FREQUENCY AND PROGNOSTIC IMPORTANCE
OF TROPONIN AND CK-MB ELEVATIONS
FOLLOWING CABG: AN ANALYSIS FROM PRIMO
I AND PRIMO II
Robert W. Harrison, MD; Kyle White, MS; Michael J. Domanski, MD; Sorin J.
Brener, MD; Peter K. Smith, MD; Graham S. Hillis, MBChB, PhD; Milo Engoren,
MD; John H. Alexander, MD, MHS; Jerrold H. Levy, MD; Bernard R. Chaitman,
MD; Michael J. Mack, MD; Michael E. Farkouh, MD, MSc; Kenneth W.
Mahaffey, MD
Duke Clinical Research Institute, Durham, NC (RWH, KW, PKS, JHA, KWM); Mouth Sinai School of
Medicine, New York, NY (MJD, MEF); New York Methodist Hospital, Brooklyn, NY (SJB); The George
Institute for Global Health, Sydney, Australia (GSH); Mercy St. Vincent Medical Center, Toledo, OH
(ME); Emory University, Atlanta, GA (JHL); Saint Louis University Sch. of Med., St. Louis, MO (BRC);
Baylor Healthcare, Dallas, TX (MJM)
Disclosures:
R.W. Harrison: None
K. White: None
M.J. Domanski: None
S.J. Brener: None
P.K. Smith: None
G.S. Hillis: None
M. Engoren: None
J.H. Alexander: None
J.H. Levy: None
B.R. Chaitman: None
M.J. Mack: None
M.E. Farkouh: None
K.W. Mahaffey: None
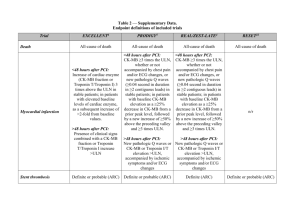
Background
Postoperative myocardial infarction (PMI) is a
serious complication of CABG
Incidence 3-20% depending on the definition
Traditionally, PMI defined by postoperative ECG
evidence of infarction
More recently, CK-MB and troponin have been
incorporated into the definition of PMI
Many contemporary CABG clinical trials have used
a combination of CK-MB elevations and Q-waves on
ECG to define PMI
Background
Troponin replacing CK-MB in the Universal
Definition of Myocardial Infarction1:
Type 5 MI: Postoperative troponin > 10x ULN
when associated with ECG changes, or imaging
evidence of graft loss or new myocardial injury
Prior studies have demonstrated increased risk of
death with elevated CK-MB and troponin2
Most have evaluated categorical elevations in
biomarkers
>5-≤10xULN, >10-≤20xULN, etc.
Little evidence to support the use of specific
biomarker thresholds, particularly for troponin.
1. Thygesen K, et al. Circulation. 2012. 126(16):2020-2035
2. Domanski MJ, et al. JAMA. 2011. 305(6) P.585
Objectives
Population of clinical trial participants who
underwent systematic assessment of CK-MB and
troponin following CABG:
Evaluate the incidence of CK-MB and troponin
elevations over a range of thresholds
Assess the association between CK-MB or
troponin elevations and 30-day mortality
Assess the independent prognostic importance
of ECG evidence of infarction
Methods
PRIMO-I and PRIMO-II:
7,234 patients
Multicenter randomized clinical trials to assess
the efficacy of intravenous pexelizumab in
patients undergoing CABG or combined CABG
and valve surgery
All patients underwent serial CK-MB, troponin-I
(TnI), and ECG measurements over 96 hours
CK-MB: 4, 8, 12, 24, 36, 48, 96 hours
TnI: 24, 48, 96 hours
ECG: enrollment, 48, 96 hours
Biomarkers and ECGs analyzed at a core
laboratory
PRIMO-I and PRIMO-II
Enrolled patient with 1 (PRIMO-I) or 2 (PRIMO-II) of the
following risk factors:
Urgent CABG
Diabetes mellitus
Female sex
Prior CABG
Prior CVA or neurological event
NYHA Class III-IV CHF
2 prior MIs, or recent MI (within 4 weeks of CABG)
Preoperative CK-MB and/or TnI abnormalities
Baseline troponin abnormal in 22.2%
Baseline CK-MB abnormal in 8.0%
Overall 30-day mortality: 3.6%
Methods
Analyzed the distributions of peak postoperative CK-MB
and TnI elevations.
Unadjusted and adjusted hazard ratios for 30-day
mortality determined over a range of thresholds for CKMB and TnI elevations
Cox Proportional Hazards
Multivariate model incorporates the following predictors:
Biomarker above threshold
Presence/absence of new ECG changes
Covariates:
age, sex, previous MI, renal insufficiency, ejection fraction,
diabetes, peripheral vascular disease, hypertension, number
of grafts used, cross clamp time, concurrent valve surgery,
and use of the internal mammary artery
Results: Baseline data
Variable
N
Age, median (IQR)
Overall Cohort
7016
60.0 (58.0-74.0)
Female, %
34.0
White, %
90.6
Ejection fraction, median (IQR)
50.0 (40.0-60.0)
Prior MI, %
36.3
Prior PCI, %
25.1
Prior CABG, %
9.0
NYHA Class III-IV, %
35.8
Concomitant valve surgery, %
14.7
On-Pump CABG, %
97.9
Cross-clamp time, median (IQR)
62 (44-86)
Results: Biomarker elevation distributions
CK-MB
Median, xULN
IQR
6.2
3.9-10.9
Troponin-I
Median, xULN
IQR
21.4
10.3-54
Results: Biomarker and ECG changes
Proportion of patients affected according to:
Biomarker thresholds
Concomitant ECG changes
Biomarker > Threshold
Biomarker > Threshold &
ECG Changes
Threshold
CK-MB
Troponin-I
CK-MB
Troponin-I
5x ULN
61.4%
92.0%
3.8%
4.3%
10x ULN
28.0%
75.8%
2.6%
3.9%
20x ULN
10.9%
52.0%
1.6%
3.5%
40x ULN
3.4%
32.1%
0.7%
2.8%
80x ULN
17.4%
2.0%
100x ULN
14.0%
1.8%
ECG changes: new Q-waves or LBBB on postoperative ECG
Results: Unadjusted HR for 30-day Mortality
Hazard ratios for 30-day mortality were calculated over a range
of peak CK-MB and cTnI thresholds defined relative to the ULN.
Results: Adjusted analysis
Adjusted HR for 30-day mortality
Biomarkers and ECG changes as independent
predictors of death
Biomarker
Threshold
5x ULN
CK-MB >
Threshold
2.3 (1.5-3.5)
New ECG
changes
1.7 (1.0-2.8)
Troponin-I >
Threshold
9.2 (1.3-66.5)
New ECG
changes
1.9 (1.1-3.2)
10x ULN
2.6 (1.8-3.6)
1.5 (0.9-2.5)
2.8 (1.5-5.1)
1.8 (1.1-3.1)
20x ULN
4.7 (3.2-6.7)
1.2 (0.7-2.1)
2.4 (1.6-3.7)
1.7 (1.0-2.9)
40x ULN
7.6 (4.8-11.9)
1.1 (0.6-1.9)
3.0 (2.1-4.2)
1.5 (0.9-2.6)
80x ULN
4.3 (3.0-6.1)
1.4 (0.8-2.3)
100x ULN
4.9 (3.4-7.0)
1.3 (0.8-2.2)
Covariates: age, sex, previous MI, renal insufficiency, ejection fraction, diabetes,
peripheral vascular disease, hypertension, number of grafts used, cross clamp time,
concurrent valve surgery, and use of the internal mammary artery
Limitations
Post-Hoc analysis
Preoperative CK-MB and/or TnI abnormalities
Sensitivity analysis performed
HRs varied <10% after excluding those with baseline
abnormal biomarkers
PRIMO-I and PRIMO-II enrolled patients at intermediate to
high risk of perioperative events
Standard TnI assay used. Results may not be comparable
for high sensitivity assays have lower ULN.
Wide confidence intervals for HRs at low ( 5x ULN for
CKMB, 10x ULN for TnI) thresholds
Few patients with few events
Requires cautious interpretation of these point estimates
Conclusions:
Postoperative increases in CK-MB and Troponin-I are
common
A higher TnI threshold, vs. CK-MB, is required to affect a
similar proportion of patients
CKMB >10xULN (28%) ~ TnI >40xULN (32%)
Concomitant ECG changes occur in a small percentage
of patients
CK-MB and TnI elevations were independently predictive of
30-day mortality at all thresholds > 5 x ULN.
Trend: higher thresholds associated with higher HR
New Q-waves or LBBB were weakly associated with 30-day
mortality
Prognostic importance wanes at higher biomarker
thresholds
 0
0