Principles of antimicrobial therapy in the field of UTI
advertisement

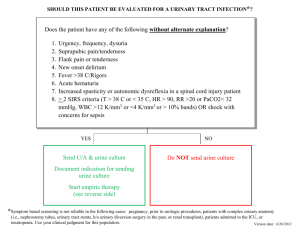
07년 대한요로감염학회 춘계학술대회 The Principles of antimicrobial Therapy in Urinary Tract Infection Wan-Shik Shin, MD Division of Infectious Diseases Department of Internal Medicine The Catholic University of Korea, Seoul, Korea 나이와 성별에 따른 역학적 특성 age (yr) females prevalence risk factors anatomic or functional urologic abnormalities males prevalence 1% risk factors <1 1% anatomic or functional urologic abnormalities 1-5 4-5 % congenital abnormalities, vesicoureteral reflex 0.5 % congenital abnormalities, uncircumcised penis 6-15 4-5 % vesicoureteral reflex 0.5 % none 16-35 20 % sexual intercourse, spermicide use, diaphragm use 0.5 % homosexuality, uncircumcised, HIV infection 36-65 35 % gynecologic surgery, bladder prolapse, postmenopausal estrogen deficiency 20 % prostatic hypertrophy, obstruction, surgery, catheterization >65 40 % as for those age 36-65, plus incontinence, chronic catheterization 35 % as for those age 36-65, plus incontinence, longterm catheterization bacterial attributes host factors capsular antigens hemolysins renal calculi urease ureteric reflux adhesion to uroepithelium (e.g. P fimbriae in E. coli) Introital colonization tumors in & adjacent to urinary tract pregnancy, bladder stones neurologic problems: incomplete bladder emptying large volume of residual urine loss of sphincter control prostatic hypertrophy short urethra in women catheterization catheterization Bacterial attributes and host factors favoring UTI 요로감염 type에 따른 원인균 Microbe E. coli S. saprophyticus Proteus Klebsiella Enterococci Pseudomonas Mixed Other Yeast S. epidermidis acute uncomplicated cystitis (%) acute uncomplicated pyelonephritis (%) complicated UTI (%) catheterassociated UTI (%) 79 11 2 3 2 0 3 0 0 0 89 0 4 4 0 0 5 2 0 0 32 1 4 5 22 20 10 5 1 15 24 0 6 8 7 9 11 10 28 8 Am J Med 1987;82(S4):278 outpatients Hospital inpatients % % 40 3 7 80 3 6 4 E.coli Coagulase-negative staphylococci Other Gram (+) e.g. S. epidermidis, S. aureus, E. faecalis Common causes of UTI 16 25 11 5 Candida Proteus mirabilis Other Gram (-) e.g. Klebsiella, enterobacter, Serratia, P. aeruginosa Laboratory Diagnosis of UTI (I) • Urinalysis with microscopy – The presence of RBC & WBC, although abnormal : not necessarily indicative of UTI – Gram stain : 1 organism/X1000 105 CFU/mL – Dipstick test : nitrite, leukocyte esterase activity • Hematuria – infection of the urinary tract and elsewhere(e.g. endocarditis) – Renal trauma, calculi, urinary tract carcinomas – Clotting disorders, thrombocytopenia • Pyuria: ≥10/HPF(X400) Urine collection Midstream clean-catch urine collection Urine collection (II) Women with symptoms of cystitis (mean age : 21 years) Clean container without performing any cleansing(n=77) Midstream clean catch technique(n=84) Midstream clean catch technique and used a vaginal tampon(n=81) 29% 32% 31% Contaminated: mixed flora, <104 CFU/mL Lifshitz E. Arch Intern Med 2000;160:2537-2540 Quantitative Culture of Urine DDx : Infection or Contamination 0.001ml 백금이 정윤섭, 진단미생물학 제2개정판 pp.95 Significant bacteriuria • 1950s, Kass : ≥ 105 CFU/mL in 2 consecutive midstream urine samples • Revised definition – women with Sx of uncomplicated cystitis • ≥ 103 CFU/mL + pyuria : sen. 80%, spe. 90% : IDSA • 실제 임상에서 균배양은 필요없음 ∵ 감수성이 비슷, 결과가 늦음 • Hx 만으로도 ≥90%에서 충분 dysuria & frequency without vaginal discharge/irritation – uncomplicated pyelonephritis & men with UTIs • ≥ 104 CFU/mL + pyuria – complicated UTIs • ≥ 105 CFU/mL +/- pyuria • 주의 깊은 해석이 필요 : 검체의 종류, 배양된 균종의 수 • ≥ 2 균종, ≤105 CFU/ml : contamination ? number of patients infected not infected significant bacteriuria 10 102 103 104 105 106 107 No of bacteria/ml of urine no prompt delivery or bad collection probable infections but require confirmation Significant bacteriuria Asymptomatic bacteriuria When to screen & when to treat ? • Definition : bacteria in urine without clinical Sx & sign of UTI microbiologic definition : ≥105 CFU/ml of organism(s) in 2 consecutive urine specimens • Clinical importance ? UTI complication : harmful ?, cross-protective effect : beneficial ? • Recommendations for screening & Tx beneficial : pregnant women, before traumatic GU procedure may be beneficial : K/T recipient (≤6 mo), women c persisent cath. acquired bacteriuria after cath. removal not beneficial : healthy infants, girls, women/men, elderly men/women in community or long-term care facilities, pts c diabetes or HIV infection, pts with short-term or chronic indwelling urethral catheters, pts with intermittent catheterization, pts with neurologic impairment of bladder emptying, pts with chronic urologic device 일반적 치료원칙 (I) • 치료 시작 전: 그람염색, 소변배양 등을 통해 감염여부 확인 (예외) 이후 배양검사에서 원인균이 밝혀지면 감수성있는 항생제 선택 • 지역사회획득 감염, 특히 초감염 : 대부분 항생제에 감수성인 균주 • 반복감염, 요로 처치를 받은 사람, 최근 병원 입원 : 내성균주 의심 • 선택 항생제 : 혈중농도보다 소변내 농도가 중요 • 치료기간 : 단순 하부요로 감염 ; 단기치료, 상부감염 ; 더 장기간 치료 • 폐쇄와 결석과 같은 감염 선행인자의 교정 일반적 치료원칙 (II) • 치료가 끝난 후 평가 : 증상 소실 ≠ 세균학적 완치 ≠ 치료 완료 - 실패 vs 완치 ? - 재발 (recurrence) 재감염(Reinfection) vs 재발 ? 조기 (치료 후 ≤ 2주) vs 후기 재발 ? • 조기 재발 상부요로의 감염이 완치되지 않아 재발 : 많지 않음 균주의 지속적 질내 정착에 인한 재감염 : 흔함 (특히 방광염 단기치료 후) • 후기 재발 대부분 새로운 균주에 의한 재감염 이전에 감염되어 질과 직장에 정착한 균주 재발(relapse) • 신장침범, 요로계의 구조적 이상이나 신석, 만성 세균성 전립선염 등 host factor 여부를 확인 • 구조적 이상이 없는 재발의 치료 세균뇨가 없어질 때까지 치료 치료 중 세균뇨가 지속되거나 다시 세균뇨가 나타나면 항생제를 바꿈 • 치료기간 단기 또는 7~10일 치료한 경우 : 2주간 치료 2주 치료한 경우 : 4~6주 치료 6주 치료한 경우 : 6개월 이상 치료 • 치료 중 검사 매달 요배양 검사, 장기치료를 받는 환자는 Ccr 측정과 1-2년마다 IVP Factors in selecting antibiotics for the empiric Tx of uncomplicated UTI • Antimicrobial spectrum • Pharmacokinetics : infrequent dosing intervals • Local prevalence of resistance • Duration of adequate urinary levels (including renal tissue) above the infecting organism’s MIC : important ! ex) shorter T ½ of ß-lactams : poor efficacy • Effect of the antimicrobial on the fecal & vaginal flora little effect on anaerobes : TMP-SMX, 1º & 2º fluoroquinolone • Potential for undesirable side effects • Cost of the treatment regimen • Public health concerns about resistance Antimicrobial Resistance : prevalance • Significant increase in resistance among E. coli • • • • TMP-SMX U.S.A. : < 20%, Europe : < 35%, Korea : 40-50% Fuoroquinolone U.S.A. : < 2.5%, Europe : < 37%, Korea : 15-20% Nitrofurantoin excellent activity & low resistance against E. coli but no activity against non-E. coli isolates : 10-30% in Korea ß-lactams : no recommendation for 1st line empiric Tx ampicillin : 26-38%, 60-70% in Korea cephalothin : 28-39%, 20-30% in Korea Uncomplicated UTI Tx guidelines by IDSA (1999) Acute uncomplicated pyelonephritis • Mild case oral fluoroquinolone (A,II) or TMP-SMX (B,II) for 7d (B,I) likely GPC : amoxicillin/clav. alone (B,III) • Moderate to severe case : admission for parenteral Tx fluoroquinolone (B,III) or aminoglycoside ± ampicillin (B,III) or extended spectrum cephalosporin ± aminoglycoside (B,III) GPC : ampicillin-sulbactam ± aminoglycoside (B,III) switch Tx to oral antimicrobial with improvement (B,III) duration : moderate case : 7 d (B,I), severe case : 14 d (A,I) Uncomplicated UTI Tx guidelines by IDSA (1999) Acute uncomplicated pyelonephritis • Mild case oral fluoroquinolone (A,II) or TMP-SMX (B,II) for 7ds (B,I) likely GPC : amoxicillin/clav. alone (B,III) • Moderate to severe case : admission for parenteral Tx fluoroquinolone (B,III) or aminoglycoside ± ampicillin (B,III) or extended spectrum cephalosporin ± aminoglycoside (B,III) GPC : ampicillin-sulbactam ± aminoglycoside (B,III) switch Tx to oral antimicrobial with improvement (B,III) duration : moderate case : 7 ds (B,I), severe case : 14 ds(A,I) 요로감염 치료를 위한 접근법 a. b. c. d. e. f. g. 요로감염 증상이나 요로계 폐쇄가 없는 임산부가 아닌 성인에서는 치료할 필요없음 모든 소아와 남자에서는 영상검사를 하여 의미있는 병변을 교정해야 함 임산부, 소아, 요로폐쇄가 있는 성인에서는 추적 배양검사가 필요함 임산부는 매달, 소아는 6주와 6개월에 추적 배양검사가 필요함 만성 세균성 전립선염 유무 평가가 필요함 임산부에서는 분만 후 2 개월로 연기함 여성에서는 3∼4회 재감염이 있을 경우 영상검사를 고려함 세균성 요로감염의 치료 임상진단 특징적인 병원체 고려할 사항 치료기간 및 선택항생제 여성에서 발생한 단 순 급성 방광염 E. coli, S. saprophyticus, P. mirabilis, K. pneumoniae 없음 3일 요법: 경구 TMP/SMX, TMP, quinolone 당뇨, 7일 이상의 증상, 최 근 요로감염, 65세 이상, diaphragm으로 피임 7일 요법: 경구 TMP/SMX, TMP, quinolone 임신 7일 요법: cefpodoxime proxetil, TMP/SMX, amoxicillin(/clavulanate) 경증 또는 중등증, 오심/구 토 없는 경우; 외래치료 경구 quinolone 7~14일(필요시 초기용량은 정주), ceftriaxone 또는 gentamicin 일회 정 주 후 경구 TMP/SMX 14일 중증, 패혈증 우려, 임산부; 입원치료 ceftriaxone, quinolone, gentamicin 또는 aztreonam을 해열때까지 정주 후 경구 quinolone, cephalosporin 또는 TMP/SMX 14일 경증 또는 중등증, 오심/구 토 없는 경우; 외래치료 경구 quinolone 10~14일 중증, 패혈증 우려; 입원치 료 ampicillin + gentamicin, quinolone, ceftriaxone, aztreonam, ticarcillin/clavulanate, imipenem-cilastatin 을 해열때까지 정주 후 경구 quinolone 또는 TMP/SMX 10~21일 여성에서 발생한 단 순 급성 신우신장 염 E. coli, P. mirabilis, S. saprophyticus 여성, 남 성에서 복 잡 요로감 염증 E. coli, Proteus, Klebsiella, Pseudomonas, Serratia, enterococci, staphylococci THANK YOU !