Somatoform disorders

Somatoform disorders
prof. MUDr. Hana Papežová, CSc.
Department of Psychiatry, First Faculty of
Medicine, Charles University and General
University Hospital in Prague
Characteristics
Somatic complains of major medical maladies without demonstrable peripheral organ disorder
Psychological problems and conflicts are important in initiating, exacerbating and maintaining the disturbance.
Physical and laboratory examinations do not explain the vigorous and sincere patients´complaints.
The morbid preoccupation interferes with and anxiety are frequently present and may justify specific treatment
Diagnostic guidelines
Somatization disorder F45.0
A definite diagnosis requires the presence of all of the following:
At least 2 years of multiple and variable physical symptoms with no adequate physical explanation has been found,
Persistent refusal to accept the advice or reassurance of several doctors that there is no physical explanation for the symptoms,
Some degree of impairment of social and family functioning attributable to the nature of symptoms and resulting behavior.
DSM- IV versus ICD
Somatization disorders appeared first in DSM-III.
Current diagnostic criteria (DSM-IV) are simplified and symptoms from each of four symptoms group (pain, 2
GIT, 1 sexual symptoms, 1 pseudoneurological ) are required.
Usually diagnosed in the primary care
Difficult when the patient forgets (represses) or refuses
(supresses) medically relevant information and critical events.
In contrast with current DSM IV the conversion disorder is assigned in ICD 10 to the cluster of dissociative disorders.
Differential diagnosis
Medical conditions multiple sclerosis, brain tumour, hyperparathyroidism, hyperthyroidism, lupus erythematosus
Affective (depressive) and anxiety disorders
–
1 or 2 symptoms of acute onset and short duration
Hypochondriasis - patient´s focus is on fear of disease not focus on symptoms
Panic disorder - somatic symptoms during panic episode only
Differential diagnosis
Conversion disorder - only one or two
Pain disorder one or two unexplained pain complaints, not a lifetime history of multiple complaints
Delusional disorders - schizophrenia with somatic delusions or depressive disorder with hypochondriac delusions, bizzare, psychotic sy.
Undifferentiated somatization disorder - short duration (e.g. less than 2 years) and less striking symptoms
Course of the illness
Chronic relapsing condition, the cause remains unknown
Onset from in adolescence to the 3th decade of life.
Psychosocial and emotional distress coincides with the onset of new symptoms and health care-seeking behavior
Clinical practice showed that typical episodes last 6 to 9 months with a quiescent time of 9 to 12 months..
Therapy and Prognosis
The somatization disorders considerably affects social life and working ability of patient.
Focus on management than treatment.
Management strategies undertaken
by primary care
Therapy and Prognosis
The major importance for successful management
Trusting relationship between the patient and one
(if possible) primary care physician
Frequent changes of doctors are frustrating and countertherapeutic.
Regularly scheduled visits every 4 or 6 weeks.
Brief outpatient visits - performance of at least partial physical examination during each visit directed at the organ system of complaint.
Therapy and Prognosis
Understand symptoms as emotional message rather than a sing of new disease
Avoid more diagnostic tests , laboratory evaluations and operative procedures unless clearly indicated
Set a goal to get selected somatization patients referral-ready for mental health care.
Group therapy (time limited, behavior oriented and structured group: peer support, improvement of coping strategies, perception and expression of emotions and positive group experience
Case history
52yrs, w.f.referred to general internist for back pain and multiple other complaints
Disabled from her job of machine operator
History of 10 operations, in 5 hospitals and 7 different physicians in last 2 yrs.
Physical examination: Obese, wearing transcutaneous el. nerve stimulation, cooperative, shows the various scars with certain enthusiasm.
Case history
Mental status examination :
Cooperative and pleasant, somewhat seductive, no pressure in her speech, euthymic, affect little shallow,no problems with discussing of intimate details of her life.
The remainder of MSE within normal limits.
Disallowing all back-related symptoms (some degeneration of vertebral bodies L2-5 revealed by spinal radiographs) positive for 8 pain symptoms: 2 sexual, 4
GIT, 2 pseudoneurological onset at 26 yrs.
Diagnosis of somatization illness made in the presence of comorbid medical condition.
Somatization disorder undifferentiated F45.1
Includes unspecified psychophysiological or psychosomatic disorder in patients whose symptoms and associated disability do not fit the full criteria for other somatoform disorders.
The treatment and the outcome however do not considerably differ.
Hypochondriac disorder F45.2
Characterised by a persistent preoccupation and a fear of developing or having one or more serious and progressive physical disorders.
Patients persistently complain of physical problems or are persistently preoccupied with their physical appearance.
The fear is based on the misinterpretation of physical signs and sensations.
Physician physical examination does not reveal any physical disorder, but the fear and convictions persist despite the reassurance.
Diagnostic guidelines
A definite diagnosis requires presence of both of the following criteria:
Persistent belief in the presence of at least one serious physical illness despite repeated negative investigations and examinations or persistent preoccupation with presumed deformity or disfigurement.
Persistent refusal to accept the advice and reassurance of several different doctors that there is no physical illness or abnormity underlying the symptoms.
Includes: Body dysmorphic disorder, Hypochondriasis,
Dysmorphophobia (non delusional), Hypochondriacal neurosis,
Nosophobia
DSM - IV and ICD - 10
In DSM IV criteria for hypochondriacal disorder are essentially the same as those of
ICD-10
Since DSM-I
In DSM-IV addition of poor insight during the current episode
Differential diagnosis
Ruling out organic disease , usually completed by the primary care physician.
Somatization disorder - in somatization disorder concern about symptoms indifference about diseas
x
the preoccupation with 1 or 2 physical illness persistent, no sex differences, no special familial context
Differential diagnosis
Signs of malingering - actually experienced symptoms reported rather simulate them.
Somatic delusions in psychotic disorders , depressive disorder schizophrenia and delusional disorders-the more serious disorders.
Anxiety and panic disorders-somatic symptoms of anxiety sometimes interpreted as signs of serious physical illness but the conviction of presence of physical illness do not develop.
Therapy and prognosis
To date no evidence-based treatment has been described.
The comorbid psychiatric symptom may facilitate the referral to psychiatrist and improve frequently the hypochondriasis
Otherwise patients strongly refuse the mental health care professionals and remain in primary health care.
Similar management and group therapy strategy as in somatization disorder may be useful.
Course of the illness
The illness is usually long-standing, with episodes lasting moths or years .
Frequently recurrences occurs after psychosocial distress and induce impairment in psychosocial functioning and work abilities. that approximately 50 % of patients show improvement , in other cases a chronic fluctuating course remain.
Higher socio-economic status, presence of other treatable condition, anxiety and depression, an acute onset, absence of personality disorder or comorbid organic disease predict better outcome .
Somatoform autonomic disorder F45.3
The somatoform autonomic disorder has been similar chronic relapsing condition as the somatisation disorder.
Patients report worse health than do those with chronic medical condition and their report of specific symptoms
If they meet the severity criteria is sufficient and need not to be considered legitimate by the clinician.
Somatoform pain disorders F45.4
Persistent severe and distressing pain that cannot be explained fully by a physiological process of physical illness.
It occurs in association with emotional conflicts or psychosocial problems.
Chronic pain - a way of seeking human relationship , attention and support
Sometimes dissipate when an accompanying psychiatric disorder is treated.
Somatoform pain disorders (2)
It has been always difficult to specify to which extend the chronic pain is associated with a given lesion.
The expression of chronic pain may vary with different personalities and cultures.
It has been clinically accepted that the patient is not malingering and the complaints about the extend of the pain are to be believed.
F50 Eating Disorders
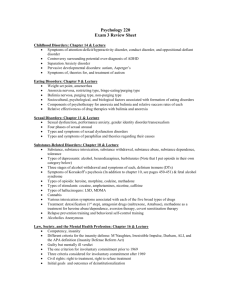
SPECTRUM OF EATING
DISOREDRS
OBESITY
BINGE EATING
BULIMIA RESTRICTING
BING-PURG. ANOREXIA
ANOREXIA
BODY WEIGHT
DRIVE TO EAT
IMPULSIVITY
IMPULSE INHIBITION
FOOD RESTRICTION
PERFECTIONISM
Risk Factors in Eating Disorders
Environmental
media images
teasing from peers
Family
maternal obesity and weight preoccupation
psychiatric disorders; substance abuse
Behavioral
personality and psychological factors
developmental model
Anorexia nervosa F50.0
a) Weight is maintained at least 15% below that expected
(either lost or never achieved) , or Quetelet´s body-mass index is 17,5 or less . Prepubertal patients fail to make the expected weigh gain during the period of growth.
b) The weight loss is self induced by diets, avoidance of
“fatting foods” and one or more following: self-induced vomiting, self induced purging, excessive exercise, use of appetite suppressant and/or diuretics.
c) There is body image distorsion in the form of a specific psychopathology with increasing emaciation the patient’s feeling to be too large persists and she imposes herself a low weight threshold.
Anorexia nervosa F50.0
Endocrine disorder of hypothalamic-pituitarygonadal axis, amenorhea in women men by lost of sexual interest and potency.
“masked” by hormonal replacement therapy
Elevated levels of growth hormone, cortisol, decrease thyroidal hormone and abnormalities in insulin secretion.
Prepubertal onset-delayed or stopped development on juvenile level (growth, breasts and the genitals).
Bulimia Nervosa F50.2
a) Persistent preoccupation with eating and an irresistible craving for food , the patients have the episodes of binge eating during which a large amounts of food are consumed in a short period of time.
b) The patient attempts to compensate the
“fattening” effect of consumed food by one or more following behaviour: self-induced vomiting, abuse of laxatives or diuretics, alternating periods of starvation, use of appetite suppressants, thyroid hormones or manipulation insulin( mainly in diabetic patients).
Bulimia Nervosa F50.2
c) The psychopathology consists of
1.morbid dread of fatness (the patient set herself or himself a sharply defined weight threshold below the premorbid weight that constitutes the optimum or healthy weight).
2.
frequent history of anorexia nervosa , the earlier episode may have been fully or mildly expressed (mild form with moderate loss of weight and/or a transient phase of amenorhea).
Eating disorders and the brain
BRAIN
EATING
BEHAVIOUR
BODY
Anorexia nervosa, Starvation
& the Brain
AN
PHYSICAL STATE
=
STARVATION
?
PSYCHICAL DISEASE
=
BRAIN ALTERATION
BRAIN ALTERATION STARVATION
Why? …nurture – does environment
matter?
perinatal factors family relationships life events
Studies with experimental starvation show that even healthy – not-predisposed – people can experience similar aspects of starvation.
Anatomy of CNS Brain atrophy I
Computed Tomography
Laessle et al 1989
AN (50) BN (50) COPP (50)
Krieg et al 1989
Brain atrophy III
WHITE MATTER
(myelinated axons, lipids)
• decreased in acute AN
• normal after recovery
GREY MATTER
(neural cell bodies)
• decreased in acute AN
• decreased after recovery!!
Katzman 1996, 1997, 2001; Lambe 1997
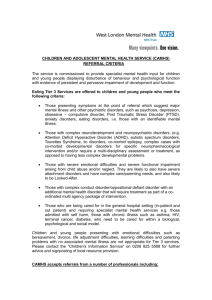
SENSORY IMPUT vision
VISUAL CORTEX
INTEGRATION
AMYGDALA
ASSOCIATIVE
LEARNING
DORSOLATERAL
PREFRONTAL CX
IMPULSE
INHIBITION smell
OLFACTORY
CORTEX taste
TASTE CORTEX
INSULA
FRONTAL
OPERCULUM
HYPOTHALAMUS
SENSING ENERGY
BALANCE
ORBITOFRONTAL
CORTEX
DECISION MAKING
REWARD VALUE
OUTPUT
BEHAVIOUR
INSULIN
LEPTIN
GHRELIN
BLOOD GLUCOSE
METABOLIC SIGNALS
The role of leptin in malnutrition
Circulating leptin levels are in most of the malnutrition states decreased in paralelle with drop of body fat
Hypoleptinemia is rather the consequence than the cause of anorexia nervosa and most of the malnutrition states
Hypoleptinemia triggers complex adaptive response to limited energy sources (
body fat). This adaptation includes decreased energy expenditure, amenorrhea, immunodeficiency etc.
Recovery
Relapse Contemplation
Precontemplation
MET
Stages of
Change
Model
Maintenance
Action
Preparation
CAT
CBT for the eating disorders
Making links between behaviour, cognitions and affect
Cognition
(e.g. gaining weight)
modifying these in parallel
Behaviour
(e.g.food avoidance)
Emotions
(e.g.anxiety, disgust)
Prevention
Increase knowledge
Promote acceptance
Diversity & puberty
Nature of eating d/o
Discourage dieting
Reduce teasing
Media literacy
Self acceptance
Increase self esteem
Coping strategies
Reduce body dissatisfaction
Healthy eating
Limit internalization