Neonatal Growth and Nutrition
advertisement

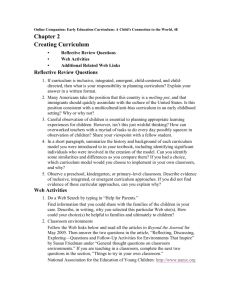
Promotion of normal growth rate, organ development, and body composition Prevention of later disease — Obesity — Cardiac — Allergic — Cancer Birth weight triples by 1 year, but does not quadruple until age 2 Birth length increases by 50% in year 1, but does not double until age 4 After age 2, children average 2 -3 kg and 6 - 8 cm of growth per year Serve as a guide for estimating nutrient need DRIs recently revised for specific childhood ages (Institute of Medicine) Much of the data are extrapolated from adult, but increasingly more specific Since they are group recommendations, they include a margin of safety The Two Factors Which Contribute to Childhood Malnutrition POVERTY IGNORANCE Children after the age of 1 are largely unprotected because — Programs are much less specific regarding nutrient requirements compared with < 1 year — A child’s diet and an adult diet are similar; thus, children can be shortchanged in a general assistance paradigm Willful or unwitting ignorance by parents may contribute to nutritional imbalances: — Parent allowing child to choose foods leading to unbalanced diet — Parent willfully manipulating diet without consideration for balance and nutrient needs » » Imposition of adult diet on young child Fad foods/”nutriceuticals” Vary considerably among children Dependent on: — Basal metabolic rate — The Barker Hypothesis & Fetal “Programming” — Growth rate — Physical activity — Body size Range from 1000 Kcal/d at 1 year to 2200 Kcal/d at 12 years Absorption of amino acids increases protein synthesis in children (unlike adults) The body is unable to store excess dietary amino acids — Uses them for energy production if energy intake is low — Or converts them to glucose or fat if energy intake is adequate (Continued) Daily protein requirement ranges from 12 grams at 1 year to 35 grams at 12 years Note that protein requirements during childhood are low compared to newborn or teen — Growth rates are slower — Tissue synthetic rates are slower Amino acid needs for growth decrease from 56% of total intake at birth to 5% at 5 years The DRIs are largely extrapolated from infant or adult data Exceptions are for energy, protein and iron where balance studies have been performed (Continued) Minerals/elements that are likely to be low in the diet of young children — Calcium » Crucial for preteen girls re: future osteopenia — Iron — Zinc — Magnesium Healthy, growing children consuming a varied diet do not need vitamin supplementation Children at nutritional risk who may benefit from vitamin supplementation — Those from deprived, neglectful or abusive families — Those consuming fad diets — Those with chronic disease, particularly affecting the GI tract — Those on dietary programs for managing obesity — Those on vegetarian diets without adequate dairy products Protein, energy and protein-energy malnutrition — Endemic areas include sub-Saharan Africa Iron deficiency — World-wide for various reasons » » Intestinal blood loss (parasitic) in developing countries Inadequate intake (cow’s milk) in developed countries Vitamin A deficiency Obesity — Begins generally after the age of 2 - do not restrict dietary fat before this age — 30% of children are obese: rate is increasing — Childhood obesity is not generally “outgrown” — Growth adiposity rebound between 5 and 7 years is critical in predicting adult obesity » Early rebound more predictive of later obesity GIRLS 2 - 18 yrs Obesity (continued) — Young children will not innately choose a wellbalanced diet unless appropriate foods are presented and models of food acceptance given — Parents and school lunch programs must provide nutritious foods at regular meals and snacks, and allow the children to decide how much they eat — Children do best 4-6 times a day with relatively low volume foods » Snacks should be considered normal meals Obesity (continued) — The influence of advertising should not be underestimated » 50% of television advertising is for foods (higher in children’s programs) » Most foods shown on TV are high in fat, sugar and salt (e.g., sweetened cereal, fast foods, snack products, candy) » TV messages have primarily emotional/psychological appeal — Physical inactivity likely plays the largest role in childhood obesity Iron Deficiency: 6-13% — Children at risk due to low iron stores at birth (up to 250,000 per year) » Growth-retarded infants » Infants of diabetic mothers — Children at risk due to inadequate intake » Early introduction of cow’s milk (before 12 months) » Unsupplemented infant formula (up to 30% of sales) » Breastfeeding without iron supplementation (20% at 9 months — Children with increased GI blood loss Vary significantly based on gender and age DRIs for males — 13 - 15 years old: 2000 Kcal/d — 16 - 18 years old: 3200 Kcal/d DRIs for females* — 13 - 15 years old: — 16 - 18 years old: *add 2200 Kcal/d 2100 Kcal/d 300 Kcal for pregnancy; 450 Kcal for lactation Second peak of protein accretion during childhood — Associated with significant growth spurt DRIs for males — 11 - 14 years (pre-growth spurt): 45 g/d — 15 - 18 years (growth spurt): 59 g/d Nutrient Gender Increment Increment (average) (peak of growth spurt) Suggested Calcium M F 210 110 400 240 1100 1200* Iron M F 0.57 0.23 1.1 0.9 10 13** Zinc M F 0.27 0.18 0.50 0.31 12 9 All values are mg/d * to increase bone mineral stores * increased iron turnover due to menses Onset of puberty in both sexes increases: — Energy needs for increased physical activity — Protein needs for rapid skeletal growth — Calcium needs for bone mineralization Onset of menstruation in girls increases: — Iron demand to replace blood loss and match expanding blood volume — Calcium need to protect against later osteopenia Low energy intake (dieting) creates difficulties in obtaining adequate levels of micronutrients Replacement of milk (or other high-calcium foods) with soft drinks, coffee, etc., results in a low calcium intake associated with a high protein intake — leads to negative calcium balance and increased risk of osteoporosis High iron requirements to sustain rapidly expanding blood volume and lean body mass and to offset menstrual losses in females are frequently not met; iron deficiency is particularly prevalent in female athletes Positive zinc balance is essential for adolescent growth; zinc deficiency is characterized by growth failure, hypogonadism, decreased taste acuity; increased prevalence in Middle East Vegetarian diets without eggs and milk lead to vitamin D and B12, riboflavin, protein, calcium, iron and zinc deficiency; adolescents on vegan diets must learn to assess protein quality and balance Obesity, often carried over from preteen years, becomes worse with poor quality snacks, limited food choice and frequent eating away from home Nutritional issues in childhood and adolescence differ in developing and developed countries The antecedents of adult diseases are found in childhood nutritional disorders Obesity Allergy ?Cancer