PowerPoint
advertisement

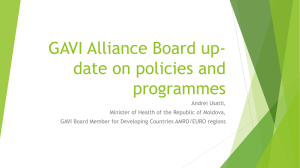
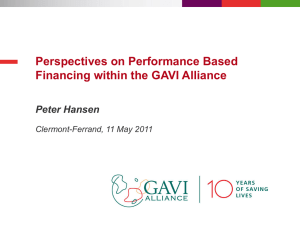
Critical conversations in Public-private partnerships Dr Ranjana Kumar 1st November 2007 The GAVI Alliance Public-private partnership bringing together all the major stakeholders in immunization Launched in 2000 Mission: Save children’s lives and protect people’s health by increasing access to immunization in poor countries Vaccines and funding to strengthen immunization and health services to 70+ of the poorest countries 2 GAVI partners Outline of innovations Raising resources – International Financing Facility for Immunisation, IFFIm Making vaccines available – Advance Market Commitment, AMC Facilitating introduction of new vaccines, ADIPs Supporting policy and programme implementation, Civil Society Organisation partnerships Programme level impact Funding innovations IFFIm: International Finance Facility for Immunisation: using markets differently – a radical shift in scale – US$ 1 billion frontloaded from the capital markets AMC: Advance market commitment pilot for pneumoccocal vaccine: accelerating access PPP example: Immunization Services Support (ISS) Background and Objectives Partner Contribution Public Sector Funds managed by governments Performance-based and time limited funding for developing countries to improve their health outcomes (i.e. increased vaccination coverage) ISS money is highly flexible to use; governments and its development partners make local decisions on most effective allocation and use of ISS funds to strengthen their health systems Additional funding or performance payments are given to countries when they have met or surpassed their self set immunization goals after the investment phase (almost similar to sales representatives receiving a commission bonus after having met their targets) Public and Social Sector Implementation: Delivery of immunization service in local hospitals or health centres run by local NGOs Success factors Monetary resources Incentivisation principals Economically minded and committed governments Rigorous control instance (e.g. independent audit of immunization coverage data to ensure system integrity) Private Sector Expertise: e.g. business based funding approaches Social Sector Advise: The WHO and UNICEF (renewable partner in GAVI Alliance Board) e.g. supported the Ministry of Health of Cambodia with the application process for ISS funds Implementation: UNICEF is managing the transfer of ISS funds Lessons learnt New performance based approaches (e.g. performance based funding) in development significantly increase its efficiency positively affects people’s commitment through increased selfdetermination Results: Speeding availability GAVI was designed to reduce the time lag in the availability of vaccines between industrialised and developing countries 200 HepB - all developing countries Millions of doses 150 GAVI established Hep B licensed 100 HepB combos licensed 50 HepB containing combination vaccines 0 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 Results: influencing the market Vaccine prices drop as new manufacturers enter the market DPT Hep B vaccines prices have declined by 40% The growing role of the developing country vaccine manufacturer Presence of multiple suppliers in the market is critical to vaccine security. In 2006, almost 30% of all the vaccines purchased by UNICEF for GAVI were manufactured in developing countries. Results to date Health services Additional children reached Hepatitis B: 126 million Hib: 20 million Yellow fever: 17 million DTP3: 28 million Dramatic immunisation coverage increase DPT3: 63% in 1999 to 77% in 2006 44% in 1999 to a 73% in 2006 in Africa Safe (auto-disable) syringes uptake 1.2 billion syringes Progress to date Estimated additional children reached with GAVI support (cumulative 200106) Hepatitis B: 126 million Hib: 20 million DTP3: 28 million Yellow Fever: 17 million • 1.7 million cumulative deaths already averted • It is projected that, by end 2006, more than 2.3 million future deaths will have been prevented (600,000 in 2006 alone). GAVI prospects and priorities • A long-term vaccine investment strategy • Ensuring effective implementation of scaled up resources • Build on the PPP model and strengthened CSOs participation in GAVI policy-making and programme implementation • Linking GAVI in with developments in international health architecture and in particular health systems work • Maintaining GAVI’s position as a leading innovative Global Health Partnership External validation of the GAVI Alliance business model “The economic impact and benefits of immunisation have been greatly underestimated; GAVI programmes could earn a rate of return of 18 percent” David Bloom, David Canning and Mark Weston (Harvard School of Public Health) “The Value of Vaccination”, World Economics, September 2005 “This is the first time that there is hard evidence that one of the major global health programmes is having a real impact.” "Independent Evaluation of the Impact of GAVI on DTP3 Coverage,” Murray et al. The Lancet, 18 September, 2006