Respiratory-Anatomy-by-Radiology-Sept
advertisement

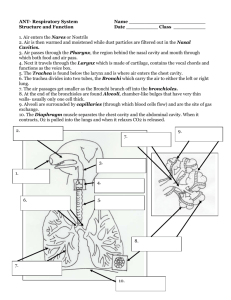
Respiratory Module Anatomy by Radiology • Welcome to this PowerPoint presentation on anatomy seen radiologically. • There are normal and abnormal views of the nasal cavity and sinuses, and of the thorax. • Plain X-ray, CT and MRI have been used. • Study the images and answer the questions before moving to answers on the next slide (your learning and retention will be much better). • Always cross-reference and integrate with other learning experiences and resources (Phase I lectures and the “Read After” anatomy guide). Nasal Cavity and Sinuses This CT is like studying a parasagittal section of a head in the Dissecting Room, but the sinuses are visible. Frontal Ethmoid Sphenoid Middle concha Inferior concha Nasal Cavity and Sinuses • Where do the sinuses open? • What opens into the inferior meatus? Frontal Ethmoid Sphenoid Middle concha Inferior concha Nasal Cavity and Sinuses • The sphenoid sinus opens into the spheno-ethmoidal recess above the superior meatus. The frontal, ethmoidal and maxillary open into the middle meatus. • The nasolacrimal duct drains lacrimal fluid from the conjunctival sac to the inferior meatus of the nasal cavity. • Look at the next two slides showing horizontal sections of the maxillary, and then ethmoid sinuses, just to appreciate their relationships to each other and to the nasal cavity. Nasal septum Maxillary sinus Ethmoid air cells Sphenoid air cells Mastoid air cells Nasal Cavity and Sinuses • Note the close proximity of the orbits, and the brain in the cranial cavity, to the nasal cavity. • To what do the arrows point? Brain ? Orbit ? ? ? ? Nasal Cavity and Sinuses Brain Ethmoid Sinus Middle Concha Orbit Maxillary Sinus Septum Inferior Concha Nasal Cavity and Sinuses • The nasal conchae create a large surface for carrying out nasal function. • But the nasal passages are narrow and easily obstructed. Position of Maxillary Sinus Opening Nasal Cavity and Sinuses • The nasal cavity and sinuses are lined by a vascular mucous membrane with pseudostratified, ciliated, columnar epithelial cells to slow, warm, filter and humidify the inhaled air. • Ciliary action empties the sinuses. • The maxillary sinus opening is high in the medial wall of the sinus and anything affecting the ciliary action, or narrowing the passageways may prevent proper emptying. Sinusitis • The right maxillary and ethmoid sinuses are obstructed. • The frontal sinuses are enlarged. Frontal Maxillary Sinusitis • Thickened mucous membrane in maxillary sinuses. • Deviated septum. Septum Thorax Cross Section Identify the numbers 1 to 10 1 2 10 9 3 8 7 4 6 5 1 Ascending aorta; 2 Pulmonary trunk (artery); 3 Left PA; 4 Left bronchus; 5 Descending aorta; 6 Oesophagus; 7 Azygos vein; 8 Right bronchus; 9 Right PA; 10 Superior vena cava. 1 2 10 9 3 8 4 7 6 5 Thorax • This is a contrast enhanced CT. As the injection is intravenous, the SVC is brighter. • Identify 1, 2 and the arrows. • You are looking from the feet upwards. Sternum ? ? 1 2 Vertebra Thorax • 1 is trachea, 2 is oesophagus. • What vertebral level is this? SVC Aortic Arch 1 2 2 Thorax • The aortic arch is in the superior mediastinum opposite T4. • The white spots in the lungs are contrast in pulmonary vessels that are cut in section as they radiate into the lungs. • What would be visible at a higher and at a lower level? Thorax T3 The trachea and oesophagus are still visible. The left and right brachiocephalic veins join to form the SVC. The aortic arch has given the brachiocephalic trunk (1), left common carotid, with vagus just lateral (2) and left subclavian (3) SVC 1 2 3 T3 Thorax T4/5 • • • • 1 and 2: Ascending and descending aorta. 3: Tracheal bifurcation. 4: SVC. What lies behind the bifurcating trachea? 1 4 3 2 Thorax T4/5 • The oesophagus on the left with the azygos vein just to the right of it. The vein can be followed to the SVC. 5 is the pulmonary trunk. 1 4 5 3 2 Azygos vein Oesophagus Thorax T5/6 1, 2 and 4 are as before but 3 is now the left main bronchus. Look at 5, the pulmonary artery dividing. Remember for next slide! Left pulmonary artery 1 5 Right pulmonary artery Oesophagus 4 3 2 Azygos vein Thorax Pulmonary Embolus Compare this slide and the previous one. Note the “filling defects” in the contrast at the bifurcation of the pulmonary artery and at the bifurcation of the left pulmonary artery: thrombotic emboli. What is the likely site of origin of the thrombus, and its route to the lung? What is visible posteriorly? Asc. Ao. Embolus in PA SVC Embolus in left PA Right bronchus Left bronchus ? Thorax Pulmonary Embolus • The thrombus originated in a deep vein in the lower limb, e.g. the posterior tibial. • It then moved to: popliteal, femoral, external iliac, common iliac, inferior vena cava, right atrium, right ventricle, pulmonary trunk (artery) and left pulmonary artery. • Posteriorly on the left, there is a little lung consolidation and pleural effusion following the embolus. • The next slide is a case presentation: Male (63) CT Pulmonary Angiogram after acute massive pulmonary embolus. Occluded Rt. main P. artery (arrow) and filling defect Lt. P. artery (arrow). Presented with: acute dyspnoea, hypoxia, low BP, acute Rt. heart strain on ECG No clot seen in IVC or iliofemoral veins on CT Abdo/Pelvis Negative coagulopathy and auto-antibody screens. Treated with thrombolysis and low molecular weight heparin, then warfarin. Thorax Heart at T 7 or 8 Identify the 4 chambers of the heart seen here in cross-section. ? ? ? ? Thorax Heart at T 7 or 8 Right ventricle Right atrium Left ventricle Left atrium Normal Chest Radiograph 1 Clavicle 2 Trachea, centrally positioned 3 Heart shadow 4 Vertebral column 5 Gas in fundus of stomach Note that the lung vascular markings fill the thoracic cavity 1 2 3 4 5 Right Pneumothorax The arrows point to the edge of the right lung. There is air outside it, within the pleural cavity. The edge is barely visible, but there are no vascular markings lateral to the arrows. The trachea is still central but may shift away from the side of the lesion in a tension pneumothorax. Here is another, very obvious right-sided pneumothorax, note how the lung markings stop and the right lung only fills about half of the right thoracic cage. Lung Tumour The arrow indicates a mass near the left lung hilum. Why might this condition present with hoarseness of the voice? Lung Tumour • The mass is seen here, compressing the left pulmonary artery. • The mass could compress the left vagus or recurrent laryngeal nerve. A Rarity! Look for the expected aortic knuckle (arch) on the left. It is not there. The arrow shows this patient has a right-sided aortic arch. Tumour, ball valve affect The arrow shows a tumour compressing the left main bronchus. It acts like a valve allowing air in but not out, as would an inhaled foreign body in the bronchus. Consequently the left lung is hyperinflated. It looks more radiolucent than the right lung and the vascular markings are reduced. Pneumonia The arrow shows the consolidation of pneumonia. 1 is the upper part of the right lobe of the liver, bulging upward under the diaphragm. 1 The End Those 34 slides complete the radiological revue of the anatomy of the Respiratory System and Thorax. A knowledge of topographical and surface anatomy is essential to understand the images. This presentation was created with the support and guidance of Dr Tom Taylor, consultant radiologist, Ninewells Hospital, who provided the radiographic images.