File
advertisement

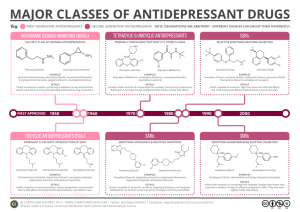
Drugs which can Elevate Mood (Mood Elevators) Definitions Affective disorders - mental illnesses characterized by pathological changes in mood (not thought – compare with schizophrenia) 1. Unipolar disorders Depression – pathologically depressed mood. Mania – excessive elation and accelerated psychomotor activity (rare) 2. Bipolar disorder (manic-depressive illness) – „cycling mood“ severe highs (mania) and lows (depressive episodes) It is common & normal emotion in which people becoming depressed as a result of unfortunate domestic and social conditions, sometimes the depression is disproportionate to precipitating factors or there may be no obvious cause at all. Clinical presentation: Emotional symptoms: Sadness. Hopelessness. Loss of interest in usual activities. Feeling of guilt. Physical symptoms Fatigue Sleep disturbance Pain (especially headache) Appetite disturbance ↑or ↓ Intellectual or cognitive symptoms Decreased ability to concentrate or slow thinking Confusion Poor memory for recent events. Reduced self-esteem & self-confidence. Ideas or acts of self harm or suicide. What is the cause of depression? Monoamine theory Suggests that depression results from functionally deficient monoamine neurotransmitters (Norepinephrine (NE) &/or Serotonin (5-HT)) in the CNS. Therefore, in the treatment we try to ↑ the level of these neurotransmitters Major classes of anti-depressants: 1.Reuptake inhibitors A. Selective serotonin(5-HT) reuptake inhibitors (SSRIs) e.g. Fluoxitine B. Selective norepinephrine(NE) reuptake inhibitors e.g. Reboxitine C. None Selective NE/5-HT reuptake inhibitors(TCAs) e.g. Imipramine ,Amitriptyline 2. Monoamine oxidase inhibitors e.g. Phenelzine 3. Atypical antidepressants e.g. Mirtazapine Tricyclic antidepressants (TCAs) MOA Inhibit reuptake mechanism which is responsible for termination of the synaptic action of NE & 5-HT in the brain Blocking of receptors:TCAs also block muscarinic,serotonin,histamine, α-adrenergic responsible of S/Es Examples: Imipramine, Amitriptyline Therapeutic uses 1.Major depression 2.Some panic disorder respond to TCAs 3.Imipramine has been used to control bed-wetting in children (older than 6 years). Advantages Disadvantages / Side Effects • Often effective in reducing panic attacks and elevating depressed mood. •Usually a single daily dose Anticholinergic : dry mouth, blurred vision constipation, urinary retension Antihistaminergic : Sedation Alpha blockade : Postural hypotension medicalquery@torrentpharma.com 12 S/Es Antimuscarinic: constipation, blurred vision, urinary retention, dry mouth Sedation Postural hypotension Arrhythmias Weight gain Selective Serotonin Reuptake Inhibitors (SSRIs) MOA :Blocks serotonin reuptake only Examples: Fluoxetine SSRIs have little activity to block muscarinic, histamine H1, α-adrenergic receptors & relatively safe in over dose Therapeutic uses 1.Primary indication is depression 2.Obsessive compulsive disorders 3.Fluoxetine is effective in treating bulimia nervosa. Unwanted effects: In combination with MAOIs ,SSRIs can result in “serotonin syndrome” Monoamine Oxidase Inhibitors (MAOIs) MOA: Inactivate monoamine oxidase A & B enzymes, permitting neurotransmitter molecules to escape degradation (↑ NE & 5-HT levels) MAO is a mitochondrial enzymein the brain, gut and liver. Example: phenelzine MOA of MAO inhibitors Indicated for depressed patients who are unresponsiveness or allergic to TCAs Because of their risk for drug & drug food interaction, MAOIs are considered to be the last line agents. S/Es: Hypertensive reaction may occur in patients taking MAO inhibitors and consume Tyramine containing food (“cheese reaction”) (as aged cheeses, beer, red wines) Pharmacology of theTyramine Reaction Tyramine Non-Selective MAO Inhibitor Tyramine Hydroxyphenylacetic acid (inactive) MAO-A X MAO-A Norepinephrine (NE) displacement NE NE NE ( NE NE NE Sympathomimetic Response NE NE NE Blood Pressure) A persistent headache is often a warning of rising blood pressure in patients on MAOIs.. Drug Choice Comparisons of the antidepressants showed that they are roughly equivalent in efficacy. Individual patients may respond better to one drug than to another. SSRIs are not sedative, safe in overdose and have mild adverse effects so they are widely prescribed. Finding the right drug and the right dose must be accomplished empirically. Bipolar Disorder - image Bipolar Disorder - image Drugs used in Mania – Mood Stabilizers The main goal of pharmacological treatment of bipolar disorder is to reduce the frequency & severity of fluctuations in mood. Lithium Carbonate Alternative Drugs: Carbamazepine Sodium Valproate Mood stabilizing drugs e.g Lithium salts Therapeutic uses: used prophylactically for treating manic-depressive disorder & in the treatment of mania. It is Teratogenic. Has a narrow therapeutic index, frequency & severity of adverse reactions is directly related to the serum levels. Monitoring plasma concentration is essential, especially in presence of renal disease. Main unwanted effects: tremor, hypothyroidism, thirst & polyuria. Different preparations of lithium vary in their bioavailability and patients should receive only one preparation. they should maintain a reasonable fluid intake. Record cards are available for patients taking lithium. Think Positive! Thank You