The U.S Health Care Paradox: Why Spending More is Getting Us Less
advertisement

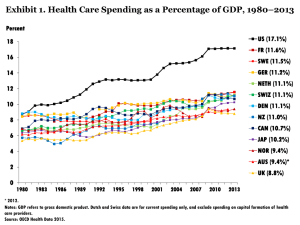
The American Health Care Paradox: Why Spending More is Getting Us Less 1 Outline Unraveling the paradox Recurrent themes from service US providers and users Learning from abroad Homegrown innovations here in the US 2 The Paradox “THEN THERE’S THE PROBLEM OF RISING COST. WE SPEND ONE AND A HALF TIMES MORE PER PERSON ON HEALTH CARE THAN ANY OTHER COUNTRY, BUT WE AREN’T ANY HEALTHIER FOR IT.” - JOINT SESSION OF CONGRESS ON HEALTH 9/9/09 3 High Spending on Health Care $9,000 $8,000 $7,990 $7,000 $6,000 $5,000 $4,000 $3,000 $5,348 $5,135 $4,225 $3,711 $3,379 $3,252 $3,035 $2,000 $1,000 $923 $0 Per capita data downloaded from OECD.StatExtracts. Available at stats.oecd.org 4 US Poor Ranking among 34 OECD Countries 35 30 31st 25th 26th 28th 25 20 15 10 5 0 Maternal Mortality Life Expectancy Low Birth Weight Infant Mortality Source: OECD, Health at a Glance 2009: OECD Publishing 5 What could help explain this paradox? 6 Incorporating Social Service Spending 35 30 25 20 Total Social Service Expenditures 15 10 5 Total Health Service Expenditures 0 7 In the US, for $1 spent on health care, about $0.55 is spent on social services In OECD, for $1 spent on health care, about $2.00 is spent on social services 8 Methods and Findings Using OECD pooled data from 1995-2007 on 29 countries, multivariable regression with 5 health outcomes The ratio of social to health spending was significantly associated with better health outcomes: - Less infant mortality, low birth weight, premature death; longer life expectancy - Non-significant for maternal mortality This remained true even when the US was excluded from the analysis Bradley et al., BMJ Qual and Safety 2011 9 Why do we do it this way? Health care and social service sectors grew up fairly independent from one another Health care grew professionalized and fit into a marketable, valued commodity for purchase Social services, in contrast, were conceived of “the poor” or aged and the target of charity 10 Recurrent Themes from Provider Interviews 1. Frontline personnel are stretched to respond to the concerns of service users with limited resources. 2. A more holistic approach was desired by both health care and social service providers. 3. Difficulties in establishing relationships between social services and health care have many roots. 11 Frontline Personnel Stretched I am sitting here writing a prescription [for] this person who has limited ability to afford the medication or have insight on the situation, who can’t go outside because the neighborhood is unsafe…and I am totally unable to do my job. -Internist We have a client who was hospitalized three times in 72 hours because they didn’t take the time to really look at what the problem was. They sent her home at midnight. The next morning before seven, an ambulance come to get her again. -Social Worker 12 More Holistic Approach is Desired What we do is an “all treaters” call -- everyone who is involved with the person, we will sit down at the table and discuss the person, what is the best care that we can give them….We can get three or four agencies working simultaneously side by side for one person; the key is communication and cooperation because if you don’t cooperate, it doesn’t get you anywhere. - Case manager 13 Many Barriers to Holistic Care - Lack of resources - Differences in cultural and professional norms - Technological and data limitations Even if you got past the privacy issues, it is very hard to tie in all of the information that was useful for the hospital based provider, the outpatient based provider, and social services to be able to capture what an individual is thinking or feeling at a given point in time, to know what intervention is necessary. -Social worker 14 User submitted comment The National Memo “…this thesis is starting to be accepted. You can see it in the models being rolled out in NY State…” Huffington Post “Rebalancing what we spend on medical care and social services can potentially deliver better health outcomes at lower cost. Cracking this code is a challenge that should concern us all.” Experience in Other High-income Countries 16 Conception of Health Your health means everything. - Winthrop University Hospital People should know that health is not the goal of life. But health is definitely a means that you can use to choose exactly the life you want because if you don’t have health, then your possibilities cannot flow and grow. -Danish Health and Medicines Authority Executive 17 Joint Planning and Budgeting It is a closed system where 80 percent of the decisions, even those they are decentralized, are made within the public integrated system. So…if one department…goes beyond its budget, somebody else will have to be below it. - Denmark, senior health policy analyst 18 Comparisons in Values (Scandinavia versus U.S.) World Values Survey, an international open source of empirical data measuring individuals’ values In-person surveys of about 1,000 randomly selected respondents in 55+ countries Data represent Sweden, Norway, and United States Differences (P<0.05) Scope of social contract Views of income, equality and social mobility Degrees of trust in “the other” 19 Is there any good news? 20 Homegrown Innovations • • • • • Public and private sector Non-profit and for-profit High and low-income clientele A range of business models Geographic diversity – New Haven, CT – New York, NY – Portland, OR Partnership between health care – Santa Monica, CA and social service providers TODAY 21 C-TRAIN (Portland, OR) • Academic medical center • 570-bed facility • 33% of patients are un- or under-insured • 501c3 serving Portland • Serving individuals and families facing homelessness, poverty and addiction • Affordable housing is primary service, plus health care, recovery services and employment assistance 22 C-TRAIN Leadership Dr. Honora Englander, Assistant Professor of Internal Medicine, OHSU These interdependencies between medical care and social determinants of health exist whether we want to acknowledge them or not… So I figured that if we’re not getting the outcomes we want by not acknowledging these interdependencies, maybe we should try something different. 23 The C-TRAIN Model Key features (1) Built on hospital emphasis on discharge planning (2) Assignment of a transitional nurse (3) Prescription assistance for patients (4) Sustained primary care at Central City Concern - Also access housing resources, insurance programs, financial and legal services etc. Outcomes RCT has found C-TRAIN patients experience lower mortality and improved quality of care; hospital is funding expansion 24 Project HEARTH at OPCC (Santa Monica, CA) • Part of Sisters of Charity Catholic Health System • 266-bed facility • Commitment to investing in community benefit programs • Over $33 million in community benefit spending in 209 TEAM PHOTO • 501c3 serving Santa Monica, est 1974 • 10 main services including homeless and domestic abuse shelters, addiction programs etc • Serves more than 8,000 individuals a year, 98% of whom fall below poverty line and 20% are <21 25 Project HEARTH Leadership Our population is really defined by this tri-morbidity, in terms of medical conditions, mental illness and then substance abuse. So we’ve really tried to integrate our response. John Maceri, Executive Director of OPCC 26 Bradley/Taylor: Inadequate attention to and investment in services that address the broader determinants of health is the unnamed culprit behind why the United States spends so much on health care but continues to lag behind in health outcomes. Pow! I can never consider U.S. macrohealth spending again and ignore this piece of the puzzle. - John McDonough, Boston Globe 27 Connect with the Authors Learn more at: theamericanhealthcareparadox.com Follow Betsy Bradley on Twitter @ehbyale Follow Lauren Taylor on Twitter @LaurenTaylorMPH 28 Thank You 29 But if we add in social service spending… 30 Washington Independent The flawed American health care system is not exclusively a problem of the “poor.” Those at greater risk in the system also include relatively isolated people at many income levels who lack supportive family and friends…these vulnerable people often call for an ambulance when what they really need is a shoulder to lean on and emotional support. Amazon review Spending on health care cannot be looked at without considering the investment in social services that impact public health. This is all too often missed. The consequence is that governments like the US spend more money on treatment...than on dealing with the underlying factors that cause those health issues in the first place. Final Thought This is work with a different set of values from the ones that medicine traditionally has had: values of teamwork instead of individual autonomy, ambition for the right process rather than the right technology, and, perhaps above all, humility—for we need the humility to recognize that, under conditions of complexity, no technology will be infallible. No individual will be, either. - Atul Gwande, The Velluvial Matrix 33