Rapid, Repeated FISH in Human Amniocytes and Fibroblasts for
advertisement

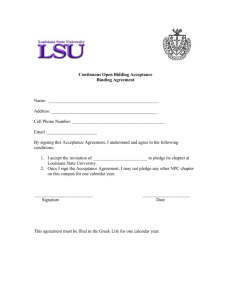
Effective ACT-based interventions with chronic illness patients: Achievable with online self-management programs? Matthew Maley, M.A., Abbie Beacham, Ph.D., John Forrette, M.A. Xavier University, Cincinnati, OH INTRODUCTION Figure 1. Percent of sample endorsing specific CI diagnoses RESULTS Those who expressed interest in sessions reported greater numbers of diagnosed CIs [Yes (mean = 2.47) versus No (mean = 1.95); p<.001]. Chronic medical illness (CI) is the leading cause of death in the world, accounting for 63% of mortalities in 2008, and nearly 80% of deaths in lower SES groups [11]. CIs also cause significant strain economically, accounting for varying proportions of GDP from country to country [11]. Health behaviors are often considered independent risk factors for many of the most common and costly CIs. Specific behavior change targets include: tobacco use, unhealthy diet, insufficient physical activity, and unhealthy alcohol use [11]. Behavior change interventions contribute to management of these conditions. One particular area psychologists may be able to intervene to improve health outcomes is in improving psychological flexibility in these populations. ACT-based interventions can be used to improve psychological flexibility, which has been linked to improved health outcomes [6]. These interventions have demonstrated efficacy with several CI populations and can impact medical conditions as well as behaviorally linked risk factors [10] including diabetes [7], epilepsy, weight loss, and chronic pain [9]. Despite the efficacy, effectiveness, and promise of ACT interventions, one of the most challenging barriers to successful intervention is generating interest in, and adherence to, behavioral CI management programs. The current study was an investigation of level of interest for CI management programs and potential modalities for program delivery. Additionally, differences in ACT related measures between interest groups were examined. Those who expressed interest in programming (“Yes”) endorsed: • Lower levels of mindfulness [Yes (mean = 4.09) versus No (mean = 4.36); p=.028] • Lower CI Acceptance-activity engagement [Yes (mean = 35.05] versus No (mean = 39.02); p=.013) and CI Acceptance-willingness Yes [(mean = 24.81) versus No (mean = 28.51); p=.021] • Higher experiential avoidance [Yes (mean = 20.65) versus No (mean = 17,95]; p =.003] Contrary to original hypotheses, when those who preferred programming on the internet were compared to all others, there were no differences in experiential avoidance, CI acceptance or mindfulness scores. Figure 2. “If chronic illness management sessions were available, would you be interested in participating in them?” METHOD Study participants (N=577) were recruited from online CI support groups and completed self-report measures as part of a larger survey study. The sample (mean age=53.02, SD=12.37) was primarily Caucasian (86.1%), female (80.2%), married (54.9%), and well educated (mean years=15.36, SD=2.74). Mean number of chronic illnesses was 2.36 (SD=1.39). CI diagnoses endorsed by study participants are presented in Figure 1. Measures: Program interest items Participants were asked to complete the following items regarding CI behavioral management programming: - “If chronic illness management sessions were available, would you be interested in participating in them?” - “If you attended these sessions, where would you most like to attend them?” Mindful Attention and Awareness Scale (MAAS) [3] The MAAS consists of 15 items designed to measure of a single-factor construct of mindfulness [3]. Each of the items is rated on a 6-point scale from 1 (“almost always”) to 6 (“almost never”). Chronic Illness Acceptance Questionnaire (CIAQ) [1] The CIAQ was adapted from the Chronic Pain Acceptance Questionnaire (CPAQ; McCracken et al., 2004). Twenty items are rated on a 0 (“Never true”) to 6 (“Always true”) scale to produce a two-factor structure: Activity Engagement and Pain Willingness. All CPAQ items were retained in the development of the CIAQ, and analyses revealed item loadings on the same two-factor structure as the CPAQ Acceptance and Action Questionnaire-II (AAQ-II) [2] The AAQ-II is a shortened, seven-item measure of psychological inflexibility and experiential avoidance designed to measure the same constructs as the Acceptance and Action Questionnaire (AAQ; Hayes et al., 2004). Items are rated from 1 (“never true”) to 7 (“always true”) scale for statements like “Emotions cause problems in my life.” “Yes” = 77.7% DISCUSSION The study results support the desirability of behavioral programming in persons with one or more CIs. In this sample, online CI self-management programs were the most appealing mode of delivery. There were no characteristic differences in ACT-related variables between those who preferred internet versus all others was contrary to our hypotheses that those who preferred internet programs would be higher in experiential avoidance than those who preferred to attend face-to-face programs in a physical space. Online interventions have been successful in changing several health and safety behaviors [5]. These mediums may be an effective mode of intervention for those who struggle to manage their CI and related symptoms, who may not otherwise seek treatment. Online intervention modalities may be considered either a first step in treatment engagement or an adjunct to face-to-face intervention. By increasing the likelihood of individuals receiving treatment through online modalities, outcomes may be improved. The willingness to engage in treatment via online intervention may be considered an avenue of through which psychological flexibility is enhanced. Several studies have investigated, or are investigating the effectiveness of online or smartphone delivered ACT-based interventions [4, 8]. Figure 3. “If you attended these sessions, where would you most Like to attend them?” REFERENCES [1] Beacham, A.O., Linfield, K., Kinman, C.R. & Payne-Murphy, J. (Revision under review) The Chronic Illness Acceptance Questionnaire: Confirmatory Factor Analysis and Prediction of Perceived Disability in an Online Chronic Illness Support Group Sample. Journal of Contextual and Behavioral Science. [2] Bond, F. W., Hayes, S. C., Baer, R. A., Carpenter, K. M., Guenole, N., Orcutt, H. K., Waltz, T., & Zettle, R. D. (2011). Preliminary psychometric properties of the Acceptance and Action Questionnaire – II: A revised measure of psychological flexibility and acceptance. Behavior Therapy, 42, 676-688. [3] Brown, K. W. & Ryan, R. M. (2003). The benefits of being present: Mindfulness and its role in psychological well being. Journal of Personality and Social Psychology, 84 (4), 822-848. [4] Fledderus, M., Bohlmeijer, E. T., Fox, J. P., Schreurs, K. M. G., & Spinhoven, P. (2013). The role of psychological flexibility in a self-help acceptance and commitment therapy intervention for psychological distress in a randomized controlled trial. Behaviour Research and Therapy, 51, 142-151. [5] Hieftje, K., Edelman, J., Carmenga, D. R., & Fiellin, L. E. (2013). Electronic media-based health interventions promoting behavior change in youth. The Journal of the American Medical Association Pediatrics,167 (6), 574-580. [6] Kashdan, T. B. (2010). Psychological flexibility as a fundamental aspect of health. Clinical Psychological Review, 30 (7), 865-878. [7] Gregg, J. A., Callaghan, G. M., Hayes, S. C., & Glenn-Lawson, J. L. (2007). Improving diabetes self-management through acceptance, mindfulness, and values: A randomized controlled trial. Journal of Counseling and Clinical Psychology, 75 (2), 336-343. [8] Lappalainen, R. Sairanen, E., Järvelä, E., Rantala, S., Korpela, R., Puttonen, S., … & Kolehmainen, M. (2014). The effectiveness and applicability of different lifestyle interventions for enhancing wellbeing: The study design for a randomized controlled trial for persons with metabolic syndrome risk factors and psychological distress. BMC Public Health, 14 (310), 1-16. [9] Lundgren, T., Dahl, J., Melin, L., & Kies, B. (2006). Evaluation of acceptance and commitment therapy for drug refractory epilepsy: A randomized controlled trial in South Africa – A pilot study. Epilepsia, 47 (12), 2173-2179. [10] Prevedini, A. B., Presti, G., Rabitti, E., Miselli, G., & Moderato, P. (2011). Acceptance and commitment therapy (ACT): The foundation of the therapeutic model and an overview of its contribution to the treatment of patients with chronic physical diseases. Giornale Italiano di Mediciana del Lavora ed Ergonomia, 33 (1), A53-A63. [11] World Health Organization (2011). Global status report on noncommunicable diseases 2010. Geneva, Switzerland: World Health Organization.