Open
advertisement

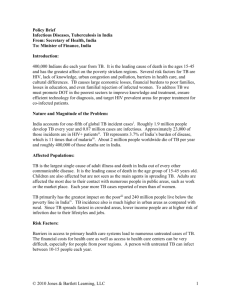
HIV Surveillance Case Definition Position Statement #12-ID-05 Overview CSTE Meeting June 3, 2012 Omaha, Nebraska Eve D. Mokotoff Proposed Revisions New HIV testing algorithms New: criteria for a suspect case HIV-2 infection Stage 0 HIV infection AIDS-defining conditions (opportunistic illnesses) CD4 test results for staging for adults/adolescents HIV Case definition for children Physician-documented diagnosis- PDD (clinical , rather than laboratory criteria for a confirmed case) PDD - date of diagnosis Proposed Revisions New HIV testing algorithms New: criteria for a suspect case HIV-2 infection Stage 0 HIV infection AIDS-defining conditions (opportunistic illnesses) CD4 test results for staging for adults/adolescents HIV Case definition for children Physician-documented diagnosis- PDD (clinical , rather than laboratory criteria for a confirmed case) PDD - date of diagnosis New HIV Testing Algorithms (slide 1) HIV cases should include persons with positive conclusions from any testing algorithm recommended by Criteria for Laboratory Testing and Diagnosis of Human Immunodeficiency Virus Infection: Approved Guideline, [CLSI document M53A, ISBN 1-56238-758-8], published June 2011 by Clinical and Laboratory Standards Institute Cases based on a presumptive positive result of a CLSI algorithm should not be distinguished from cases based on a definitive result in surveillance tabulations Why are we Suggesting this Change? The CLSI document describes algorithms that clinicians and labs are already using We are making these changes so we can have the infrastructure in place to allow reporting of cases diagnosed using these new algorithms We are not driving clinical practice- we are adapting surveillance to account for changes that are occurring Why are we Suggesting this Change? (cont) If we fail to develop a way to recognize cases diagnosed using the new algorithms we will undercount cases as use of the new algorithms increases the number of cases we would lose increases Implementation is complex but necessary Progression of HIV Viral Markers IgG IgM Acute Das G et al. BMJ 2010;341:bmj.c4583 Seroconversion→Established 7 New HIV Testing Algorithms (slide 2) What is new about the new algorithms? Results of more sensitive and specific antibody tests formerly used only as initial tests for screening (e.g., immunoassays such as EIAs and rapid tests) may now be used as supplemental tests to confirm a case of HIV-infection after a positive result on another immunoassay Relative Sensitivity of Tests From: Branson, JAIDS, 2010, 55 (S2): S102-S105 9 New Testing Algorithms (slide 3) Labs and healthcare providers may need guidance on how to report results from new multi-test algorithms to surveillance programs. Labs may need to report results of both first and subsequent test(s) in algorithm, not just final test Surveillance needs way to know both tests were part of same algorithm, not just unrelated screening tests We expect implementation issues to be resolved by a workgroup that consists of representatives from areas with established lab reporting systems and CDC staff. Proposed Revisions New HIV testing algorithms New: criteria for a suspect case HIV-2 infection Stage 0 HIV infection AIDS-defining conditions (opportunistic illnesses) CD4 test results for staging for adults/adolescents HIV Case definition for children Physician-documented diagnosis- PDD (clinical , rather than laboratory criteria for a confirmed case) PDD - date of diagnosis Suspect Case Criteria Cases meeting the following criteria should be reported for follow-up and confirmation: 4th gen IA positive (Ag/Ab test) F/U antibody-only test is negative NAT (normally used to confirm results above) is unavailable Conclusion - case may be antigen positive/ antibody negative Suspect Case - Rationale Cases meeting criteria may represent acute HIV infection Highly infectious - high viral loads May not know their HIV status High priority for follow-up by health department to obtain second specimen for NAT testing (if possible), notify of potential infectiousness, start partner notification process, refer into care for further testing and follow-up Suspect Case - Concerns Cases meeting criteria may be false positives Sensitivity and specificity of 4th generation IA is >99% (higher than the Western Blot we have been using to confirm cases as positive since the 1980s) so do not expect many false positives If case is falsely positive sending health department out to obtain second specimen for NAT testing/refer patient to care for follow up testing will determine status If HD unable to obtain NAT results, case can be changed to negative if received in the future Suspect Case – Concerns (cont) Are we expecting states to start routine collection of negative results? NO We do not want nor expect all negative results to be reported BUT if the 4th gen IA was + we would want negative results on antibody tests associated with that + reported if possible We expect we will learn of these cases primarily from reports from clinicians who encounter them Will know more as use of new lab tests increases Suspect Case – Concerns (cont) Inclusion of these cases in the case definition is to: help states emphasize the importance of such cases and give them the support to be able to report them Inclusion of these cases is not required Suspect Case - Steps Needed to Include in Position Statement Not included in PS#12-ID-05 as submitted on March 29, 2012 Is included in June 1 version of the Position Statement (posted on CSTE website) Addition is in section VII- Case Definition for Case Classification A.3 and A.3.a and Table VII-B.3 Suspect Case - Why Now? Work groups and consultation on integrating new testing algorithms occurred before testing using new algorithms widely implemented Once implementation began we realized that commercial labs would likely require a second blood draw with specimen received within 72 hours for confirmatory NAT testing Lab reality: second draws occur infrequently and/or specimens not received within 72 hours Consequently, need a process for cases described above and shown again in next slide Suspect Case Criteria Cases meeting the following criteria should be reported for follow-up and confirmation: 4th gen IA positive (Ag/Ab test) F/U antibody-only test is negative NAT (normally used to confirm results above) is unavailable Conclusion - case may be antigen positive/ antibody negative Proposed Revisions New HIV testing algorithms New: criteria for a suspect case HIV-2 infection Stage 0 HIV infection AIDS-defining conditions (opportunistic illnesses) CD4 test results for staging for adults/adolescents HIV Case definition for children Physician-documented diagnosis- PDD (clinical , rather than laboratory criteria for a confirmed case) PDD - date of diagnosis HIV-2 Infection HIV case surveillance should accept as sufficient for diagnosis of HIV-2 infection: Positive initial test that can detect HIV-2 antibody (e.g., HIV-1/2 immunoassay) AND One or more of the following: • FDA-approved HIV 1/2 type-differentiating antibody test positive for HIV-2 and negative for HIV-1 or • Positive HIV-2 nucleic acid test (NAT) or • Positive HIV-2 Western blot/immunoblot (WB) and negative HIV-1 WB or • Diagnosis by CDC-recognized expert in WB interpretation if positive HIV-2 WB and positive or indeterminate HIV-1 WB Proposed Revisions New HIV testing algorithms New criteria for a suspect case HIV-2 infection Stage 0 HIV infection AIDS-defining conditions (opportunistic illnesses) CD4 test results for staging for adults/adolescents HIV Case definition for children Physician-documented diagnosis- PDD (clinical , rather than laboratory criteria for a confirmed case) PDD- date of diagnosis Stage 0 HIV Infection (slide 1) First confirmed positive HIV test (confirmed Ag/Ab positive or NAT) 180 days 30 days OR Negative or indeterminate HIV antibody test or negative/undetectable NAT/viral load Negative or indeterminate HIV antibody test followed by positive NAT Stage 0 HIV Infection (slide 2) Exceptions These criteria for Stage 0 do not apply to HIV-2 Stage 0 does not last >180 days after diagnosis date Stage 0 is excluded if first positive test was preceded by >60 days by evidence of long-standing infection: CD4 T-lymphocyte count <200 cells/µL Physician documented diagnosis Otherwise, Stage 0 criteria are independent of CD4 Tlymphocyte test results and take precedence over criteria for other HIV stages Expectations of Health Departments This Position Statement does not imply that we expect you to start obtaining all negative reports-clearly a problem for most/all of us Identifying an acute case will likely come from physicians or other testers and this definition is to allow us to capture these critically important cases Proposed Revisions New HIV testing algorithms New: criteria for a suspect case HIV-2 infection Stage 0 HIV infection AIDS-defining conditions (opportunistic illnesses) CD4 test results for staging for adults/adolescents HIV Case definition for children Physician-documented diagnosis- PDD (clinical , rather than laboratory criteria for a confirmed case) PDD - date of diagnosis AIDS-Defining Conditions (Opportunistic Illnesses [OIs]) (slide 1) OIs should be removed from criteria for Stage 3 (AIDS) in future staging among adults/adolescents, because CD4 data adequately substitute for OI data as criteria for Stage 3 More direct measure of immune system damage 95% of cases meet Stage 3 criteria based on CD4 results Most systems do not routinely collect OI data- expensive to collect AIDS-Defining Conditions (Opportunistic Illnesses [OIs]) (slide 2) OIs should be removed from criteria for Stage 3 (AIDS) in future staging among adults/adolescents, because OI data collected by routine surveillance are too incomplete to be useful for analyzing OIs Other projects and surveillance systems do a better job of collecting representative OI data than does routine HIV case surveillance (MMP) Eliminating OIs from staging will simplify surveillance AIDS-Defining Conditions (Opportunistic Illnesses [OIs]) (slide 3) OIs should be kept as criteria for Stage 3 in children because CD4’s are not being used as criteria for Stage 3 in children, but Whatever method was used to make an OI diagnosis should be accepted as sufficient for surveillance (eliminating requirement that some OIs be “definitively” diagnosed) Lymphoid interstitial pneumonia should be removed from the list because it is associated with moderate rather than severe immunodeficiency Proposed Revisions New HIV testing algorithms New: criteria for a suspect case HIV-2 infection Stage 0 HIV infection AIDS-defining conditions (opportunistic illnesses) CD4 test results for staging for adults/adolescents HIV Case definition for children Physician-documented diagnosis- PDD (clinical , rather than laboratory criteria for a confirmed case) PDD - date of diagnosis CD4 Test Results as Criteria for Staging in Adults/Adolescents CD4 count should take precedence over CD4 percentage as criterion for staging; CD4 percentage should be criterion only if CD4 count is missing Reasons: Clinicians consider CD4 count to have greater prognostic value than CD4 percentage Some studies show CD4 percentage has little effect on prognosis after adjusting for CD4 count CD4 percentage used as threshold between Stages 1 and 2 should be 26% instead of 29% (if data supporting this change are published) Other Staging Issues Use of term “AIDS” should be minimized in staging system (just call it “Stage 3”) Permit alternative applications of staging system: most severe stage experienced as of a particular date (for which changes in stage could be in only one direction--from less to more severe) stage at initial diagnosis stage based on most recent CD4 test results (for which changes could be in either direction, including from more to less severe); (excluding Stage 0 because not based on CD4 test results) Proposed Revisions New HIV testing algorithms New: criteria for a suspect case HIV-2 infection Stage 0 HIV infection AIDS-defining conditions (opportunistic illnesses) CD4 test results for staging for adults/adolescents HIV Case definition for children Physician-documented diagnosis- PDD (clinical , rather than laboratory criteria for a confirmed case) PDD - date of diagnosis HIV Infection Case Definition for Children For a diagnosis of HIV infection among children under 18 months of age, Remove 2008 case definition’s requirement of HIV-infected mother for • Definitive HIV infection and • Presumptive HIV infection because laboratory test results can be sufficient to make those diagnoses, but keep requirement of HIV-infected mother for indeterminate HIV infection, where required lab results are unavailable for definitive or presumptive diagnosis, and for determination of absence of HIV infection among perinatally HIV-exposed children Proposed Revisions New HIV testing algorithms New: criteria for a suspect case HIV-2 infection Stage 0 HIV infection AIDS-defining conditions (opportunistic illnesses) CD4 test results for staging for adults/adolescents HIV Case definition for children Physician-documented diagnosis- PDD (clinical , rather than laboratory criteria for a confirmed case) PDD - date of diagnosis Clinical Criteria for Confirmed HIV Case (Physician-Documented Diagnosis) (slide 1) If physician’s written statement says patient had positive result on a particular type of HIV test in a specific year (not stated to be only what patient said), then diagnosis should be considered laboratory-test-documented, not physiciandocumented (i.e., meets lab criteria, not clinical criteria) Clinical Criteria for Confirmed HIV Case (slide 2) If initial diagnosis is not laboratory-testdocumented, but physician’s note says patient has HIV infection (not stated to be only what patient said), and subsequent diagnosis is laboratory-test-documented or there is circumstantial evidence of HIV infection (with other explanations ruled out), such as • Receipt of HIV-related care (e.g., antiretrovirals, OI prophylaxis, repeated CD4 tests and viral loads) • CD4 count <350 cells/µL • OI diagnosis then initial diagnosis is physician-documented Date of Physician Documented Diagnosis Official date of diagnosis should be defined as: Date of diagnosis reported in physician’s note, even if inaccurate or inexact, not necessarily date on which note was written unless diagnosis date (year) was not reported in note However, all dates should be collected, including Diagnosis date reported by physician (not stated to be reported by patient) Diagnosis date stated to have been reported by patient Date note was written by physician Many thanks to CDC’s Richard Selik for all the work he did on this Position Statement: the initial writing and research, working with the workgroups which informed the decisions made at the February 2012 case definition consultation and on which this PS is based. Eve Mokotoff Contact Info Eve Mokotoff, MPH MokotoffE@michigan.gov (V) 313.876.4769 (0353) (C) 313.407.7761 HIV/STD/VH/TB Epidemiology Section Michigan Department of Community Health 1151 Taylor Room 211B Detroit, MI 48202