Eutanázie
advertisement

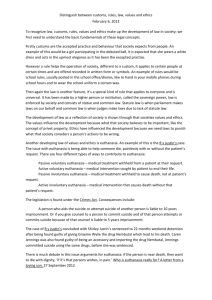
2011 Marek Vácha EUTHANASIA Euthanasia eu = good, right; thanatos = death "Passive euthanasia" = withdrawing (=stopping) medical treatment with the deliberate intention of causing the patient's death „Active euthanasia“ = A deliberate act to end another person's life on patient´s request the difference between "active" and "passive" is that in active euthanasia, something is done to end the patient's life; in passive euthanasia, something is not done that would have preserved the patient's life. there is difference between „letting die“ and „killing“ Euthanasia Euthanasia means knowingly and intentionally performing an act that is clearly intended to end another person´s life and that includes the following elements: the subject is a competent informed person with an incurable illness who has voluntarily asked for his or her life to be ended; the agent knows about the person´s condition and desire to die and commits the act with the primary intention of ending the life of that person the act is undertaken with compassion and without personal gain Assistence in Suicide Assistance in suicide means knowingly and intentionally providing a person with the knowledge or means or both required to commit suicide, including counseling about lethal doses of drugs, prescribing such lethal doses or supplying the drugs NAZI GERMANY 1939 - 1941 Karl Brandt Philipp Bouhler Nazi physician Karl Brandt, director of the Euthanasia Program. August 27, 1942. Program T4 1000 : 10 : 5 : 1 Tiergartenstraße 4 This image originates from a film produced by the Reich Propaganda Ministry. It is captioned: "A moral and religious conception of life demands the prevention of hereditarily ill offspring." Nazi propaganda aimed to create public support for the compulsory sterilization effort. Six places, where euthanasia were performed Brandenburg near Berlin (January 1940 - September 1940), Grafeneck near Stuttgart (January 1940 - December 1940), Hartheim near Linz in Austria (January 1940 - December 1944), Sonnenstein/Pirna near Dresden (April 1940 - August 1943), Bernburg near Magdeburg (September 1940 - April 1943), Hadamar near Koblenz (January 1941 - August 1941). Buses used to transport patients to Hadamar euthanasia center. The windows were painted to prevent people from seeing those inside. Germany, between May and September 1941. 1936 'This person suffering from hereditary defects costs the community 60,000 reichsmark during his lifetime. Fellow German, that is your money too.' Nazi poster bearing the phrase, translated from German, "A strong and healthy nurse is there only to give care to a dangerous madman. Shouldn't we be ashamed?" Clemens von Galen Lebensunwertes Leben ? “We must expect, therefore, that the poor defenceless patients are, sooner or later, going to be killed. Why? . . . because in the judgement of some official body, on the decision of some committee, they have become “unworthy to live", because they are classed as “unproductive members of the national community". The judgment is that they can no longer produce any goods: they are like an old piece of machinery which no longer works, like an old horse which has become incurably lame, like a cow which no longer gives any milk. What happens to an old piece of machinery? It is thrown on the scrap heap. What happens to a lame horse, an unproductive cow? I will not pursue the comparison to the end — so fearful is its appropriateness and its illuminating power . . . If it is once admitted that men have the right to kill “unproductive" fellowmen — even though it is at present applied only to poor and defenceless mentally ill patients — then the way is open for the murder of all unproductive men and women: the incurably ill, those disabled in industry or war. The way is open, indeed, for the murder of all of us, when we become old and infirm and therefore unproductive". “For some months we have been heating reports that inmates of establishments for the care of the mentally ill who have been ill for a long period and perhaps appear incurable have been forcibly removed from these establishments on orders from Berlin. Regularly the relatives receive soon afterwards an intimation that the patient is dead, that the patient's body has been cremated and that they can collect the ashes. There is a general suspicion, verging on certainty, that these numerous unexpected deaths of the mentally ill do not occur naturally but are intentionally brought about in accordance with the doctrine that it is legitimate to destroy a so-called “worthless life” — in other words to kill innocent men and women, if it is thought that their lives are of no further value to the people and the state. A terrible doctrine which seeks to justify the murder of innocent people, which legitimises the violent killing of disabled persons who are no longer capable of work, of cripples, the incurably ill and the aged and infirm!” I will give you an example of what is happening. One of the patients in Marienthal was a man of 55, a farmer from a country parish in the Münster region — I could give you his name — who has suffered for some years from mental disturbance and was therefore admitted to Marienthal hospital. He was not mentally ill in the full sense: he could receive visits and was always happy, when his relatives came to see him. Only a fortnight ago he was visited by his wife and one of his sons, a soldier on home leave from the front. The son is much attached to his father, and the parting was a sad one: no one can tell, whether the soldier will return and see his father again, since he may fall in battle for his country. The son, the soldier, will certainly never again see his father on earth, for he has since then been put on the list of the “unproductive”. A relative, who wanted to visit the father this week in Marienthal, was turned away with the information that the patient had been transferred elsewhere on the instructions of the Council of State for National Defence. No information could be given about where he had been sent, but the relatives would be informed within a few days. What information will they be given? The same as in other cases of the kind? That the man has died, that his body has been cremated, that the ashes will be handed over on payment of a fee? Then the soldier, risking his life in the field for his fellow-countrymen, will not see his father again on earth, because fellow-countrymen at home have killed him. Who could then have any confidence in a doctor? Then no man will be safe: some committee or other will be able to put him on the list of “unproductive” persons, who in their judgment have become “unworthy to live”. And there will be no police to protect him, no court to avenge his murder and bring his murderers to justice. Who could then have any confidence in a doctor? Tiergartenstraße 4 today Slippery slope Baby Knauer dětská "eutanázie" T4: "eutanázie" dospělých Auschwitz …after Auschwitz How can the progress of modern science and medicine and industry promise to liberate people from ignorance, disease, and brutal, mind-numbing work, yet help create a world where people willingly swallow fascist ideology, knowingly practice deliberate genocide, and energetically develop lethal weapons of mass destruction? Theodor Adorno EUTHANASIA (ALL OVER THE WORLD) 1973 - 2010 Euthanasia we are able to cope with a concrete illnesses... ...but we are unable to cope with aging Euthanasia The Netherlands, 1994 On April 10, 2001, the Dutch Parliament approved the "Termination of Life on Request and Assisted Suicide (Review Procedures) Act."(41) It amended sections of the criminal code, specifically stating that the offenses of euthanasia and assisted suicide are not punishable if they have been "committed by a physician who has met the requirements of due care" that are described in the act and if they have informed the municipal "autopsist" in accordance with the Burial and Cremation Act. Australia: 1995 – 1997 Oregon (AS) from 1998, Washington (AS) from 2008 Belgium from 2002 Luxembourg from 2008 Oregon from 1998 the patient must be a capable adult be an Oregon resident have a terminal illness, with less than six month to live (!!) voluntarily request a prescription for lethal drugs the request must be made both orally and in writing Countries where Euthanasia/AS are allowed Euthanasia „Dutch definition of euthanasia“ =the intentional termination of the life of a patient at his request by someone other than the patient Medische macht en medische ethiek Hippocratic oath the physician must preserve human life, save it and prolong it, where and whenever possible today, with all the medical possibilities: the physician must preserve human life, save it and prolong it, wherever it is sensible and meaningful to do so. should the physician consider it no longer sensible to proceed, then he should be permitted to end patient´s life. This can be done in two ways: through ceasing all life-sustaining measures through actively terminating the life of the patient Sohn, W., Zenz, M., (eds) (2001) Euthanasia in Europe. Schattauer. Stuttgart, New York. p.138 The Netherlands In 1973 Dr. Gertruida Postma, who gave her dying mother a lethal injection, received light sentence in the Netherlands. The case and its resulting controversy launched the euthanasia movement in that country. Postma Case Leeuwarden 1973 Dr. Postma was sentenced to only one week in prison this remarkably mild sentence was based on the fact, that the physician´s mother was incurably ill she experienced her suffering as unbearable she was already in dying phase the ending of life was done on her own expressed wish The Netherlands 1973 Voluntary Euthanasia societies formed in the Netherlands 1982 A Rotterdam court states conditions under which aiding suicide and administering Voluntary Euthanasia will not lead to prosecution in the Netherlands 1984 The Supreme Court of the Netherlands declares that V.E. is acceptable subject to ten clearly defined conditions 1990 Notification procedure agreed between the Royal Dutch Medical Association and the Ministry of Justice 1994 Amendments under the Burial Act incorporate the notification procedure, giving the latter formal legal status Rotterdam criteria: 1982 the patient makes a voluntary request the request must be well considered the wish for death is durable the patient is in unacceptable suffering the physician has consulted a colleague who agrees the proposed course of action The Netherlands The Penal Code of the Netherlands contains a variety of provisions prohibiting the intentional taking of human life. Two of these provisions specifically relate to physicianassisted suicide and active voluntary euthanasia: Article 293 of the Penal Code prohibits taking a person's life at that person's 'express and serious request'. This crime, sometimes described as 'the offence of voluntary euthanasia'(133), is punishable by imprisonment for a maximum of 12 years or by a fine. Article 294 of the Penal Code prohibits assisting suicide. Where a death by suicide has occurred, anyone who helped bring about that death could be prosecuted under article 294 for intentionally inciting another to commit suicide, assisting in the suicide of another, or procuring the means for another to commit suicide. Where a death has occurred, this crime is punishable by imprisonment for a maximum of 3 years or a fine. Netherland The most important reasons for the request for euthanasia were futile suffering (29%), avoidance of humiliation (24%) unbearable suffering (18%). Although pain was among the reasons in 40% of cases, only in 5% of cases was pain mentioned as the most important reason. Van der Wal G, van Eijk JThM, Leenen HJJ, Spreeuwenberg C. Euthanasia and assisted suicide. II. Do Dutch family doctors act prudently? Family Practice 1992;9:135-40. Remmelink Report Since 1984 the practice of euthanasia in Holland has been very open, and many claims have been made as to its frequency and its benefits or drawbacks. To establish the facts on euthanasia, a government-sponsored study was undertaken and the report released September 10, 1991. This report, Euthanasia and other Medical Decisions Concerning the End of Life, commonly called the Remmelink Report, has revealed disturbing findings. The population of the Netherlands in 1990 was 15 million. The study findings indicated the following annual figures: 2300 cases of active voluntary euthanasia. 400 cases of assisted suicide (the lethal means for death is provided to the patient for self-administration) 1040 cases of involuntary euthanasia (.8% of total deaths in Holland). These cases --averaging almost 3 per day -- were those in which the physician prescribed, provided or administered a medicine with the deliberate aim to hasten the end of life, though the patient had made no explicit request for euthanasia. Remmelink Report 14% of patients whose lives were ended without their explicit request were fully competent. 62% of patients whose lives were terminated without their explicit request had never given any indication regarding termination of life. An additional 8100 patients died after pain medication (morphine) was administered by physicians who intended to shorten life. The decision to administer the intentional overdose was not discussed with 27% of fully competent patients who died in this manner. Remmelink report: 1991 The Netherlands 1995 2000 2,2% - 2,3% 2,2% - 2,6% assisted 0,2% - 0,4% suicidium without explicite 0,7% request 0,1% - 0,2% Euthanasia 0,6% - 0,7% …without specific request… there is a difference between questions what would the patient want in this circumstances? what do you want for the patient? Netherland The most important reasons for the request for euthanasia were futile suffering (29%), avoidance of humiliation (24%) unbearable suffering (18%). Although pain was among the reasons in 40% of cases, only in 5% of cases was pain mentioned as the most important reason. Van der Wal G, van Eijk JThM, Leenen HJJ, Spreeuwenberg C. Euthanasia and assisted suicide. II. Do Dutch family doctors act prudently? Family Practice 1992;9:135-40. The Netherlands On April 1st 2002, euthanasia became legal in The Netherlands, rather than being technically illegal but not punishable in circumstances of ‘force majeure’ (necessity). Key points in the new law include the following: incompetent patients can be killed if they have written a statement in advance requesting euthanasia. teenagers aged 16-18 may receive euthanasia, not necessarily with the agreement of a parent or guardian. The Netherlands children 12-16 years old may receive euthanasia with the agreement of a parent or guardian. the doctor must hold the conviction that the patient’s suffering is lasting and unbearable. all cases will be reviewed after the death of the patient. the law does not prohibit doctors from administering euthanasia to nonresidents. The Netherlands 2002 in order for the physician to assist with the euthanasia, the following must occure the patirnt must request the assistance freely and frequently, after careful consideration the physician may act on the request only if the patient is terminally ill, with no hope of improvement and in severe pain the physician must consult with another physician and file a report with the coroner The Netherlands 2002 the standard process is to give a large dose of barbiturates to produce com and then an injection of curare, which stops respiration and heart rate The Netherlands 2002 types of patient availing themselves for euthanasia option: women and men are equal in requesting euthanasia the average age for men is sixty-three and for women sixty-six requests are rare in people over age seventyfive and even rarer for those over age eightyfive The Netherlands 2002 The Dutch Patient´s Association: „We feel our lives are threatened. We realize that we cost the community a lot. Many people think we are useless, often we notice that we are being talked into desiring death. We will find it extremely dangerous and frightening if the new medical legislation includes euthanasia.“ Oregon from 1998 the patient must be a capable adult be an Oregon resident have a terminal illness, with less than six month to live (!!) voluntarily request a prescription for lethal drugs the request must be made both orally and in writing Kevorkian case june 1990 – Janet Adkins ended her life with the assistance of Dr. Jack Kevorkian by the end of June 1998, Kevorkian had participated in over fifty similar events using his suicide machines Kevorkian Sentenced to Prison (1999) In 1999, pathologist Dr. Jack Kevorkian was sentenced to a 10-25 year prison term for giving a lethal injection to Thomas Youk whose death was shown on the 60 Minutes television program. in 2006 he was released Switzerland Suicide tourism In 2000 three foreigners committed suicide in Zurich. In 2001, the number of death tourists to Zurich rose to thirty-eight, plus twenty more in Bern. Most of the deaths occurred in an apartment rented by Dignitas, one of the four groups that have taken advantage of Switzerland's 1942 law on euthanasia to help the terminally ill die. Letting die = enabling nature to take its course but there is a difference between: withdrawing machines and medications from the patient withholding or withdrawing artificial nutrition and hydration A Question What is the difference between administering a large dose of morphine for reducing physical pain and using that same dosage in response to a person saying, „I want to end this“? An Answer the physical pain occurs against the will of the patient, and the morphine is therefore a therapeutic response the statement „I want to end this“ is, however, an expression of the individual´s will Pain organic emotional social spiritual (Cicely Saunders) Quality end of life care according to „ „The Committee on Care at the End of Life of the US Institute of Medicine, NationalAcademy of Sciences“ overall quality of life physical well-being and functioning psychosocial well-being and functioning spiritual well-being patient perception of care family well-being and perception „…tired of living“ Jurisprudence from 1994 states that the extent of the suffering is determined by the way in which it is experienced, and should be abstracted from the cause. However, jurisprudence from 2002 adds to this that the cause must be medical: if a patient is suffering from the consequences of old age and requests EAS because (s)he is ‘tired of living’, but does not suffer from a severe disease, the physician is not allowed to grant such a request „…tired of living“ One of the reasons for this, as given by the Supreme Court, is that a physician is a medical expert, and can therefore judge the extent of unbearable and hopeless suffering of a patient with a medically defined disease, but is not an expert in dealing with patients who are tired of living Arguments For Euthanasia It provides a way to relieve extreme pain It provides a way of relief when a person's quality of life is low Frees up medical funds to help other people It is another case of freedom of choice Arguments For Euthanasia There are two general arguments used in favour of legalised euthanasia and assisted suicide. One is the ending of unbearable physical and/or psychological suffering in the case of terminal illness, and the other is to enhance individual autonomy. Arguments for euthanasia Refused by a court in Dijon the right to die under medical supervision, she was found dead at home. According to prosecutors, she had taken a "deadly dose" of barbiturates. Chantal Sebire died March 19, 2008 Arguments Against Euthanasia: Euthanasia devalues human life Euthanasia can become a means of health care cost containment Physicians and other medical care people should not be involved in directly causing death There is a "slippery slope" effect that has occurred where euthanasia has been first been legalized for only the terminally ill and later laws are changed to allow it for other people or to be done non-voluntarily. Arguments Against Euthanasia: Increasingly, however, euthanasia activists have dropped references to terminal illness, replacing them with such phrases as: "hopelessly ill" "desperately ill" "incurably ill" "hopeless condition“ "meaningless life" Arguments Against Euthanasia: Immanuel Kant Kant offered the "formula of the end in itself" as: "Act in such a way that you treat humanity, whether in your own person or in the person of another, always at the same time as an end and never simply as a means." This places more emphasis on the unique value of human life as deserving of our ultimate moral respect and thus proposes a more personal view of morality. In application to particular cases, of course, it yields the same results: violating a perfect duty by making a false promise (or killing myself) would be to treat another person (or myself) merely as a means for getting money (or avoiding pain) Arguments against euthanasia Emotional and psychological pressures could become overpowering for depressed or dependent people. If the choice of euthanasia is considered as good as a decision to receive care, many people will feel guilty for not choosing death. Financial considerations, added to the concern about "being a burden," could serve as powerful forces that would lead a person to "choose" euthanasia or assisted suicide. Arguments against euthanasia permitting assisted suicide may at first look like an affirmation of the patient´s liberty, but it soon transforms into a duty to die protecting individuals´liberty is more effectively achieved by making assisted suicide a socially unacceptable option so the individuals need not defend their desire to continue living Arguments Against Euthanasia: Immanuel Kant Kant offered the "formula of the end in itself" as: "Act in such a way that you treat humanity, whether in your own person or in the person of another, always at the same time as an end and never simply as a means." This places more emphasis on the unique value of human life as deserving of our ultimate moral respect and thus proposes a more personal view of morality. In application to particular cases, of course, it yields the same results: violating a perfect duty by making a false promise (or killing myself) would be to treat another person (or myself) merely as a means for getting money (or avoiding pain) we should not be asking whether one may aid another in dying; we should rather explore what prompts people to seek to die in the first place and then we should remove those motivations through proper pain medication and through attentive care people asking for help in dying to overcome the loneliness and the futility of their lives should not be offered aid in dying but should rather be given assistance in making the remainder of life meaningful Remember… Competent patients have the right to refuse treatment, even when the refusal will result in disability or death. Dysthanasia USA: about half of all patients spent their last days in what the researches termed „an undesirable state“, including a week or so in an intensive care unit having a physician who was unaware of wishes not to be resuscitated being in serious, insufficiently treated pain the enthusiasm for physician-assisted suicide is driven, in part, by the fear that we will receive overly aggressive care at the end of life and that our suffering may be prolonged Euthanasia THE WORLD MEDICAL ASSOCIATION RESOLUTION ON EUTHANASIA Adopted by the WMA General Assembly, Washington 2002 May 2001 20.3/2001 Euthanasia „Euthanasia, that is the act of deliberately ending the life of a patient, even at the patient's own request or at the request of close relatives, is unethical. This does not prevent the physician from respecting the desire of a patient to allow the natural process of death to follow its course in the terminal phase of sickness." Euthanasia WMA , 1994: „Physicians-assisted suicide, like euthanasia, is unethical and must be condemned by the medical profession. Where the assistance of the physician is intentionally and deliberately directed at enabling an individual to end his or her own life, the physician acts unethically. However the right to decline medical treatment is a basic right of the patient and the physician does not act unethically even if respecting such a wish results in the death of the patient." Euthanasia BE IT RESOLVED that: 1. The World Medical Association reaffirms its strong belief that euthanasia is in conflict with basic ethical principles of medical practice, and Euthanasia The World Medical Association strongly encourages all National Medical Associations and physicians to refrain from participating in euthanasia, even if national law allows it or decriminalizes it under certain conditions. Physicians should not abandon dying patients but should continue to provide compassionate care even when cure is no longer possible Hippocratic Oath I will not give a lethal drug to anyone if I am asked, nor will I advise such a plan; First world conference on euthanasia: 2008 The first International Symposium on Euthanasia and Assisted Suicide held in Toronto Nov. 30-Dec. 1 2008 “I have experienced all the symptoms which they claim are symptoms for euthanasia,” Davis said. “If my country had had laws allowing euthanasia and assisted suicide when I was at my lowest point, I would be dead,” RELIGION PERSPECTIVES A Jewish Approach Jewish sources view all forms of active euthanasia and assisted suicide as forbidden acts of murder that is true even if the patient explicitly asks to be killed Pragmatism Judaism American school of Judaism requires us to pragmatism, its media and even its recent welfare legislation reforms would think of ourselves in utilitarian terms, with our worth being a function of what we can do for ourselves and others American attitudes and laws thus permit suicide, especially when a person can no longer do anything useful for either herself or himself or for others evaluate our lives in light of the ultimate value inherent in us because we were created in God´s image Jewish ideology and law therefore strongly oppose commiting suicide or assisting others in doing so, for life is sacred regardless of its quality or usefulness A Jewish Approach God created and therefore owns the entire universe, including each person´s body and we therefore do not have the right unnecessarily to destroy or dammage God´s property , including even God´s vegetation and inanimated property this obligation makes suicide an act of theft from God, a violation of God´s prerogatives, and the trespass of the proper boundaries between God and human beings (Dorff, E.N., (2003) Matters of Life and Death. A Jewish Approach to Modern Medical Ethics. The Jewish Publication Society, Philadelphia, PA, p. 179) A Jewish Approach Assisted Suicide the helper minimally inviolates Leviticus 19,14: „Do not put a stumbling block before the blind“ A Jewish Approach Even though Jewish law goes quite far in permitting terminally ill patients to die with whatever palliative care they need and without any other medical interference it does not permit suicide or assisted suicide the tradition maintains a firm line between legitimately withholding and withdrawing medical efforts on the one hand and illegitimately helping a person actively to take his or her life on the other A Jewish Approach the value of life does not depend on the level of one´s abilities it derives from the image of God embedded in us the tradition thus strongly affirms the divine quality of the life of disabled people the Jewish tradition requires that we recognize the divine aspect of people in the last stages of life, regardless of the quality of their lives Christianity The Role of Suffering: Down through the centuries and generations it has been seen that in suffering there is concealed a particular power that draws a person interiorly close to Christ, a special grace. Pope John Paul II: Salvifici Doloris, 1984 We should relieve suffering when we can, and be with those who suffer, helping them to bear their suffering, when we can't. We should never deal with the problem of suffering by eliminating those who suffer. around 1470