Length of Need - Aeroflow Healthcare
advertisement

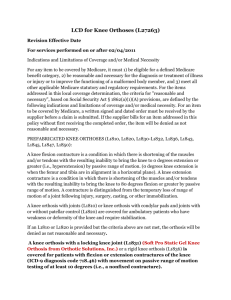
AEROFLOW HEALTHCARE TOLL FREE FAX# 1-800-249-1513 PATIENT #: CERTIFICATE OF MEDICAL NECESSITY FOR HINGED KNEE BRACE HIC#: PATIENTS NAME: STREET ADDRESS: PATIENT TELEPHONE: PATIENT DOB: ===================================================================================== ORDERING PRACTITIONER: ADDRESS: TELEPHONE: PRACTITIONER NPI: ===================================================================================== What is the patient’s Diagnosis Code? 714.0 - Rheumatoid Arthritis 717.0 - Meniscal Cartilage Derangement 717.81 - Knee Ligamentous Disruption 733.49 - Asceptic Necrosis of Tibia or Fibula 821.20 - Fracture of Femur-Lower End 823.00 - Fracture of Tibia or Fibula-Upper 844.0 - Sprain & Strain of Knee 715.16 - Osteoarthritis 717.7 - Chrondromalacia of patella 727.65 - Rupture of quadriceps tendon 733.16 - Pathologic fracture of Tibia/fibula 733.93 - Stress fracture of Tibia/fibula 836.0 - Dislocation of Knee Other:______________________________ Please Select the Product Prescribed and the knee(s) with the medical need: L1832 – Hinged Knee Brace – Rigid support orthosis with adjustable joints Right Left Both L1820 – Sleeve Knee Brace – Elastic and condylar pads and joints Right Left Both Describe why this patient requires the product prescribed above: To reduce pain by restricting mobility of the knee joint. To facilitate health and reduce pain following an injury to knee or related soft tissues. To facilitate health and reduce pain following a procedure on the knee or related soft tissue. To otherwise support weak upper or lower leg muscles/joints and/or a deformed knee joint. Other: ______________________________________________________________ ***Medical justification must be documented in the patient’s medical record*** BY SIGNING BELOW, I AUTHORIZE the use of this document as a legal prescription and I certify that the above prescribed equipment is medically necessary and reasonable, and is consistent with the current standards of medical practice and treatment of this patient’s condition. I will maintain an original, signed copy of this physician order in my medical records and make it available to Medicare, their authorized agents, or other insurer, if required. Order Date:_______________________ Length of Need: _______ months (99 mos. = lifetime need) Signature:___________________________________________ (NO SIGNATURE STAMPS) Signature Date:_________________