NEPHROLOGY FOR STEP 3
By James K. Rustad, M.D.
Copyright © 2009 All Rights Reserved.
Outline
Renal Failure (Post-Renal, Pre-renal and Intrarenal)
Glomerulonephritis
Nephrotic syndrome
Acid-Base Disturbances
Imbalances of Sodium
Post-Renal
Distended bladder on
exam.
Large volume diuresis
after passing urinary
catheter.
Bilateral
hydronephrosis on
ultrasound.
Post-void residual >
200 ml is suspicious.
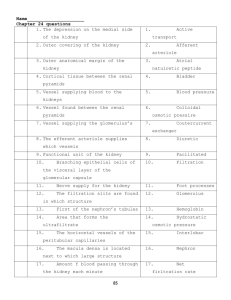
Black arrow = renal capsule
Black arrowhead = sinus fat
White arrow = dilated calyx
White arrowhead = renal cortex
Hydronephrosis
Large hypoechoic area
(black on U/S = no
echoes) in center of
kidney. Dilation extends
into the parenchyma. The
normal hyperechoic area
in the center of the
kidney (hilum) is
replaced by a large
hydronephrotic renal
pelvis. This kidney has
hydronephrosis due to
obstruction of upper
ureter.
Treatment of Obstruction
Lower tract: Foley cath.
Upper tract: Ureteral
stent or percutaneous
nephrostomy.
Pre-renal
Hypotension.
Hypovolemia
(decreased renal
perfusion).
CHF: pump doesn’t work,
can’t perfuse kidney.
Constrictive pericarditis:
heart cannot fill, can’t
perfuse kidney.
GI Bleed (digested
blood is source of urea).
Excess diuresis.
Dehydrated patient
may have high BUN
(azotemia) due to lack
of fluid volume to
excrete waste products.
Nothing wrong with
kidney itself – will try to
absorb sodium to
maintain volume.
Treat the underlying cause! Prerenal usually improves with IVF
Pre-renal vs. Renal
Pre-renal
Renal
BUN/Creatinine
>20:1
<20:1
Urine sodium
< 10
20
FENa
<1
>1
Intra-Renal
Acute Tubular Necrosis
(ATN)
Caused by
hypoperfusion to the
point of tubular cell
death or from toxic
injuries.
Muddy Brown Casts
ATN (continued)
Contrast Nephropathy
Typically begins
immediately after study.
Renal function recovers
after 3-5 days.
Prevent: Hydration, ½
NS 75 cc/hr 8-12 hr
before and after study.
Acetylcysteine 600 mg
BID for 2 days if
diabetes, CHF, CRI.
Aminoglycoside Toxicity
Begins at least 5 days
after treatment.
Rhabdomyolysis leading to ARF
Labs: CPK elevated, Urine
dipstick (urinalysis best
initial test) shows blood
but no RBC on microscopy.
Urine myoglobin most
accurate.
Tx: IVF, IV sodium
bicarbonate to alkalinize
urine to solubilize
myoglobin.
Mannitol and diuresis
decrease contact time of
myoglobin with tubule.
Clinical Situation
Patient is brought to the
emergency room after a
seizure leading to
prolonged immobility on
sidewalk. Next step?
A) Urinalysis
B) Urine Myoglobin
C) EKG
D) CPK
E) Phosphate level
F) Creatinine
Acute Rhabdomyolysis
EKG most urgent step.
Severe muscle necrosis
leads to Hyperkalemia.
Look for peaked T
waves. Treat with
immediate IV calcium
gluconate, insulin,
glucose.
Order Potassium level
(cellular destruction).
Order Calcium level
(hypocalcemia):
damaged muscle may
bind increased calcium.
Hyperphosphatemia
may lead to calcium
binding with phosphate.
Order chemistries to
detect decreased serum
bicarb.
Acute Interstitial Nephritis
The Pentad:
Acute Renal Failure
Fever
Rash
Arthralgia
Peripheral blood
eosinophilia
Urine: WBC casts,
eosinophil positive
(Wright Stain)
Causes: Penicillin, Sulfonamide,
Rifampin, Allopurinol, Indinavir,
5-aminosalicylates, Proton Pump
inhibitors.
If NSAID induced: Fever, rash,
eosinophilia, eosinophiluria
usually absent.
Treatment: Stop medication!
Prednisone may be prescribed.
Glomerulonephritis
RBC Casts, Dysmorphic RBC
Hematuria, proteinuria, HTN
Causes:
IgA Nephropathy
Post-streptococcal GN
Wegener’s granulomatosis
Goodpasture Syndrome
Endocarditis
Lupus Nephritis
IgA Nephropathy (Berger’s Disease)
History of URI 1-2 days before presentation + Painless
recurrent hematuria
Recurrent hematuria following exertion
Serum IgA increased in 50% of patients
Normal complement
Renal Biopsy to confirm
Treatment: ACE inhibitor and ARB
Consider adding Fish Oil
Prednisone if tx-refractory or nephrotic
syndrome/markedly proliferative disease.
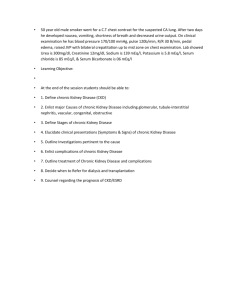
IgA Nephropathy Biopsy: Mesangial
Hypercellularity
IgA Nephropathy Immunofluorescence
IgA mesangial deposits =
characteristic and defining
feature of the disease
Deposits are exclusive of
IgA in only ~26% of
cases; usually
accompanied by IgG
(~37%) or IgM (~13%),
and the three Igs may be
present in ~25% of cases.
However, IgA must be
dominant or codominant
Post-streptococcal GN
URI 7-10 days before
presentation
“Cola or tea” colored
urine
Periorbital
edema/HTN
ASO titer, Low serum
complement
Treat infection/HTN
Clinical Scenario
Patient with sinusitis,
rhinorrhea, bloody
nasal discharge and
cough, shortness of
breath, hemoptysis.
Hematuria, Proteinuria
and Renal Failure.
+ for c-ANCA
Most likely diagnosis?
Wegener’s granulomatosis
Confirm with biopsy of
nasopharyngeal lesion if
possible.
Alternative: renal biopsy
(crescentic necrotizing
GN). Focal or diffuse
necrotizing
extracapillary GN is
histological hallmark of
ANCA-associated
Vasculitis.
Tx: Corticosteroid and
Cyclophosphamide
Good Pasture Syndrome
Hemoptysis +
Hematuria
Proteinuria + Renal
Failure
Anti-GBM antibody!
Tx: Plasmapheresis +
Prednisone +
Cyclophosphamide
Lupus Nephritis
Type I: Minimal
Mesangial
Type II: Mesangial
Proliferative
Type III: Focal
Proliferative
Type IV: Diffuse
Proliferative
Type V: Membranous
Type VI: Advance
Sclerosis
Nephrotic Syndrome
Not enough albumin (Hypoalbuminemia)
Edema
Proteinuria > 3.5 gm/24 hours
Hyperlipidemia
Nephrotic Syndrome
Renal causes: Minimal Change Disease,
Membranous Nephropathy, FSGS
Systemic: SLE, Diabetes, Amyloidosis
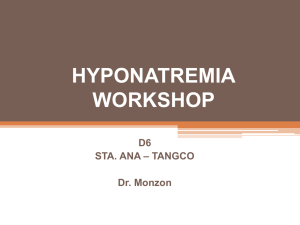
Minimal Change Disease
Electron Microscopy Normal vs. MCD
Normal Kidney
MCD: The individual foot processes
can no longer be made out- they
have all just “melted” together into
a single thin layer. Barrier in
filtration process can no longer
keep protein from being filtered out
of the blood and into urine.
Membranous Nephropathy
Most common cause of
Nephrotic syndrome in
adults.
Causes: idiopathic,
carcinoma, Hep B, Hep
C, SLE, Drugs:
Penicillamine,
Captopril, Gold
Treatment: Prednisone
Kidney Biopsy Review
DIFFUSE
When all or at least
more than 80% of the
glomeruli seen in the
biopsy is affected.
FOCAL
Only certain
proportion of the
glomeruli seen in the
biopsy involved.
Kidney Biopsy Review
GLOBAL
When the entire globe
of the glomerulus is
affected .
SEGMENTAL
Only a segment of
glomerulus involved.
Focal Segmental Glomerular Sclerosis
Most common cause of
Nephrotic syndrome in
black patients, obese
patients, IVDA, heroin
abuse, HIV.
Acid-Base Disturbances
Normal pH
7.4 = 40 nmol/L
24 X 40/24
H + = 24 X PCO2
(respiratory)/HCO3(metabolic)
pH < 7.4 is acidotic
Anion Gap
(Na+) – (Cl- +HCO3-)
MUDPILES
Methanol
Uremia
DKA
Paraldehyde/Propylene
glycol
INH/Iron
Lactic acidosis
Ethylene glycol
Salicylates
“My name is MUD!”
Normal anion gap (8-12 mEq/L)
Diarrhea
Glue sniffing
Renal tubular acidosis
Hyperchloremia
Metabolic Acidosis: Compensation
For every 1 mEq
HCO3- down, there is
1.3 mmHg PCO2
down
Increased ventilation,
blow off CO2
Metabolic Alkalosis
Vomiting (urine
chloride < 20)
Diuretic use (except
carbonic anhydrase
inhibitors): Ucl>20
Antacids/milk-alkali syndrome
Hyperaldosteronism
Bicarbonate addition
Loss of H+ from GI tract or
kidney
Loss of Chloride from GI tract
or kidney
Adaptation: 0.7 mm Hg
of PCO2 up for every
1mEq/L up of HCO3Decrease ventilation!
Respiratory Acidosis
Primary disturbance?
PCO2 Up
Acute causes:
Airway obstruction
Status asthmaticus
Alveolar defects
(pulmonary edema,
pneumonia)
CNS depression,
neuromuscular impairment
Ventilatory restriction (flail
chest with rib fractures)
Chronic causes: COPD,
abnormal chest wall
mechanics.
Compensation: Acute (for
any PCO2 up go 1-3
mEq/L up in HCO3-)
Chronic: For any 1 mm Hg
up in PCO2 go up 0.4
mEq/L in HCO3-)
Respiratory Alkalosis
Primary disturbance?
PCO2 down
Cause:
High altitude residence
Pregnancy, Pulmonary
disorder, CNS disease,
Aspirin intoxification
Hepatic failure, Sepsis
Anxiety
Hyperventilation
High Carbon Dioxide
Respiratory Acidosis
Metabolic Alkalosis
CO2
High
High (compensation)
pH
<7.4
>7.4
Low Carbon Dioxide
Respiratory Alkalosis
Metabolic acidosis
CO2
Low
Low (compensatory)
pH
>7.4
<7.4
High Bicarbonate
Metabolic Alkalosis
Respiratory acidosis
Bicarb
High
High (compensation)
pH
>7.4
<7.4
Low Bicarbonate
Metabolic acidosis
Respiratory alkalosis
Bicarb
Low
Low (compensation)
pH
<7.4
>7.4
Clinical Scenario: Aspirin Overdose
Causes two different
primary disturbances:
Respiratory Alkalosis
and Metabolic Acidosis
Look for co-existing
tinnitus, hypoglycemia,
vomiting, history of
“swallowing several
pills.”
Alkalinize urine with
Bicarbonate: speeds
excretion.
Imbalances of Sodium
Hypernatremia
Serum Na+ > 145
Causes: Diabetes
insipidus, dehydration.
Diabetes insipidus
Lab: Urine osmolality
less than serum.
How do you
differentiate between
central and
nephrogenic DI?
Vasopressin challenge:
Uosm increases in
central, minimal
change in nephrogenic.
Central vs. Nephrogenic DI
Central: Decreased
production of vasopressin
(trauma, neurosurgery,
idiopathic). Treatment:
intranasal DDAVP.
Nephrogenic: renal tubules
unresponsive to vasopressin
(Lithium, Demeclocycline,
hypokalemia,
hypercalcemia). Treat the
cause, thiazide or
amiloride.
Clinical Scenario
78 year old male from nursing home with altered
mental status, serum sodium 160. BUN/Cr high and
Uosm very high >800. Started DSW: after 10
hours the patient developed a seizure. What
happened?
Rapid correction of hypernatremia. In
hypernatremic patient: slow correction 0.5 mEq/L
per hour by free water or D5W (no more than 12
mEq/L over first 24 hours). Check serum sodium
every 2 hours!
Hyponatremia
Hypovolemia
Isovolemia
Hypervolemia
Diarrhea
Vomiting
Diuretics
SIADH
Hypothyroidism
Cortisol insufficiency
Polydipsia
Beer Potomania
CHF
Nephrotic syndrome
Cirrhosis
Hyponatremia
In True hyponatremia: Serum Osmolality should be
low.
Hyponatremia with normal plasma osmolality:
Pseudohyponatremia due to hyperlipidemia or
hyperproteinemia.
Hyponatremia with elevated plasma osmolality:
mannitol or hyperglycemia. For every 100 above 100
mg/dl of glucose > correct serum Na+ 1.6. Example: Plasma
glucose 400 and Serum Na+ 130 > corrected will be 134.8
Treatment of Hyponatremia
Asymptomatic: increase serum sodium 0.5 mEq/L
per hour (10-12 mEq/L per day).
Hypovolemia: Use Normal saline.
Hypervolemia, SIADH: FLUID RESTRICTION!
Symptomatic: Hypertonic saline, 1-2 mEq/L per
hour first 3-4 hr then 0.5-1 mEq/L per hour. No
more than 10-12 mEq/L per day in first 24 hours.
Rapid Correction of Hyponatremia
Central Pontine
Myelinolysis or
Osmotic Demyelination
Syndrome (flaccid
paralysis, dysarthria,
dysphagia).
Thank you for your attention!