Presenting a medical topic to colleagues
advertisement

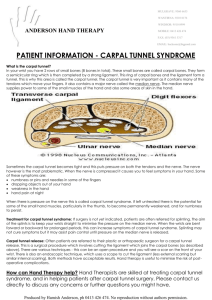
Presenting a medical topic to colleagues Wim Willems Craiova, September 2011 Program • Who is everybody? • What makes a medical presentation good / what makes it bad? • A medical program: carpal tunnel syndrome • Rules & take home messages What makes a training good / bad? • Tell your colleagues about a training / seminar that was really bad and didn’t teach you anything. Why was it bad? • Tell your colleagues about a training / seminar that was really good and educational. Why was it good? Rule 1 – avoid boredom Rules to avoid boredom • Keep it small • Start with the needs of the group • Use the knowledge that the group has already • Be interactive (little groups, avoid monologue) • Change methods (presentation, quiz, case history, discussion regarding statements, skills) Rules to avoid boredom • Keep it small • Start with the needs of the group • Use the knowledge that the group has already • Be interactive (little groups, avoid monologue) • Change methods (presentation, quiz, case history, discussion of statements, skills) Keep it small Carpal tunnel syndrome Start with the needs of the group • What do you want to know? What do Dutch GP’s want to know? • Is it necessary to perform an EMG to establish the diagnosis CTS ? • Is it necessary to have positive tests like Tinel, Phalen etcetera ? • Are injections with corticosteroids helpful ? • Can I give an injection with corticosteroids myself ? What dosage should I give? How can I do this safely ? How often can I do this ? Quiz 1 • Mrs A, 53 years old, complains of nightly tingling in her right hand which wakes her up. When you examine her you find nothing abnormal. The tests of Tinel and Phalen are negative. Mrs A has no carpal tunnel syndrome Correct / Incorrect Quiz 2 • Mrs A, 53 years old, complains of nightly tingling in her right hand which wakes her up. You refer her for an EMG: this is negative (no nerve conduction abnormality). Mrs A has no carpal tunnel syndrome Correct / Incorrect Quiz 3 Where is the carpal tunnel ? “Painful nightly tingling” • Female, 52 years • Wakes up in the early morning with painful tingling in the hand (thumb / index) • Flapping of hand eases complaints Carpal tunnel syndrome • • • Female, 52 years Wakes up in the early morning with painful tingling in the hand (thumb / index) Flapping of hand eases complaints What do you do in Romania? Carpal tunnel syndrome Epidemiology Open population (history + nerve conduction examination): – Female: 9 % – Male: 0,6% – Peak between 40-60 year Risk factors Weight Pregnancy Diabetes mellitus Hypo/hyperthyreoidy Ovariectomy Anatomic deviation (traumatic / RA / congenital) Work related Natural course • ¼ - 1/3 significant improvement > 1 year • After pregnancy 50% without complaints Pathofysiology • Narrow tunnel • compression n. medianus in carpal tunnel • 90% idiopatic Diagnosis = history ! Dutch consensus (CBO 2006) / guideline NHG 2009: • • • • • • Nightly tingling Median nerve area Sleep disturbance Other tingling / pains Flapping (Flick sign) Advanced stages: tingling during the day Sensory innervation N. Medianus Atypical localisations tingling sensations • Often outside median nerve area • Sometimes ulnar nerve area Provocation tests: CBO 2006 / NHG 2009: Limited usefulness Diagnostic tests CTS test sensitivity specificity Tinel 0.25-0.60 0.64-0.89 Phalen 0.10-0.91 0.33-0.86 Flick sign 0.93 0.96 Square wrist sign 0.47-0.69 0.73-0.83 Pressure provocation test 0.28-0.63 0.33-0.74 Tourniquet test 0.21-0.51 0.36-0.87 Tests • Tinel: percussion median nerve • Phalen: flexion during 60 seconds • Further: -sensory loss median nerve area -thenar dystrophy -dry skin (thumb / index / middle finger) Neurophysiological examination • Verification of clinical diagnosis prior to operation EMG sensitivity specificity 60-82 95-100% Limitation EMG: • No golden standard • 10-15% false negative • No relation between complaints and results • Results not predictive for therapy • Value unclear for primary health care Treatment Splint • Day and night • Short term effective • Minor complaints / recent onset Surgery: • Highly effective • Major / recurrent complaints. Patient’s wish • Open / endoscopic • Success: 75-90% • Complications: damage to nerve, pain, scar, complex regional pain syndrome) Corticosteroid injection • Short term effectiveness + • 50% without complaints after one year • Diagnostic use? Referral • Insufficient reaction to symptomatic treatment (2 injectons) • Common sense • Diagnostic uncertainty • Severe complaints Corticosteroid injection • • • • Several techniques Safe Effective Tradition / experience / authority determines technique Medicament / Dosage • Most common: Triamcinolonacetonide 10 mg/ml (Kenacort® A10), or methylprednisolonacetaae (Depo-Medrol®) 40 mg/ml • Volume: 1-2ml • Interval between injections: 1-3 weeks • Effectiveness: 1st injection 80%, after 2 injections 15%, after 3 injections 5% Needle? -orange/ light brown (0,45x23mm) -light blue (0,5x25mm) -green (0,8x40mm) Localisation carpal tunnel Os pisiforme Os scaphoideum m. Palmaris longus Tendon m. Palmaris longus • Absent tendon: ulnar to median axis Localisation insertion • 3 ulnar to tendon m. palmaris longus 3-4 cm before distal wrist line Injection underneath retinaculum • Angle 30 degrees Hygiene • Wash hands, wear gloves or disinfect fingers • Once-only ampoules • Change needles • Disinfect skin Side effects and complications • Side effects -flushing: 1 day after injection -steroid-flare 24-48 hours -menstruation problems -hyperglycemia -locale effects: redness, atrophy fatty tissue, hypopigmentation • Complications -very rare, case-reports -tendon ruptures, median neuritis (CTS), local infection Take home messages • Organize and prepare your own training for yourself and for your colleagues • Keep it small • Try to answer only questions that have immediate consequences for your everyday practice • Do it yourself – specialists can tell you only what is important to them Take home messages • Organize and prepare your own training for yourself and for your colleagues • Keep it small • Try to answer only questions that have immediate consequences for your everyday practice • Do it yourself – specialists can tell you only what is important to them Take home messages • Organize and prepare your own training for yourself and for your colleagues • Keep it small • Try to answer only questions that have immediate consequences for your everyday practice • Do it yourself – specialists can tell you only what is important to them Take home messages • Organize and prepare your own training for yourself and for your colleagues • Keep it small • Try to answer only questions that have immediate consequences for your everyday practice • Do it yourself – specialists can tell you only what is important to them Take home messages • Organize and prepare your own training for yourself and for your colleagues • Keep it small • Try to answer only questions that have immediate consequences for your everyday practice • Do it yourself – specialists can tell you only what is important to them Material • www.hovumc.nl/gp • www.nice.org.uk • www.cks.nhs.uk/home Did you see this? Did it work? • Keep it small • Start with the needs of the group • Use the knowledge that the group has already • Be interactive (little groups, avoid monologue) • Change methods (presentation, quiz, case history, discussion regarding statements, skills) Va Mulţumesc, la revedere