02.09.13 DDES CCG Governing Body Meeting in Common
advertisement

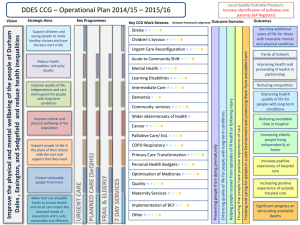
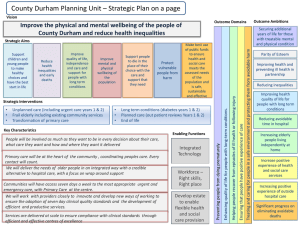
A Meeting in Common of the NHS Hartlepool & Stockton-on-Tees Clinical Commissioning Group and NHS Durham Dales, Easington and Sedgefield Clinical Commissioning Group Governing Bodies Monday 2nd September 2013, 1:30-3:30 pm Hartlepool College of Further Education, Conference Centre CONFIRMED MINUTES Present Dr Boleslaw Posmyk (PB) Neil Atkinson (NA) Brian Dinsdale (BD) Ken Lupton (KL) Claire Young (CY) Mary Bewley (MB) Roger French (RF) Jean Fruend (JF) Dr Charles Stanley (CS) Graham Niven (GN) Dr Bhadrash Contractor (BC) Hilary Thompson (HT) Dr Nick Timlin (NT) Dr Mike Smith (MS) Ali Wilson (AW) Annie Dolphin (AD) Mike Taylor (MT) Joseph Chandy (JC) Gillian Findley (GF) Peter Carr (PC) David Taylor-Gooby (DTG) Keith Tallintire (KT) Deborah Perry (DP) Paul Garvin (PG) Alan Foster (AF) Julie Gillon (JG) David Emerton (DE) Governing Body Chair, Hartlepool & Stockton-on-Tees Clinical Commissioning Group (HaST CCG) Deputy Director of Finance and Information, North Tees and Hartlepool NHS Foundation Trust (NTHFT) Deputy Chair, Non-Executive Director, NTHFT Non-Executive Director, NTHFT Head of Communications, NTHFT Head of Communications and Engagement, North of England Commissioning Support (NECS) Director of Finance and Resources, North East Ambulance Service (NEAS) Executive Nurse, HaST CCG Secondary Care Consultant, HaST CCG Chief Finance Officer, HaST CCG GP Member, HaST CCG Lay Member for Public and Patient Involvement, HaST CCG GP Member, HaST CCG GP Hartlepool Locality Lead, HaST CCG Chief Officer, HaST CCG Governing Body Chair, Durham Dales, Easington and Sedgefield Clinical Commissioning Group (DDES CCG) Chief Finance and Operating Officer, DDES CCG Director of Performance and Information, DDES CCG Director of Nursing, DDES CCG Secondary Care Clinician, DDES CCG Lay Member for Public and Patient Engagement, DDES CCG Lay Member Audit and Assurance, DDES CCG Corporate Services Administrator Coordinator, Minute-taker in attendance, DDES CCG Executive Chairman, NTHFT Chief Executive, NTHFT Deputy Chief Executive and Chief Operating Officer, NTHFT Medical Director, NTHFT 1 Jean McLeod (JM) Narayaran Suresh (NS) Claire Curran (CC) Heidi Holliday (HH) Kerry McLean (KM) Debbie Lamming (DL) ITEM 1 Clinical Director of Medicine, NTHFT Clinical Director of Anaesthetics, NTHFT Director of Human Resources and Education and Company Secretary NTHFT Private Office Manager, NTHFT Minute-taker in attendance, Administration Assistant, NECS Minute-taker in attendance, Administration Assistant, NECS SUBJECT Welcome and Introductions from Joint Chairs of the Meeting ACTION PB welcome everyone to the meeting in common of the Hartlepool and Stockton-on-Tees Clinical Commissioning Group (HaST CCG) and the Durham Dales, Easington and Sedgefield Clinical Commissioning Group (DDES CCG) Governing Bodies relating to the proposal to centralise the emergency medical and critical care services at the University Hospital of North Tees. PB explained that the meeting was being held in public but was not a public meeting where questions could be taken directly from the public. Members of the public were present to observe and to ensure involvement in the process. PB stated that the Governing Body members of both CCGs would make themselves available for half an hour at the end of the meeting to discuss matters with attendees and take any questions. 2 Declarations of Interest There were no declarations of interest made. 3 Apologies for absence Dr Stewart Findlay, Chief Clinical Officer, DDES CCG Dr Dinah Roy, Director of Clinical Quality and Primary Care Development, DDES CCG Dr Helen Moore, Clinical Locality Lead, Sedgefield Locality, DDES CCG Dr Stephen Muscat, Clinical Locality Lead, Easington Locality, DDES CCG Dr Satinder Sanghera, Clinical Locality Lead, Durham Dales Locality, DDES CCG Dr John McGuire, Sessional GP, DDES CCG Dr Paul Williams, GP Stockton Locality Lead, HaST CCG Steve Smith, Lay Member for Governance and Audit, HaST CCG 4 Proposal to centralise emergency medical and critical care services at the University Hospital of North Tees PB explained that the two CCGs needed to consider the proposals put to them by the Acute Trust regarding the changes to NT&H hospitals. The meeting would be chaired by both CCG chairs with the first part being received in the form of a presentation from NTHFT on the clinical case for change and the consultation process. 2 The second part of the meeting would be the opportunity for the Governing Body members of both CCG to put questions to the presenters. DDES CCG would then run through their decision-making process followed by HaST CCG, with the public in attendance to witness this. Following the separate Governing Body decision-making process next steps would then be discussed. AW checked that everyone present had seen and read the consultation documents, which was confirmed. All papers had been uploaded to both CCG websites. The key reports had taken into account all legal requirements of the Secretary of State. AW set the scene by referring to the changing needs of patients and how medical care is changing now and in the future. CCGs are more aware than ever of an ageing population, far more complicated disease patterns, the increasingly complex and multiple health needs of patients. Higher standards, availability of medication, providing care closer to home and the best possible discharge care make it increasingly difficult for NTHFT to provide services and the highest standards across the two hospital sites. As an organisation NTHFT has always been very proud of achieving the highest clinical standards with the best possible care for patients and are driven by very specific clinical guidelines which encourage cooperative working. The Trust strives to maintain these standards and will continue to do so in the future. Changes were needed because of the difficulty of sustaining two units; this issue was discussed in detail within the Trust and brought to the attention of commissioners who were appraised of the situation. NS explained that historically intensive care was always viewed as a subspeciality of anaesthetics but that the General Medical Council (GMC) last year recognised it as more than this. It is now more difficult to achieve national body standards and it has proven difficult to recruit staff to such a small unit as existing staff feel unsupported and concerned regarding the possibility of clinical errors, maintaining clinical qualifications and, therefore, standards of care. The main aim of NTHFT is to make the service as safe as possible, hence the rationale behind the proposed changes. The National Clinical Advisory Team (NCAT) spent time looking at the services provided and recognised a potential clinical risk and differences in equality of services offered to North Tees and Hartlepool patients (for example patients experiencing medical complications at Hartlepool need to be moved to another site and those at North Tees only need to be move to another floor of the same building). Options for reducing risks were considered for both sites (see Appendix A) by NCAT and NTHFT; for example increased staffing levels, increased working hours, changes to patient pathways. The possibility of running 3 the two units in parallel was considered but this was advised against. NCAT advised NTHFT that they were correct in recognising and addressing clinical safety concerns and that the service was unsustainable. Redesign of the service by centralising intensive care at North Tees, with medical care following, was viewed as the safest and most viable option available. Final assessment from NCAT advised that changes should be made as soon as it was safe to do so and as soon as possible. NTHFT concluded that to maintain the standards and highest quality of care for patients already established in the catchment area centralisation of critical care and medicine at the North Tees site could be the only recommended option. NTHFT has acknowledged that the recommendations need to be followed through and that if the health service is to be fit for the future centralisation is required but also that the consultation process has brought concerns from the public around several areas. The Trust is committed to providing care closer to home of the highest standard and will do their utmost to support members of the public as a result of the proposed changes. A steering group made up of representatives from Healthwatch, CCGs, Commissioning Support and the Trust was set up to work on the consultation process and key messages to the public were highlighted in their consultation report, as below. AW reminded attendees that 97% of healthcare contacts currently being dealt with in Hartlepool will continue and that the proposals would affect approximately 30 patients per day from Easington and Hartlepool. No change to the point of access is planned and patients will still need to contact their GP, 111 or 999 as previously. Extra beds will be made available at North Tees and the staff from the emergency medical ward and critical care staff from Hartlepool will move to North Tees. The majority of health services for patients will continue to be delivered through GP practices and other community services as usual. MB stated that to ensure requirements of the four tests (see slide content) had been met and to strengthen patient and public involvement the consultation process was underpinned by the steering group at all points. As part of the process as wide a range as possible of communication access points was provided; face to face meetings, internet, email, telephone, and independently evaluated questionnaire, websites, a summary leaflet to GP practices and delivered door to door, local media and networks, drop in sessions and market place events, community meetings, events for governors and the public. All were good opportunities for people to talk and to feed back about the process and all were documented and recorded. Output of the consultation resulted largely in negative responses but people felt very passionate and did not want a reduction in hospital services. However most agreed, once an understanding of the clinical 4 argument was reached, that the changes are the safest and most sensible course of action. One of the main issues identified was transport and the lack of information available to patients. The consultation process was used to consider all transport-related issues and CCGs were reminded that in commissioning services they are expected to consider the transport needs of patients. An exercise was undertaken as part of the process which looked at, amongst other things, travelling times between Hartlepool and North Tees and mitigation plans are being considered for the issues identified; additional shuttle services, discount travel costs, collaborative work between the CCGs and the Trust, application for additional car parking at North Tees, volunteer driver scheme improvements, park and ride systems, car sharing and shuttle transport for staff including shift pattern studies and coordination. It was highlighted that the patient transport service provided by NEAS was sometimes untimely, often resulting in missed appointments and long waits for the elderly. These issues are being considered to ensure the service is more accessible and practical. The Trust and CCGs are working with NEAS to ensure transport needs are met as identified by the public. HaST CCG recognise that providing services closer to home is a priority for patients and is working collaboratively with DDES colleagues all the time to achieve this. GPs in both CCG areas, although disappointed about the proposals, have been involved in the consultation from the start and agree that from a clinical safety viewpoint the planned changes are the safest option for their patients. It was reiterated that NCAT feel very strongly that all clinical evidence points to the move as the right thing to do. The Trust and the CCGs have an ongoing quality assurance process in place to assure, and be assured, that all quality and safety concerns are met. Patient Choice exists for planned care (elective) already but not unplanned care (non-elective) and this will not change except for a small number of surgical patients. Other statutory requirements have all been met as part of the process (Health and Social Care Act and equality assessments). The main issues raised as part of the process: High quality is paramount Patient safety cannot be compromised Understanding concerns regarding loss of services Transport Close working with partners 5 Need to provide better public information and communication How we will address these: Each GB was asked to consider the clinical case for change and all feedback from the public consultation and agree next steps today. NCAT had pointed out in the report that as commissioners CCGs had to assure themselves of the provision and safety of services at North Tees and those left behind at Hartlepool. JF confirmed that the Clinical Quality Review Group meets regularly and has received assurance from all parties that clinical quality concerns have been met using a very robust consultation process. 5 Opportunity for the Governing Body members to raise questions and issues Q1 If the proposals did not go ahead, how will current services be maintained? A1 Current services could be maintained; however, whether these can be sustained is unclear. Q2 JF asked what the issues were regarding recruitment to the critical care unit. A2 NS responded that although there were no real issues with recruiting to one service, if it was run over two sites the Trust would have to consider recruiting a further 10 consultant physicians and double the junior doctor cover for all shifts including Out of Hours. Recruitment to a small intensive care unit is deeply unattractive as jobs have become more specialist and therefore more competitive. It is now more challenging to work towards the required quality of care standards and, at the same time, retain high quality personnel across two sites. Q3 PC asked whether, in the long term, there would be issues for consultants working across two sites with regard to continuity of care, ie who looks after patients once they have been moved? What are the transfer arrangements from one site to the other? A3 There is disruption to continuity of care at the moment as when patients are moved the “parent team” changes, which can be difficult for families concerned. In the new model patients would be discharged to the rehabilitation unit and cared for by the elderly care team, who are effectively the gatekeepers for the unit. This will apply to any patients with limited continuing medical needs but with the need for rehab, occupational therapy and input from other services, with a view to their planned care being picked up by the Care Closer To Home services (using a step down / sub-acute approach, designed to be part of the “looked after in your own home” teams). It is vitally important that continuity is reassured, in effect improving the service for these patients with the changes. This care is provided by colleagues working under a multidisciplinary service. This new model is a completely different approach which depends on the 6 needs of the patient, being built around them and not around the service team. Q4 DTG asked whether these changes would lead to further services being moved out of Hartlepool into other local sites, for example Sedgefield Community Hospital? A4 The Trust has had discussions with Dr Stewart Findlay, Chief Clinical Officer for DDES CCG, and are already engaging with clinical leads, particularly around stroke, to see if Sedgefield Community Hospital can be utilised. The Trust reiterated that it will continue to work to ensure pathways are optimised within the community with key milestones achieved around care closer to home. Q5 Will the seven day working arrangements be affected by the new developments? A5 Seven day working has been in effect in both hospitals for acute services for two years already and this will continue as well as considering the possibility of a seven day working model for outpatients at one site, as this may enhance earlier consultant intervention into the patient’s disease journey. The current seven day working model for intensive care meets national standards. JC – The Trust is working closely with DDES and Easington locality in particular, being part of the Care Closer To Home subgroup taking integrated pathways forward, working collaboratively with Durham County Council and County Durham and Darlington NHS Foundation Trust. Working to improve pathways, recruiting to an older peoples’ team, for example, to ensure pathways are provided in an appropriate setting. Transport HT – The Trust and CCGs will work hard with local authorities to improve all transport issues raised as an outcome from the consultation process; accessibility, cost, travelling time, major areas of deprivation in the area, low numbers of car users. Reassurance has been provided by NEAS that they will work to achieve a sustainable transport system for patients. Q6 KT expressed his gratitude that assurances have been received but asked for more detail about what was planned? A6 RF – This review of hospital services is not a new process for them, successful development models have been formulated previously and NEAS will continue to improve the patient journey. Q7 PB asked what assurance NEAS could provide to patients over concerns whether ambulances having to travel further would affect patient safety. A7 RF referred to appreciation of the skills of paramedics who would receive improved training on top of what they have already. A longer journey would be necessary but paramedics will provide the same care and attention they give to all patients during the journey. Q8 AW – Transport congestion – Has NEAS envisaged further difficulties around this? 7 A8 RF – If an accident happens or congestion occurs vehicles already have direct access to other emergency services and mapping devices. Q9 AD – Parking will be increased with the convergence on North Tees. What is the plan? How does the Trust propose to marry patient appointments up with patient transport timetables? A9 Car parking will be provided on a temporary basis for staff who will move there to create more public spaces. A bid has been placed with the Local Authority for additional car parking spaces and the Trust are working with staff to consider alternative ways of travelling, car sharing, shuttles etc. With regard to Outpatient appointments for patients, particularly the elderly, Patient Transport Service is not part of this consultation but the Trust is looking at alternative travelling times which would be more sensitive to the needs of elderly patients. Volunteer driver scheme extensions are being considered. All were reminded that the Trust relies on the public to alert them to transport issues so they can act. AW also pointed out that transport measures for disability access spaces are being taking into account and CCGs are working collaboratively with Healthwatch with regard to this, ensuring that staff who are also wheelchair-users are considered also. Q10 PB – Could the services have been moved to Hartlepool instead? A10 The Trust considered internal options, ie all acute medicine and intensive care services move to Hartlepool rather than North Tees but due to the fact that these services would not all fit into Hartlepool it was not considered a viable option. Q11 PB – There is space at Hartlepool to build – why not? A11 There is a population in Stockton of approximately 190,000 and 9099,000 in Hartlepool. If a new hospital was built in Hartlepool this would not be central to the whole population and funding was not available. Q12 PB/AW Why was there only one option in the consultation? A12 AW All clinical and quality safety issues were considered and not taken at face value. NCAT assessed independently along with clinical experts who agreed entirely that the option put forward was the only safe and viable one. It would not have been appropriate for an open and transparent commissioning body to then look at other options. Of course if there had been clinical evidence to the contrary other options would have been considered but none were provided. It would have been remiss of the CCG to move forward with the proposals without looking also at the impact on the population and mitigation of issues raised during the consultation process. 6 Summary and Governing Body decisions There were no further questions and AD summed up the discussion and said that the questions asked showed the robustness of the information received. All the information received showed a consistent picture which 8 was reassuring. The summary report was helpful and explained why this change needs to be made. AD asked whether the Trust have plans to implement the changes, and their response was that the Trust does have a plan to implement the changes if approved. The proposed date for implementation is October 2013 to ensure that the changes are made before the onset of winter. AD referred to the County Durham Overview & Scrutiny Committee report – the CCGs would want to ensure that the implementation process was monitored so their suggestion of an oversight group was very helpful. DCC had been part of an oversight group that was set up when changes were being made to County Durham and Darlington FT hospital services and that group gave assurance that issues and actions identified in the consultation were considered and taken forward AD explained that DDES CCG would now hold their Governing Body meeting in pubic and were reminded that the purpose of the meeting in common was to meet together with HaST CCG and the Trust to review the proposal, the outcome of the consultation and assess the robustness of the process and plans. AD formally asked the DDES CCG Governing Body members present to confirm individually whether they were in agreement with the proposal and the plans to address the concerns of the public, the CCG and County Durham Overview & Scrutiny Committee. All members confirmed their agreement subject to plans to address the concerns being in place and implemented. PB explained that HAST CCG would now hold their Governing Body meeting in public and were reminded that they were quorate and that the purpose of the meeting was to receive a presentation from the Acute Trust around the changes to Acute care, the challenges to the Acute Trust, reasons for the changes, to agree that safety issues had been met, with a particular note to transport issues and whether they had reached a decision to support the changes. PB formally asked the HaST CCG members present to confirm whether they were happy to proceed on that basis. All members confirmed their agreement. 7 Next Steps AW summarised the actions which had been identified during the discussion: - Monitoring from the oversight board - Evaluation of the travel plan, ensure that this is working well and delivering sustainable ways of working with partners - Communication with the public – improvement by all 9 - Working with Local Authority colleagues - Monitoring quality and safety - Strengthening local services AW explained that dates are in diaries already for meetings to take plans forward and the Trust and CCGs recognise that steering group members need to be included. This group needs to be extended to ensure the right people are involved, everyone was in agreement that AW would liaise with Stewart Findlay and Mike Taylor from DDES CCG on this as soon as possible to avoid further delays. It was agreed that plans need to be implemented before the winter period (towards the end of October) and information need to be communicated to the public and staff immediately after this meeting, including dates for changes. This communication should also be conveyed to those involved in any pathway changes. The Trust concluded the meeting in common by stating that over the past years the Trust’s Board of Directors have challenged the rationale behind delivering such a plan, internally as well as over the past few months working externally with the CCGs looking at the plans and challenging these again. The process has moved the Trust to a place where it is happy to work very closely together with partners to continue to deliver the safest services possible for their patients. Thanks were given to everyone involved in the work done so far. 8 Any other business None The meeting closed at 3:15 pm. Signed …………………………………………… Name …Annie Dolphin ……………………….. Date ….. 10th October 2013………………….. 10