PH711: Space medicine
advertisement

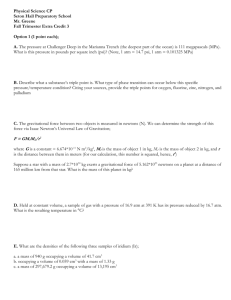
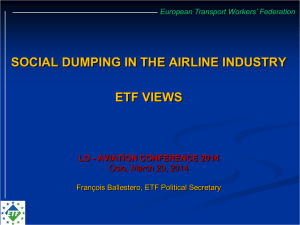
Review the effects of being in space on the human body: ◦ ◦ ◦ ◦ ◦ Effects of acceleration/deceleration Air pressure (or lack thereof!) Temperature and humidity Weightlessness (immediate and extended) Ionising radiation “Space Physiology and Medicine” by Nicogossian, Huntoon and Pool. Published by Lea & Febiger. ◦ Library classmark – RC1150 Accelerations (and conversely ‘decelerations’) are given units of ‘g’ – multiples of Earth standard gravitational acceleration (9.81ms-2) Large, sustained accelerations are not natural. Sustained here means tens → hundreds of seconds. Need a velocity of ~8 km s-1 to reach Earth orbit. Launch lasts a few hundred seconds. Area under the graph is the ‘g secs’ total. To achieve Earth orbit approximately 815 g secs are experienced by an astronaut Mercury acceleration profile (Friendship 7) Both launch and re-entry result in a series of sharp jolts to the astronauts against a modest g (>1) continuum. How the body responds is the main medical issue. ◦ The change in blood pressure, especially blood flow to the brain and eyes. ◦ Damage to lung tissue Blood pressure: pressure exerted by the blood on the walls of blood vessels. During each heartbeat blood pressure varies from a maximum (‘systlolic’) to a minimum (‘diastolic’ ) pressure. Normally measured at a person’s upper left arm (BP varies throughout the body, so need a ‘standard’ reference point). Units of blood pressure are ‘millimetres of mercury’ (mmHg). [1 mmHg ≡ 133 Pa, ρHg = 13534 kg m-3] Normally quoted as two numbers systolic over diastolic pressure. i.e., “110/70” Average values vary widely but ‘normal’ is considered to be in the range 110/65 – 140/90 Under normal conditions there is approximately a 20mmHg pressure difference between the pressure leaving the heart (cardial), and the pressure of blood entering the brain (cerebral). This difference is merely due to the heart having to pump against gravity. Under vertical acceleration, an additional gravitational force (>1g) acts against the heart causing a drop in cerebral pressure. For accelerations >4.5g this causes the cerebral blood pressure to drop to zero (hypoxia). As the brain has no long term store of oxygen, this causes unconsciousness within 6-7 seconds. Extended periods cause brain damage through necrosis (tissue death) and death. Just as there is a drop in pressure in the brain, there is an increase in pressure in the lower parts of the body (legs and abdomen) as the blood accumulates. This in turn restricts the amount of blood flowing back to the heart, the heart then restricts its output, further reducing blood pressure (the dizzy feeling that some people get when they stand up suddenly). This ‘negative’ feedback process causes cerebral pressure to drop even further. The eye is also very sensitive to blood pressure changes. It has an internal vitreous humour pressure of ~20 mmHg. Blood flowing to the retina must have a pressure greater than this pressure. As blood pressure drops, peripheral vision is lost, then finally central vision (non-permanent damage, if blood supply is restored within minutes). Occurs (just) before unconsciousness. How does the body react to these effects? ◦ The carotid artery in the neck (right) has receptors which detect BP changes. ◦ As BP lowers smaller arteries constrict to increase BP. ◦ Heart beat also increases to keep blood volume constant ◦ The pooling effect of blood in the lower body is a one-off event. It takes the body ~10 seconds to restore normal blood volume (some people get dizzy if they stand up suddenly, particularly if you are borderline hypotensive). Acceleration also ‘squashes’ soft tissue. Lungs are soft bags which are squeezed during acceleration. This causes various effects: ◦ Blood is squeezed out of the lungs, and affects oxygen intake. ◦ The oxygen/CO2 exchange mechanism is compromised leading to a build-up of CO2 in the blood. ◦ Very high accelerations (>15g) can lead to tearing of lung tissue, lung cavity distortion and oxygen starvation. ◦ Soyuz 18 crew experienced re-entry acceleration ~20g and one of the crew never flew again due to internal damage. Technological solutions: ◦ Breathing high pressure gas. Counteracts the gforces acting on the lungs ◦ Wearing ‘g-suits’ (as used by combat pilots). These squeeze the legs and abdomen reducing the amount of ‘pooling’ that occurs and keeping BP high. ◦ Change the astronaut’s position so that highest-g is experienced in the least sensitive direction. Astronauts need to breath. Two ways of supplying oxygen: ◦ Have astronauts remain in pressure (space) suits, and supply oxygen from tanks or umbilicals. Ok for short flights (Mercury, Vostok). Impractical for long duration flights. ◦ Have a sealed and pressurised cabin to allow crew to move and work freely. More complicated. Minimum pressure humans can operate in is approximately 6% of standard atmospheric pressure (using pure oxygen). ◦ Limited by oxygen consumption within the body ◦ Lower pressures can cause the evaporation of bodily fluids (water, mucous membranes etc.) ◦ Haemorrhaging of surface capillaries. ◦ Would probably be very uncomfortable High pressures also problematic as loss of cabin pressure would amplify the effects of decompression (due to the larger pressure differential between the cabin and vacuum). 4 main concerns ◦ Barotrauma. Caused when gas is trapped within the body due to external pressure changes. Mainly lowering of pressure, but increasing pressure can cause severe ear pain resulting in rupturing of the tympanic membrane). Large pressure differentials can cause severe pain. ◦ Examples: middle ear, sinuses, teeth fillings and the gut (long haul aircraft lower pressure in the passenger cabin). Astronauts have had their fillings replaced during training to stop this effect in teeth. ◦ In the Spaceshuttle, normal pressure is 1 atm (~105 Pa) but can be controlled. Prior to an EVA pressure is reduced to 0.69 atm and the rate of change is limited to 0.007 atm/sec – 0.07 atm/sec (in an emergency). ◦ Explosive decompression (everyone’s favourite). ◦ A pressure change so great and rapid that any gas trapped within the body cannot flow out to equalise the pressure. The result is a transient overpressure. A transient overpressure ~0.1 atm can rupture the lungs. Capillaries in the alveoli of the lungs rupture leading to bleeding and ‘frothing’ of blood and air in the lungs. ◦ Leads to embolisms (air bubbles in the blood) which get trapped and occlude blood vessels. Almost certainly fatal. ◦ Swelling and rupturing of capillaries on the skin and cornea (unpleasant, but probably not fatal). ◦ A pressure differential of 1 atm does not cause people to explode and people (or aliens) do not get sucked out of small holes. The results of explosive decompression depend on: 1) Starting pressure 2) Rate of change of pressure 3) Absolute change in pressure 4) Ratio final/starting pressure 5) Ratio of lung volume at time of decompression to maximum lung capacity 6) Ratio of venting area in cabin to airway orifice of lung Example: If a cabin leak occurs from a small hole, the size of which is comparable to the opening from the mouth to the lungs (glottis). Flow rates will be similar and lung pressure will drop with cabin pressure. If this is not the case, lung volume will try to expand to permit equalization of pressures. If this expansion is limited (i.e. reach capacity of lungs) before equalisation of pressure, the difference determines if rupture occurs (i.e. greater than 0.1 atm ?). In the Space-shuttle, the risk of decompression limits the ejection altitude. Above certain altitudes is can only occur is the crew wear oxygen masks. Non-explosive decompression ◦ Slow decompression itself is a problem. Decompression sickness (the ‘bends’) occurs when the pressure of gases dissolved in a bodily fluid (normally the blood) exceeds the ambient pressure. ◦ The gas evolves from the blood (i.e., it forms bubbles – think of opening a bottle of fizzy water). ◦ Bubbles in the blood are generally bad news. Can form embolisms (blockages) and cause severe pain in joints and lungs. ◦ Problems occur when dissolved gas pressure / ambient pressure is >1.3. ◦ Bubbles are removed via the lungs and the dissolved gas pressure equalises eventually. ◦ Different gases equalise at different rates: oxygen equalises within seconds → minutes. Nitrogen takes minutes →hours. This is one reason why pure oxygen is used. ◦ Soyuz 11 (1971) crew killed when a valve opened at too high an altitude during re-entry and vented the atmosphere. No spacesuits meant the crew suffocated. Pre space-shuttle NASA flew missions at 33% atm pressure (pure oxygen). EVA suits had pressures of 25% atm so moving from one to another didn’t cause decompression problems. Spaceshuttle flies with an atmosphere of 1 atm. EVAs have to be carried out at 25% atm due to pressure constraints in a ‘soft’ suit. The astronaut therefore has to go through a decompression procedure to allow for EVAs 1. 2. 3. 4. 1 hour pure oxygen at 1 atm 70% atm at 26.5% oxygen for 24 hours 40 minutes in spacesuit (prior to EVA) at 70% atm and 100% oxygen Reduction to 25% atm and pure oxygen in airlock prior to EVA. Why so complicated? Various procedures tried (on the ground) to check whole body washout times of dissolved gases. This procedure reduces the chances of decompression sickness (~1%). Altitude sickness This occurs due to poor oxygen pickup at low pressures. At sea level the partial pressure of oxygen in the air is 3.06 psi. In the STS it is 3.2 psi. In the alveoli (small sacs in lung tissue where gas exchange occurs) the partial pressure is 2.01 psi. Problems of oxygen uptake occur if this is not maintained. If there is less oxygen (this falls with altitude, hence the name), the height at which an individual can still take enough oxygen is approx. 1830m, where alveoli oxygen pressure is 1.50 psi. Above this altitude problems appear progressively. When the problem occurs the symptoms are; vision impairment, loss of breath, exhaustion, reduced mental capacity (e.g. confusion, poor learning ability), motor impairment. Finally at 0.67 psi unconsciousness occurs. Equally, high alveoli oxygen levels ( > 2.01 psi) are bad. This results in oxygen toxicity. Note however, that oxygen concentrations themselves are not the problem, the pressure is also important. (Mauna Kea observatory in Hawaii is at 4000 m – working here is like having a constant stinking hangover). CO2 This is a product of respiration. On Earth it comprises 0.04% of the atmosphere by concentration. But in an enclosed space with crew this builds up. Extra CO2 causes increases in heart rate, respiration rate, and changes acid base of the body. On STS, CO2 is limited to 0.15 psi, above this there is a mission contingency, i.e. crew don breathing masks if it reaches 0.30 psi (2% CO2). The CO2 content in a cabin is controlled by scrubbers. These are usually chemical absorption devices, i.e. cans of chemicals (e.g. lithium hydroxide) which react with CO2, trapping it in their volume. These cans have finite capacity, so on space stations they need regular replacement (cf. the weekly house keeping on Salyut/Mir). Cans can be recycled. When heated they release their CO2. If this is done in a sealed port and vented externally, they can then be reused. On the STS the cans are disposable. 2LiOH (s) + CO2 (g) → Li2CO3(s) + H2O(g) 1% ≡ 0.01 atm ≡ 0.147 PSI Water vapour. Percentage humidity is water vapour pressure/max water vapour pressure in the atmosphere at the given temperature. High relative humidity is associated with condensation (on any local relatively cool surfaces), and is conducive to microbial and fungal growth (and electrical short-circuits). It is thus to be avoided. Absolute humidity is also important (i.e. actual partial pressure of water vapour). Low humidity causes dry eyes and skin, as well as dry mucus membranes, chipping of lips etc. Breathing tract suffers damage and this in time encourages respiratory illness. High percentage humidity is uncomfortable. Humidity also affects heat loss and heat balance. 0.19 psi is optimal for habitability (relative humidity ~30-60%). STS maintains 0.12 to 0.27 psi. Temperature. Bodies perform best within an optimum temperature range. Outside this range shivering/sweating try to correct imbalance in body temp. This causes discomfort/impairs performance. Oddly no single optimum temp exists, it varies from person to person by 5oC. STS maintains temp between 18 and 27oC. Crew wear/discard light clothing to suit themselves. The operation of apparatus inside the STS means that in normal flight the problem is one of reducing cabin temperature. This is done via heat pumps which redistribute heat to radiators mounted on the interior of the cargo bay doors. It is thus essential that these are opened as early as possible into a mission. Failure to open the doors can require an abort of the flight. Temperature Hyperthermia (‘heat stroke’) occurs when the body temperature rises above 40.6oC. Symptoms include red and hot skin, sweating, nausea, confusion. Hypothermia occurs when the body temperature drops below 35oC. Symptoms include shivering, numbness in extremities (blood vessels constrict to reduce heat loss through radiation). Humans can only exist in a narrow range of temperatures without thermal protection (it gets uncomfortably cold below 10oC and hot above 35oC – but this is humidity dependent). Toxic gas build-up. Venting of fumes from rocket exhausts into the cabin is a design flaw that occurred on several early missions What usually happened was that during descent pressure equalisation of cabin and exterior occurs. This can permit drawing of fumes into the cabin. Apollo-Soyuz mission: a valve opened prematurely and nitrogen tetroxide gas (a fuel oxidiser) was sucked into the spacecraft. All 3 astronauts suffered gas poisoning and inflammation of the lungs (pulmonary edema) and spent two weeks in hospital. Today the STS has potential problems after landing, as fumes can build up in nozzles etc. and then disperse as a cloud around the landed shuttle. So crew disembark into a cabin with its own air supply. After earlier STS missions the crew sat in the craft until external monitoring indicated no hazard. Toxic gas build-up Fumes can also build up in a cabin during a mission. Outgassing of materials releases gases which can be poisonous. On Earth these are simply vented away. In flight they accumulate. The result is that you need ‘scavengers’ to remove toxic chemicals or gases, or you need to prevent the flight of any material subject to outgassing. NASA has strict ratings as to permitted outgassing of materials. This also limits the amount of scientific or engineering work that may be carried out in the crew area. Clearly no process can occur which releases fumes into the crew atmosphere (or which consumes oxygen !). The atmosphere therefore has to be circulated (and ‘scrubbed’). Fire A separate issue not strictly related to atmospheres is the need to avoid fire. This consumes oxygen and can release poisonous gases. The oxygen resupply and toxic gas removal systems have limited capacities, and finite response times. If the oxygen content is high, or has been increased in preparation for an EVA, flash fires present an enormous hazard (Apollo 1 crew were killed (1967), the Soyuz T-10-1 crew barely escaped (1983)). Smoke from a fire can fill the cabin and make movement difficult to carry out. Fire is thus a hazard that requires major efforts to avoid, and serious countermeasures. Weightlessness (well, ‘microgravity’) During spaceflight the most dramatic effects on the body are associated with microgravity The body was has evolved for a 1 g constant load in the vertical, with regular periods of rest perpendicular to this. Spaceflight violates this natural order of things. The effects on the body’s systems are varied and include: ◦ ◦ ◦ ◦ balance (neurovestibular system), bones (calcium loss), muscle (nitrogen loss) cardio-pulmonary system Balance and Space Motion Sickness (SMS) The most obvious external symptom is that 50% of astronauts suffer from space nausea. Some experience discomfort, others the onset of stomach heaving, and some are simply sick. Onset of symptoms is very rapid once orbit is achieved. It can take 8 hours for the worst to pass, and then almost all astronauts recover. Earlier astronauts had a much lower incidence of illness (indeed there were virtually no reports of illness during the early sixties). It was therefore supposed that some change in mission organisation had triggered the onset of nausea. The most obvious change was that early astronauts had been securely strapped in, with no freedom of movement. The surfaces in their cabin were fixed relative to them, and horizons were thus fixed. It was supposed that later missions, where crew had freedom of movement, confused the crew with a mismatch of horizon and expectations. Result nausea. Travel sickness (or ‘earth motion sickness’ - EMS, sea sickness) are very similar. Long periods watching a rushing past landscape, whilst local objects are stationary. Sends conflicting messages to the brain. This has been tested by NASA. They constructed a room, with a chair which slowly rotated with both pitch and yaw. Candidates then had to carry out tasks, alternatively focusing on their hands and the background. A sequence of 1200 hand eye coordinated movements is required. No candidate completed the sequence first time without illness. Seeming confirmation of the theory. Repeated tests increase the tolerance to this problem. Drugs administered before the tests also increase tolerance. The neurovestibular (‘balance’) system is also affected. The three semi-circular canals (superior, posterior and horizontal) contain a viscous fluid that brushes against hairs on the internal surface of the cochlea. In μg this fluid is no longer flowing under gravity and leads to conflicting nerve impulses. The left and right ears may also be affected differently. Leads to dizziness and nausea In μg blood also tends to migrate upwards – probably due to the way blood flows from the heart (initially upwards to the brain). This causes increased pressure on blood vessels and nerves, again leading to dizziness and nausea. Tests carried out on Earth indicate there is a difference between EMS and SMS. Spontaneous vomiting is very rare in EMS, but common in SMS. SMS normally improves within a few hours, but some astronauts have suffered for 2 – 4 days.