damage disconnects ascending & descending tracts Motor Centers: Instructions for motor response coordinated Motor Cortex connects to Descending Motor Tracts Stimulation of different point on Motor Cortex muscles in different parts of body to contract *** Lg area of motor cortex devoted to muscles that control tongue & thumb mvmts Reflects amount of control req’d for hand mvmts & speech Regions of Motor Cortex cont’d 10 Receiving Centers: Receive sensory input from PNS (Sensory) Somatic Sensory Cortex (behind motor cortex) is 10 receiving center for sensory input from skin & joints via Ascending Tracts Association Centers: Separate from Motor & 10 Rec. Centers but connected to motor & sensory thru neural pathways Brain Studies 1940’s Wilder Penfield surgically exposed Cerebral Cortex Used weak electrical stimulation on patients still awake Brain pkd w/ neurons but NO pain receptors!!!! Stimulated part of Cerebral Cortex at a time & patients described sensations Motor Cortex = areas where stimulation muscle contraction Sensory Cortex = areas where stimulation taste, touch, sound Areas where stimulation memories = physical location of memories Sensory control Sensory Neurons (Affecter) brings message to spinal cord Neurons in spinal cord carry impulses to Thalamus via Ascending Tracts Thalamus: switching station relays impulses to Sensory Cortex (in Cerebrum) for action Motor Cortex sends message ↓ spinal column via descending tracts to synapse w/ Motor Neuron (Effecter) ??? Cases where parts of spinal cord destroyed & still sensation at different parts of body, despite no connections to carry impulse to cerebral cortex!!! Brain Studies Hebel & Wiesel (Harvard) studied visual cortex in kittens Thought all nerve connection in brain genetically determined Kittens: Kept 1 eye closed since birth Nerve connection failed to develop!!! Other eye nerve connections developed normally Determined: Pattern of connections depends on kinds of visua stimulation experienced in early development after birth Concluded: Abnormal nerve development env. not genetic influence Env & sensory input develops neural pathways (plasticity) *Babies & visual stimuli ↑ visual stimuli ↑ Nerve Connections Cerebellum: 2nd largest part of brain (outer gray, inner mostly white) Back of skull Commands to move come from Cerebral Cortex but Cerebellum coordinates & balances actions of muscles smooth, efficient, graceful mvmt Involuntary Damaged Cerebellum muscle weakness ↓ Coordination Simple tasks (walk, run) difficult Train Cerebellum to coordinate muscle use Practice helps develop connections to Cerebellum make task easier (but not under conscious control) ***Occupational Therapy Importance Brain Stem Midbrain Pons Medulla Oblongata * * ** b r a i n s t e m ** ** * * Brain Stem Foramen Magnum opening in occipital bone for spinal cord to pass thru Medulla: Extension of spinal cord just inside cranial cavity Gray & White matter intermingle Reticular Formation *Remember in spinal cord inner (H) = gray outer = white Pons: (middle/bridge) between Medulla & Midbrain Midbrain: above Pons Brain Stem is 2 way conduction path Sensory fibers impulses spinal cord brain Motor fibers impulses brain spinal cord Many Vital Reflex Centers lie in Medulla of Brainstem Cardiac, Respiratory, Vasomotor Centers Impulses that control heartbeat respirations blood vessel diameter Diencephalon: Between midbrain & cerebrum Contains Hypothalamus & Thalamus (below thalamus) Hypothalamus: Contains Posterior pituitary gland Control over Paraventricular & Supraotic Nuceli All internal organs (2 clusters of neuron cell bodies) Appetites Make hormones Posterior Pituitary Body Temp Gland stores/ secretes into blood. Hunger Thirst Fatigue Ex. ADH affects urine volume to maintain body’s H2O balance *** Coordinates Nervous System & Endocrine System Some Neurons in hypothalamus Fx as Endocrine (ductless) Glands Axons secrete Releasing Hormones into blood RH’s control release of Anterior Pituitary Hormones that influence hormone secretion by other Endocrine Glands Thalamus (above hypothalamus) • Helps produce sensations (relays impulses to cerebral cortex from sense organs, (except smell) • Associates sensations w/ emotions • Arousal/alerting mechanism Brain Waves Brian neurons capable of Action Potential (electrical activity) Voltage sensitive electrodes on scalp record weak electrical current EEG: Electroencephalogram Records electrical activity on scalp Measures average activity of thousands of neurons general idea of brain activity Sleep: Activity of Cerebral Cortex ↓ to lowest level unconsciousness deep unresponsive to light sleep RAS (Reticular Activating System) Network of neurons in Medulla Oblongata (brain stem) helps control consciousness Level of RAS ↓ sleep begins Special group of neurons in brainstem activate light sleep During deep sleep ↓ in heart rate, BP, respiration rate, energy use During REM (Rapid Eye Mvmt) sleep dreaming occurs Memory Short Term: Not permanent Stored as pattern of nerve impulses in Cerebral Cortex Vanishes w/in few days unless interesting or effort to remember Long Term: More permanent Some last lifetime May require effort to recall Can become part of person’s consciousness Some patients w/ severe brain injuries keep long term memory (even w/ Cerebral Cortex damage) Suggests long term memory stored in structure of brain itself